
Table 1.
Demographic and clinical features of patients with CHD and PHEO-PGL
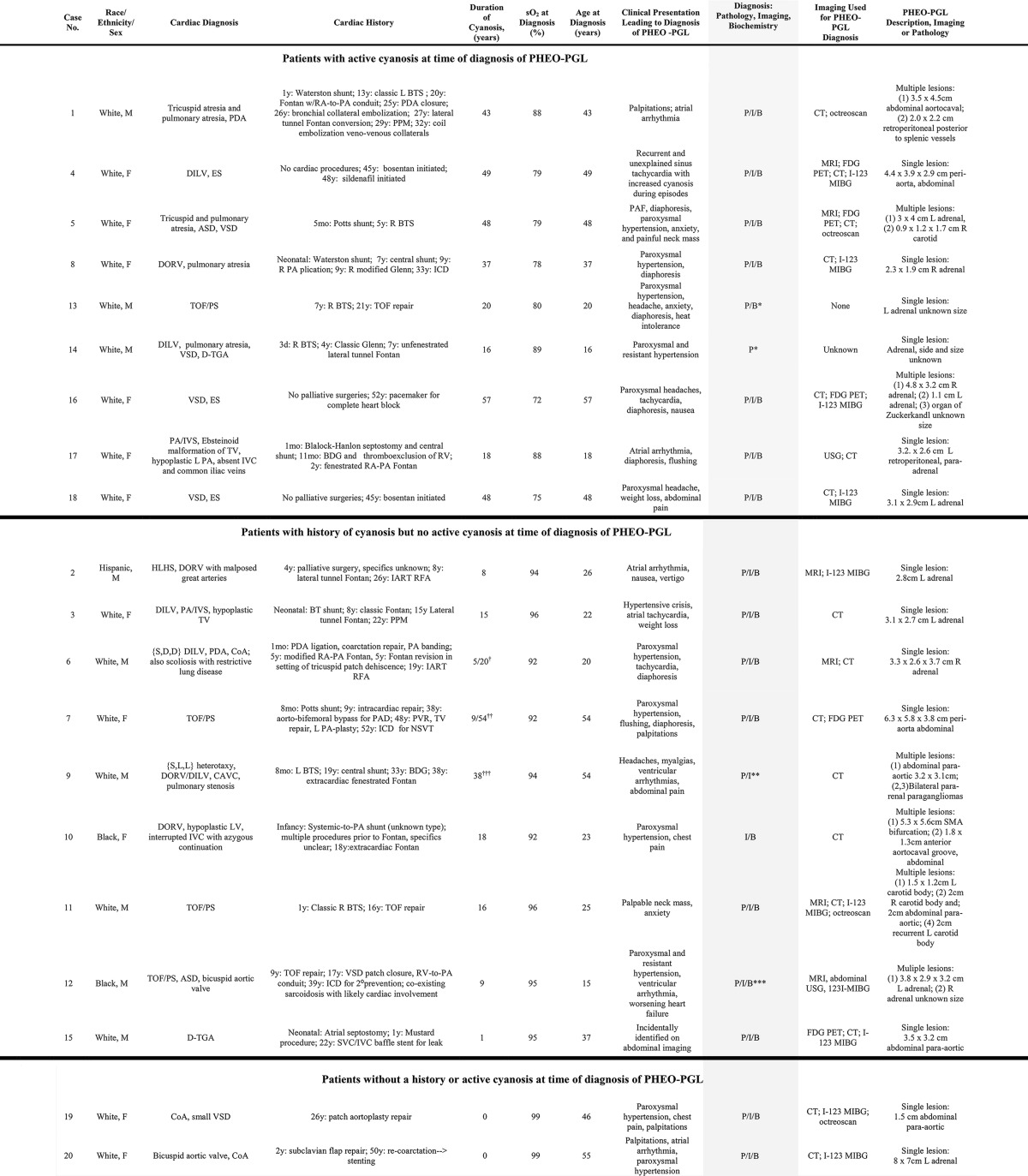
Abbreviations: ASD, atrial septal defect; BDG, bidirectional Glenn; BTS, Blalock-Taussig shunt; CAVC, complete atrioventricular canal defect; CoA, coarctation of the aorta; DILV, double-inlet left ventricle; DORV, double-outlet right ventricle; ES, Eisenmenger syndrome; FDG PET, 18-fluoro-deoxyglucose positron emission tomography; HLHS, hypoplastic left heart syndrome; IART, intraatrial reentrant tachycardia; ICD, implantable cardioverter defibrilator; I-123 MIBG, 123I-metaiodobenzylguanidine scintigraphy; IVC, inferior vena cava; L, left; PA, pulmonary artery; PAD, peripheral artery disease; PAF, paroxysmal atrial fibrillation; PA/IVS, pulmonary atresia, intact ventricular septum; PDA, patent ductus arteriosus; P/I/B, diagnosis by pathology, imaging, and biochemistry, respectively; PPM, permanent pacemaker; PVR, pulmonary valve replacement; R, right; RA, right atrium; RFA, ablation procedure; SVC, superior vena cava; TGA, transposition of the great arteries; TOF/PS, tetralogy of Fallot with pulmonary stenosis; TV, tricuspid valve; VSD, ventricular septal defect.
a Cases 13 and 14 underwent surgical resection of PHEO-PGL prior to presentation to the participating centers. Diagnosis of PHEO-PGL is based on available data that included primary information on biochemistry and pathology for case 13 but only historical documentation of consistency and confirmatory pathology for case 14.
b Severe cyanosis prior to Fontan. Documented resting saturations were 86%–92% between 10 and 20 years old.
c Severe cyanosis prior to TOF repair. Resting saturation was 92% in the decade prior to a PHEO-PGL diagnosis.
d Resting saturation after Fontan ranged from 91% to 94%, with exertional desaturation to a high percentage in the 80s.
e Diagnosis for case 9 was based on autopsy. An abdominal computed tomography scan performed shortly before the patient died suggested lymphadenopathy; PHEO-PGL was not suspected. The imaging findings suggestive of lymphadenopathy likely represented autopsy-documented paragangliomas.
f Diagnosis for case 12 differed for the two lesions. A left-sided pheochromocytoma was resected at age 15 years, with the diagnosis based on pathology. The right-sided lesion was diagnosed at age 31 years, and resection was pending at the time of data collection; the diagnosis for this lesion is based on imaging and biochemistry.