

Abstract
Hepatitis C virus (HCV) is an important health care problem in haemodialysis. Hepatitis C virus is both a cause and complication of kidney diseases. Yet there are limited information on antibody against HCV in patients on haemodialysis. The purpose of this study was to determine the prevalence of anti-HCV and the risk factors associated with HCV infection in a cohort of 100 participants on haemodialysis. They were consecutively recruited into the study, anti-HCV testing was made by the 3rd-generation ELISA System (C-100, C-33c, C-22). The prevalence of HCV antibody was 15%, risk factors associated with HCV antibody were history of blood transfusion and duration of session of haemodialysis; the risk increased with increased with the number of blood transfusion and seasons of haemodialysis. The observed high prevalence of HCV antibody among patients on haemodialysis reflect the quality of healthcare services and the standards of infection control practices in our haemodialysis units. Routine screening for HCV should be done before blood transfusion using third generation ELISA assays with high sensitivity and specificity. Safety measures should be taken in our haemodialysis units to prevent cross infection among patients and staffs. These safety measures include; discarding syringes, needles, gloves, bloodlines and dialysers after single use, and the use of sterile dressings on each patient visit.
Keywords: HCV, haemodialysis, risk factor, transfusion
Introduction
Hepatitis C virus (HCV) is a significant cause of morbidity and mortality among chronic renal failure patients due to their inability to clear the virus efficiently [1]. Patients on haemodialysis dependantant on blood transfusion instead of erythropoietin to reverse anemia are at particular risk of acquiring HCV as it is easily transmissible through blood and blood product [2–4]. Other factors reported to favour HCV acquisition among patients on dialysis include cross infections from the sharing of dialysis machines and the dialysis equipment, the reprocessing of dialyzers and blood lines and the increased requirement of blood transfusions [5, 6]. Studies have reported a significant association between the dialytic age and anti-HCV positivity; dialytic age has been shown to be predictor for the risk of the acquisition of the HCV infection [5–7]. Furthermore, although repeated dialysis increases the risk of contracting HCV, there is no risk through the equipment used in dialysis [8]. The prevalence of HCV is less prevalent in developed countries due to socioeconomic factors, better infection control measures, use of erythropoietin instead of blood transfusion to treat anemia [9]. Conversely the prevalence of hepatitis C virus infection is expected to be high in developing countries especially in patients with chronic kidney disease because of exposure of these individuals to multiple risk factors such as blood transfusion and haemodialysis. Unfortunately information on the risk factors of HCV among renal failure patients is sparse in Nigeria. To the best of our knowledge, no study has reported the risk factors associated with HCV acquisition in our environment. We therefore set out to determine the risk factors associated with contracting HCV among patients on Haemodialysis receiving care at a kidney centre attached to tertiary health institution in Maiduguri, Nigeria.
Methods
This cross sectional analytic study considered one hundred consecutive patients with stage 5 chronic kidney failure. Participants were either recruited at kidney centre or on medical wards of the University of Maiduguri Teaching Hospital. Patients were subsequently examined. Patient's demographic data including age and sex, were recorded. Risk factors, clinical features, possible aetiology of chronic kidney failure, and laboratory data were obtained by the use of questionnaire. Blood samples were obtained at entry for creatinine clearance, serum electrolytes, urea, and creatinine, including serum calcium and phosphate, liver function tests, HIV screening, Anti-HCV testing was made by the 3rd generation ELISA System (C-100, C-33c, C-22), HbsAg and full blood count (FBC). Abdominal ultrasound scan was also done on all the patients. Case definition of patients with stage 5 chronic Kidney failure i.e eGFR <15 ml/min was based on the estimated glomerular filtration rate (eGFR) by Cockroft-Gault equation [10]. All data were collected and statistical analysis was performed using Epi Info 2002. Chi-square test & Fisher's exact test were used for comparing categorical variables. A probability of less than 0.05 was considered statistically significant. Permission to conduct this study was obtained from research and ethics committee of University of Maiduguri Teaching Hospital. Informed consent was obtained from all patients.
Results
Sociodemographic characteristics
The participants consisted of 68 (68%) males and 32(32%) females, with most of them in 3rd and 4th decade of life. Their ages ranged between 15 and 74 years with a mean (± SD) of 39.9 ± 13.58 years. Males with mean age (± SD) of 41.71 ± 13.27 were older than females that had mean age (± SD) of 36.06 ± 13.64 years. Majority of the participants, 79 (79%) were in stable marriage union, while 21(21%) were single. The age and sex distribution of the studied participants is as depicted in Table 1. Most of the patients (32%) had secondary education followed by tertiary education in (31%). Thirty patients (30%) had non-formal education whereas 7 (7%) had primary education. Figure 1 shows the educational status of the patients. Majority of the study subjects (36%) were unemployed. Semiskilled workers followed with 27%. Twenty-three percent of the study patients were professionals while 14% were artisans as shown in Figure 2.
Table 1.
Age and sex distribution
| Age (years) | males, no(%) | females, no(%) | Both, no(%) |
|---|---|---|---|
| ≥19 | 03(3%) | 03(3%) | 06(6%) |
| 20-29 | 09(9%) | 08(8%) | 17(17%) |
| 30-39 | 17(17%) | 07(8%) | 24(24%) |
| 40-49 | 20(20%) | 09(9%) | 29(29%) |
| 50-59 | 11(11%) | 03(3%) | 14(14%) |
| 60-69 | 06(6%) | 02(2%) | 08(08%) |
| ≥70 | 02(2%) | - | 02(02%) |
| Total | 68(68%) | 32(32%) | 100(100%) |
Figure 1.
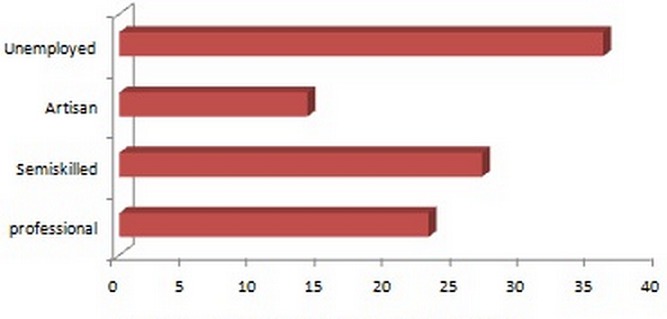
Proportion (%) of participants by occupation
Figure 2.
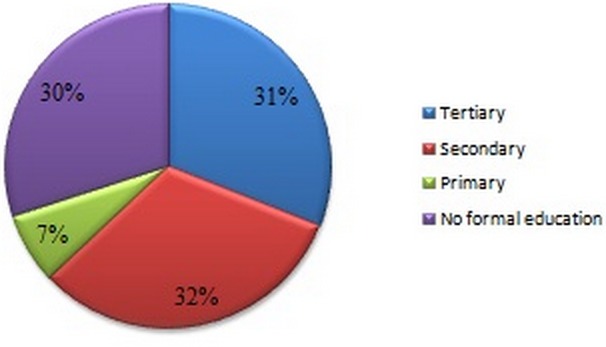
Distribution of participants by educational status
Risk factor for hepatitis C virus infection
We sought to determine the risk factors for HCV infection in our study population. The prevalence of HCV among our studied cohort was 15 (15%). Fifty five (55%) of the patients had no identified risk factor for HCV infection. A total of 33 (33%) patients had received blood transfusion, 17 (17%) of these patients had blood transfusions alone; 15 (15%) had received blood transfusions and were on haemodialysis as well. One patient was a haemophilic and had received blood transfusions. Of the 33 patients who received blood transfusion, 10 (10%) tested positive for HCV antibodies. When taking into consideration the 33 patients who received blood transfusion, it could be seen that 26 patients received 1-5 units of blood and among whom 3 patients were positive for HCV abs. While the 2 patients who received 6-10 units of blood and the 5 patients who received =11 units of blood were all positive for HCV abs. Blood transfusion therefore was found to be an important risk factor for HCV infection with a p value of 0.0000. Taking the risk of HCV through haemodialysis into account, patient that had ≥ 10 sessions were all negative for HCV abs, while the 2 patients who had ≤11 sessions were positive for HCV antibody. Haemodialysis was also found to be a risk factor for HCV infection with a p value of 0.0095. Evaluation of the risk factors of HCV antibody is as presented in Table 2.
Table 2.
Risk factor for HCV among the participants
| Risk factor | HCV negative | HCV positive |
|---|---|---|
| Blood transfusion | ||
| 1-5 units | 23 | 03 |
| 6-10 units | - | 02 |
| ≥11 units | - | 05 |
| Total | 23 | 10 |
| Fisher's exact test, p = 0.0000 | ||
| Haemodialysis | ||
| 1-5 sessions | 12 | - |
| 6-10 sessions | 01 | - |
| ≥11 sessions | - | 02 |
| Total | 13 | 02 |
| Fisher's exact test, p = 0.0095 | ||
| Health worker | ||
| 1-10 years | 03 | - |
| 10-20 years | 01 | - |
| ≥20 years | - | 02 |
| Total | 04 | 02 |
| Fisher's exact test, p = 0.07 | ||
| Intravenous drug abuse | ||
| 1-5 years | 03 | - |
| 6-10 years | - | 01 |
| ≥ 11 years | - | 02 |
| Total | 03 | 03 |
| Fisher's exact test, p = 0.10 |
Discussion
The point prevalence of HCV antibody of 15% among patients on haemodialysis in this study is alarmingly high in comparision to 1.4% among prospective blood donors earlier reported in our environment [11]. The observed high prevalence of HCV infection among the patients on haemodialysis reflect the quality of healthcare services and the standards of infection control practices in haemodialysis unit. The prevalence among blood donors may be presumed to reflect the general population as they are exposed to similar risk as the general population. Several studies have identified transfusion of blood and blood product as a significant risk factor for acquisition of HCV [3–7]. This proposition was corroborated in this report as we established blood transfusion as a major factor for HCV (p = 0.000). We also observed the risk to linearly increase with the number of transfusion (p =0.000). This is not surprising, as those who received multiple blood transfusions were more likely to receive transfusion of unscreened blood or to receive blood transfusion from centres that don't have facilities for HCV antibody detection, as such are likely to be positive. Conversely other studies documented that the number of transfusions did not correlate with the anti-HCV prevalence [8, 9, 12] which may be due, among other factors, to a bias of data collected on the number of transfusions and safety standard [8]. Although the mode of transmission of HCV in dialysis is yet to be fully elucidated. We identified association between increased sessions of haemodialysis with risk of HCV (p = 0.0000). Studies have shown that contamination of the ultrafltrate, fluid that is removed from the blood during the dialysis procedure might constitute a potential risk for HCV transmission. It is possible that HCV infection could be transmitted from patient to patient in haemodialysis units, infact epidemics have been reported in some haemodialysis units. Also a breach of the safety devices on the haemodialysis machine could lead to transmission of infection [6–9, 13, 14]. Health profession exposes hospital staff to various infections particularly those that have direct access to patients, body fluids and equipment. Studies by Thorburn et al [15], Thomas et al [16] and Neal et al [17] found health profession to be an important risk factor for HCV infection. We are unable to validate or refute this finding due to limited health workers in our study.
Limitations
Although we detected antibody against HCV using third generation ELISA assays with high sensitivity and specificity. We were unable to detect and estimate HCV-RNA using reverse transcription-polymerase chain reaction (RT-PCR).
Conclusion
The observed high prevalence of HCV antibody among patients on haemodialysis reflect the quality of healthcare services and the standards of infection control practices in our haemodialysis unit. Routine screening for HCV should be done before blood transfusion using third generation ELISA assays with high sensitivity and specificity. Safety measures should be taken in our haemodialysis units to prevent cross infection among patients and staffs. These safety measures include; discarding syringes, needles, gloves, bloodlines and dialysers after single use, and the use of sterile dressings on each patient visit.
Acknowledgments
We thank patients for consenting to take part in this study, also the staff working at the kidney centre for their understanding and co-operation with us.
Competing interests
The authors declare no conflict of interest.
Authors’ contributions
All authors have read and agreed to the final version of this manuscript and have equally contributed to its content and to the management of the case.
References
- 1.Pol S, Vallet-Pichard A, Corouge M, Mallet VO. Hepatitis C: epidemiology, diagnosis, natural history and therapy. Contrib Nephrol. 2012;176:1–9. doi: 10.1159/000332374. [DOI] [PubMed] [Google Scholar]
- 2.Alashek WA, McIntyre CW, Taal MW. Hepatitis B and C infection in haemodialysis patients in Libya: prevalence, incidence and risk factors. BMC Infect Dis. 2012 Oct 20;12:265. doi: 10.1186/1471-2334-12-265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Morikawa T, Nakata K, Hamasaki K, Tsuruta S, Kato Y, Nakao K, Ohtsubo T, Eguchi K. Prevalence and characterization of hepatitis C virus in hemodialysis patients. Intern Med. 1999 Aug;38(8):626–31. doi: 10.2169/internalmedicine.38.626. [DOI] [PubMed] [Google Scholar]
- 4.Niu MT, Coleman PJ, Alter MJ. Multicenter study of hepatitis C virus infection in chronic hemodialysis patients and hemodialysis center staff members. Am J Kidney Dis. 1993 Oct;22(4):568–73. doi: 10.1016/s0272-6386(12)80930-9. [DOI] [PubMed] [Google Scholar]
- 5.Salama G, Rostaing L, Sandres K, Izopet J. Hepatitis C virus infection in French hemodialysis units: a multicenter study. J Med Virol. 2000 May;61(1):44–51. [PubMed] [Google Scholar]
- 6.Jaiswal SP, Chitnis DS, Naik G, Artwani KK, Pandit CS, Salgia P, Sepaha A. Prevalence of anti-HCV antibodies in central India. Indian J Med Res. 1996 Aug;104:177–81. [PubMed] [Google Scholar]
- 7.Hardy NM, Sandroni S, Danielson S, Wilson WJ. Antibody to hepatitis C virus increases with time on hemodialysis. Clin Nephrol. 1992 Jul;38(1):44–8. [PubMed] [Google Scholar]
- 8.Okuda K, Hayashi H, Kobayashi S, Irie Y. Mode of hepatitis C infection not associated with blood transfusion among chronic hemodialysis patients. J Hepatol. 1995 Jul;23(1):28–31. doi: 10.1016/0168-8278(95)80307-6. [DOI] [PubMed] [Google Scholar]
- 9.Kalantar-Zadeh K, McAllister CJ, Miller LG. Clinical characteristics and mortality in hepatitis C-positive haemodialysis patients: a population based study. Nephrol Dial Transplant. 2005 Aug;20(8):1662–9. doi: 10.1093/ndt/gfh895. [DOI] [PubMed] [Google Scholar]
- 10.Cockcroft D, Gault M. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31–41. doi: 10.1159/000180580. [DOI] [PubMed] [Google Scholar]
- 11.Denue BA, Ajayi BB, Abja AU, Bukar AA, Akawu C, Ekong E, Alkali MB. Survey of Prevalence of Hepatitis B and C in a tertiary health institution in northeastern Nigeria. International Journal of Medicine and Medical Sciences. 2012;4(1):13–18. [Google Scholar]
- 12.Medin C, Allander T, Roll M, Jacobson SH, Grillner L. Seroconversion to hepatitis C virus in dialysis patients: a retrospective and prospective study. Nephron. 1993;65(1):40–5. doi: 10.1159/000187438. [DOI] [PubMed] [Google Scholar]
- 13.Hayashi J, Nakashima K, Kajiyama W, Noguchi A, Morofuji M, Maeda Y, Kashiwagi S. Prevalence of antibody to hepatitis C virus in hemodialysis patients. Am J Epidemiol. 1991 Sep 15;134(6):651–7. doi: 10.1093/oxfordjournals.aje.a116137. [DOI] [PubMed] [Google Scholar]
- 14.Schlipköter U, Gladziwa U, Cholmakov K, Weise A, Rasshofer R, Lorbeer B, Luz N, Deinhardt F, Roggendorf M. Prevalence of hepatitis C virus infections in dialysis patients and their contacts using a second generation enzymed-linked immunosorbent assay. Med Microbiol Immunol. 1992;181(3):173–80. doi: 10.1007/BF00202057. [DOI] [PubMed] [Google Scholar]
- 15.Thorburn D, Dundas D, McCruden EA, Cameron SO, Goldberg DJ, Symington IS, Kirk A, Mills PR. A study of hepatitis C prevalence in healthcare workers in the West of Scotland. Gut. 2001 Jan;48(1):116–20. doi: 10.1136/gut.48.1.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Thomas DL, Factor SH, Kelen GD, Washington AS, Taylor E, Jr, Quinn TC. Viral hepatitis in health care personnel at The Johns Hopkins Hospital: The seroprevalence of and risk factors for hepatitis B virus and hepatitis C virus infection. Arch Intern Med. 1993 Jul 26;153(14):1705–12. [PubMed] [Google Scholar]
- 17.Neal KR, Dornan J, Irving WL. Prevalence of hepatitis C antibodies among healthcare workers of two teaching hospitals Who is at risk? BMJ. 1997 Jan 18;314(7075):179–80. doi: 10.1136/bmj.314.7075.179. [DOI] [PMC free article] [PubMed] [Google Scholar]