

Abstract
Background:
Nurses are members of the health care team for crisis response. Identifying nurses’ capability in responding to a disaster and promoting their preparedness will lead to effective use of human resources and decreasing the detrimental effects of disaster. The purpose of this article was to determine emergency nurses’ competences in triage, life support, and basic clinical skills in disaster response.
Materials and Methods:
This study was a descriptive study in which 40 emergency nurses were recruited by purposeful sampling. Moreover, their competencies in performing triage, life support, and basic clinical skills were evaluated by utilizing eight-station objective structured clinical examination (OSCE).
Results:
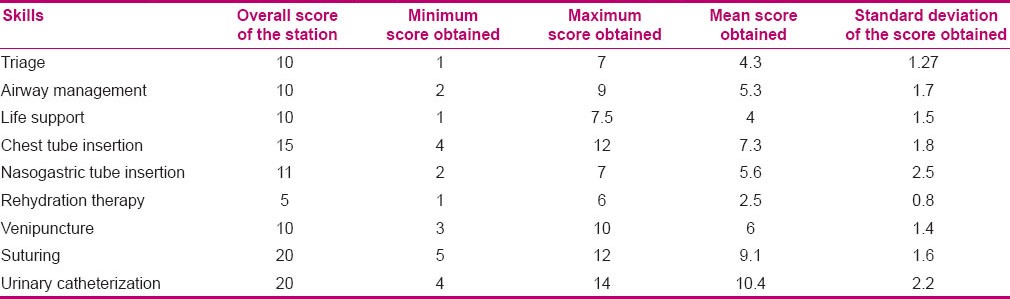
Our findings showed that the mean scores of nurses’ performance were: In triage (4.3 ± 1.27), life support (4 ± 1.5), airway management (5.3 ± 1.7), chest tube insertion (7.3 ± 1.8), nasogastric tube insertion (5.6 ± 2.5), IV therapy (2.5 ± 0.8), IV line insertion (6 ± 1.4), suturing (9.1 ± 1.6), and urinary catheterization (10.4 ± 2.2). No statistically significant correlation was found between demographic variables and nurses’ performance (P > 0.05).
Conclusion:
According to our findings, it can be concluded that competencies of nurses in performing triage, life support, and basic clinical skills were undesirable. Because emergency nurses are members of the emergency medical team, they should be prepared for disaster response via continuous training programs.
Keywords: Disaster response, nurses’ competencies, objective structured clinical examination
INTRODUCTION
Crisis has always threatened human societies.[1] The number and severity of crises have been increasing in the world; in the past 30 years, the number of natural and technological disasters has increased dramatically.[2] Factors such as excessive population, urban industrialization, climate changes, and spreading of infectious diseases with increased traveling and trading have increased the risk of crises and their effects.[3] In 2011, about 332 natural disasters were recorded in the world. Although it was less than the number recorded in the years 2001–2010, the human and economic impact of these crises had been far greater than in previous years. In 2011, Asia had the largest number of crises in the world and accounted for 86.3% of the reported victims.[4] In the most recent report by the Center for Epidemiological Crisis in 2012, Iran was not among the first 10 countries in terms of deaths caused by crisis, but between 1980 and 2010, about 1,376,263 people in Iran had been affected by natural disasters every year.[5] The existing reports showed that between 1970 and 2007, about 137,293 deaths and 70,996 damages had been reported following crises in Iran.[5] According to the Center for Epidemiological Crisis studies, during the period from 1900 to 2007, about 181 crises had been registered in Iran; also, there were 155,811 deaths, 168,217 injures, and 4,4037,516 disasters.[6]
The above figures indicate a high prevalence of crisis in Iran. Iran, being an accident-prone country and due to its geographic situation, is at risk of unpredictable events such as floods, earthquakes, drought, war, etc. Due to its climatic variation in important strategic situations, normal and abnormal events are observed. Therefore, it is important to address the topic of crisis in Iran. Due to there being a variety of disasters, it is necessary to be prepared to deal effectively with different types of crisis.[7] Preparation for an effective and timely response to incidents and natural disasters reduces the incidence of mortality and minimizes the amount of damage.[8] Conversely, the lack of preparation appropriate to the type and extent of impending crisis could have implications including loss of community abilities and resources for managing and coping with crisis.[9]
Nurses are important members of the crisis team. The main goal of nursing in crisis is to achieve the best possible level of health for the individuals and communities affected by the crisis.[10] Nurses are among the first people who are present at the site after an accident. Therefore, they need to be able to use their skills and take prompt action to provide the care necessary for the people involved in the accident, in order to prevent exacerbation of the problem and its complications.[11] Ensuring the clinical competence of nurses is essential for crisis intervention. Nurses should be aware of their limitations in knowledge, skills, abilities, independence, and self-efficacy before a critical disaster, so that they can play the effective expected role in these situations by the modification of these restrictions.[12] To ensure their reliability and assess their preparedness and skill, a measure is needed which could determine the degree of nurses’ competence to act in situations of crisis. The assessment of knowledge, skills, and abilities of nurses and identification of the existing gaps in their knowledge and skills, before participating in critical situations, can minimize the risks associated with crisis response.[13]
Competence is defined as the ability to manage critical situations or carrying out professional duties accurately. Clinical competence has a complex structure, including dynamic interaction between knowledge and performance. Assessment of clinical competence is essential in order to ensure the achievement of minimum professional standards and preparedness to perform their role.
Using the measures of competence not only leads to awareness and knowledge of nurses and managers relative to the general competency of nurses, but also identifies their deficiencies, and skill and cognitive deficits. Nurses can also gain awareness about their performances and identify their strengths, abilities, and areas that may require development and enhancement by using the process of rethinking.[14]
Although published articles and studies have partly explained the prevalence and significance of crisis, studies on the role of nurses, their skills and competencies in the emergency units, their role in crises, and their response to these situations are very limited. The results of a study conducted in 2006 in Australia on the readiness of nurses as members of the crisis team indicated that the number of nurses who had practical preparedness, competence, and sufficient experience and could be held accountable in critical situations was limited.[15] Moreover, the study by Tracey et al. conducted in 2008 in Canada on emergency nurses’ perceptions of preparedness in facing crisis showed that nurses felt they lacked preparation in responding to vast crises. This feeling largely depended on their perception of crisis or previous exposure to crisis.[16]
Studies conducted in other countries indicate the need to prepare nurses and other health care personnel to provide care in critical situations.[17] Studies conducted in Iran by Khankeh et al. also indicated the lack of preparedness of health care providers, especially nurses, in responding to disasters.[18] Furthermore, given the lack of studies in the field of nursing practical preparedness assessment in different areas of response to crisis, the present study aimed to assess the competence of emergency unit nurses of Alzahra Hospital, Isfahan, Iran, in triage skills, life-saving measures, and basic clinical skills.
MATERIALS AND METHODS
This was a descriptive study conducted in 2012 evaluating the clinical competence of emergency unit nurses of Alzahra Hospital, affiliated to Isfahan University of Medical Sciences, in responding to crisis, by utilizing objective structured clinical examination (OSCE). The OSCE test was composed of eight test stations in this study. These test stations included three main skills of triage, airway management, and life support, and basic clinical skills including venipuncture and rehydration, suturing, nasal gastric tube insertion, urinary catheterization, and drawing fluid from the pleural space. There were also two rest stations among the test stations. The duration for each station was 10 min. Points for each station were determined based on the number of items intended for the checklist in each section. Each item was scored 0 (not at all), 0.5 (to some extent), or 1 (strong). The minimum score of the stations was zero. The maximum scores of the stations were: 40 points for airway management station and life support, 10 points for triage, 15 points for drawing fluid from the pleural space, 11 points for nasal gastric tube insertion, 5 points for hydrotherapy, 10 points for IV catheterizing, and 20 points for urinary catheterization. The sum of the scores in each of the checklists was divided by 3, and thus classified into weak, intermediate, and strong levels. To measure the performance of each individual in the stations, exclusive checklists were designed for the stations based on the standard guide and professional nursing books. Content qualitative validity method was used to assess their validity. It was revised and reformed during three sessions by an expert panel consisting of the research team and a number of emergency unit nurses who had the experience of providing care in critical situations and were supposed to participate as evaluators in conducting the OSCE. Based on the opinions of the expert panel, some items of the standard checklist were changed in order to facilitate the evaluation and some items were added. Then, the checklists were sent to five experts for evaluation and OSCE test. Comments were collected and the proposed amendments performed. To estimate the reliability of checklists, inter-rater reliability method was used and the correlation was estimated at 0.98. Scenarios for each station were designed by two experts in the field of crisis management who had a PhD in health and disaster and had experience in the management of critical situations. At different stations, based on the assessed skills, manikins were used.
To evaluate the performance of the individuals at each station, an evaluator was appointed prior to the test and explanations on how to complete the test were given to them during the test. The statistical population included all the nurses working in the emergency unit of Alzahra Hospital. After explaining the objectives of the study to them and obtaining their informed consent, 40 of them were enrolled in the study by census. First, the exam objectives, test methods, test schedule, their duties during the test, and the method of evaluating their performance at the stations were explained during a briefing. Then, they were divided into two groups of 20 each; one group was tested in the morning and the other in the evening.
On the day of the test, the test procedures, evaluation methods, and the evaluator's role were described again. The registration form was completed by the subjects. The test venue was organized in a way that the test subjects entered from one door and, after finishing the test, exited through another door, so that there was no contact between the examinees, those who were waiting to take the test, and those who had finished the test. Instructions were written on the door of each test station, and before entering each station, they were read by the subjects for 1 min. During performance of the required skill, the evaluator assessed the performance of the subjects by the checklist. Assessors did not give any advice on how to respond to the tests. After finishing the test, the test subject was moved to the next station.
Ethical considerations
Prior to the study, the approvals of the Research Ethics Committee of Isfahan University of Medical Sciences and the relevant authorities were obtained, and necessary arrangements were made. Objectives of the study, test methods, confidentiality of the personal information, and voluntary participation in the study were explained to the study subjects and their written consents were obtained.
Analysis of data
To analyze the data, SPSS for Windows (version 16; SPSS Inc., Chicago, IL, USA) was used. Analysis of data on the demographic characteristics of the subjects was done by mean and frequency tests. The level of nursing competence was determined by using mean and standard deviation. The relationship between demographic variables and the level of competence of nurses was examined by Pearson correlation coefficient.
FINDINGS
Findings regarding demographic characteristics showed that the subjects’ mean work experience was 9.7 years, 100% had BSc in nursing, the majority of subjects were single [52.5% (21)], and they had history of responding to earthquake crisis [17.5% (7)], flood [15% (6)], and providing care for victims of critical incidents in hospitals [85% (34)]. In addition, 92.5% (37 subjects) had no record of participation in disaster training exercises and only 2.5% (n = 1) had participated in in-service training courses for crisis care.
The findings of the study regarding mean scores of the study subjects’ performances in the skills of triage, airway management, and life support, and some basic clinical skills are summarized in Table 1. Results showed that nurses’ skills in airway management and life support were weak, and in performing triage, drawing fluid from the pleural space, nasal gastric tube insertion, rehydration therapy, IV catheterizing, suturing, and urinary catheterization, they had intermediate skills. Pearson and Spearman tests also showed no significant correlation between nurses’ performance scores at different stations and their demographic characteristics (P > 0.05).
Table 1.
The mean performance scores of study subjects in the studied skills utilizing objective structured clinical exam
DISCUSSION
This study examined the level of competence of nurses in emergency rooms, regarding basic clinical skills, triage skills, airway management, and dealing with life-saving measures. The findings showed that nursing competence in the majority of these skills was at an average level. The participants of this study, due to their employment in emergency wards, were the first people to respond to crisis, as members of the health care team, voluntarily or being called to the scene. Therefore, they might not be prepared for the performance of basic skills during the occurrence of an incident.
Regarding the experience of responding to crisis as a member of the care team, the findings of the study showed that almost one-third of the participants in the study had the experience of showing their skills in earthquakes or floods and 82% reported the experience of providing care to victims of critical incidents. Therefore, it was expected that the participants would have a good level of competence required in performing basic clinical skills, triage, or life support, but their competence was less than expected. In some previous studies, having experience caused the nurses to feel prepared in responding to crisis as a member of the care team. As an example, in the study by Suserud and Haljamae, half of the nurses with previous experience of crisis had reported that they were ready to provide care in crises, but nurses who previously had not experienced a crisis did not report feeling prepared.[19] However, in some previous studies conducted in developed countries, such as the study of Arbon et al. in Australia, a high percentage of nurses who volunteered to provide care in crises (80%) had no previous experience of providing care in critical situations.[15] Investigation of the experiences of nurses in their study suggested that nurses who work in hospital emergency wards can play an important role in emergency nursing and can perform skills such as triage and life support. Nurses who lack experience in this area will not be able to operate effectively in critical situations.[19] In the present study, despite having previous experience, the nurses did not perform well in the above skills. This contradiction was perhaps due to the fact that in this study, the nurses’ performance was objectively measured that showed their actual performance, whereas in the previous study, the nurses’ feeling of preparedness in providing care in crisis was assessed subjectively and by a self-report that could differ from their actual performance.
Despite having previous experience in the phase of crisis response, only 2.5% of the participants had attended in-service training related to crisis response, which was much less compared to studies in other countries. For example, in the study by Murray et al., 23% of the participating nurses received only primary education, 29% received in-service training, and 48% received both training methods.[20] In the study by Greenberg et al., 15.5% had participated in in-service training programs on emergency care.[21] A comparison of figures reported in previous studies with recent studies in other countries showed that in recent years, more attention has been devoted to the education of nurses in disaster response; however, this issue has received little attention in Iran. Meanwhile, in another study conducted in Iran, the experience of nurses in responding to crisis showed the need to update information and skills necessary for nurses in emergency care in the form of in-service training.[22]
One of the skills assessed in the present study was the skill to perform triage. The level of nursing competence in performing this skill was average and none of the participants were able to perform triage accurately. Meanwhile, in the experience of nurses in Sweden, the first action that was needed in response to crisis was to perform triage.[19] In the study by Slepski in America on the professional competencies required of nurses in the Katrina crisis, one of the greatest skills reported as required by nurses was the skill in performing triage. In this study, nurses had a high level of proficiency in performing triage and only 3% of them had reported the need for special training to perform triage.[23] This was inconsistent with the results of present study. Considering that in this study, 97.5% of nurses had not participated in any training related to nursing skills in crisis, this difference may be due to differences in the amount of training received by nurses in the two studies. However, in the last decade, countries like America had been planning more seriously on this issue and their nurses were able to obtain more skills in this area. Two other studies conducted in Iran indicate the lack of appropriate preparation of nurses for victims’ triage. For example, the study of Nasrabadi et al. conducted in Iran on the experiences of nurses in the earthquake in Bam reported the inability of nurses in performing triage.[22] Furthermore, Faraji et al. reported the mean of nurses’ skills and their accuracy in performing triage to be weak.[24] Studies in other developing countries also reported almost similar results. A study by Fung et al. in Hong Kung on the nurses’ preparedness to respond to crisis reported that a high percentage of nurses (58.5%) needed training for triage skills.[25] The study by Wolf and Everson on the competence of nurses in performing triage showed that 80% of nurses obtained 48–69% (moderate level) of the score. Literature indicated that nurses make decisions regarding triage on a daily basis. Thus, this skill is a necessity not only for emergency nurses but also for all clinical nurses.[26]
Other skills assessed in the present study were airway management skills and practices in life support. The findings of this study showed that nurses had a moderate level of competence in performing these skills. In the study by Suserud and Haljamae, the second important step in the experiences of nurses in response to crisis was supporting life.[18] Furthermore, Chapman and Arbon reported that cardiopulmonary resuscitation skills are not unique to critical situations and all nurses should be competent in performing them.[27] Fung et al. showed that the nurses had weakness in cardiopulmonary resuscitation and life-saving measures; 75% of the subjects required training in these two skills.[25]
Research findings regarding basic clinical skills, such as venipuncture, suturing, urinary catheterization, and fluid therapy, also showed moderate levels of competencies for nurses. In the study by Fung et al., 76.2% of the nurses reported feeling weak in performing basic clinical skills.[25] In the study by Slepski, the third skill required for nurses in response to crisis, after triage and proficiency in life-saving procedures, was reported to be basic clinical skills.[23] Overall, the findings of this study revealed the gaps in nurses’ skills in response to crisis, such as triage, basic clinical skills, and life-saving measures. This could be due to lack of receiving related training and performing practical skills during education course or in-service training. It is recommended that appropriate training programs, according to the practical needs of emergency nursing, be designed and nursing skills be periodically evaluated by simulated tests. One of the limitations of the current study was the small sample size. Therefore, it is suggested that similar studies with greater sample size be conducted to increase the generalizability of the study.
CONCLUSION
Nurses, as members of the medical team, should at least have the minimum necessary competency to act in response to crisis. Periodic assessment of professional competence of nurses can be a continual education guide for employees, in order to improve their competencies. Clinical skills in performing triage, life-saving measures, and basic clinical skills were assessed by utilizing an OSCE in the present study. As a result, it was indicated that emergency nurses and medical emergency nurses, despite having a history of work in emergency wards and the experience of past crises, did not have the maximum preparation in performing the above skills and during in-service training programs, no attention was paid to these skills. Considering the fact that Iran is among the countries with high occurrence of natural disasters, it is necessary that administrators of continuing education programs pay more attention to reinforcing these skills for all nurses, especially emergency unit nurses, by performing training courses. However, the findings of this study should be considered along with its limitations. First, the participating nurses were restricted to only one training hospital. Although the studied hospital was a specialized training center and generally nurses in the emergency ward had different rankings and were experienced, it is recommended that the research be replicated with a larger sample and in different centers.
ACKNOWLEDGMENT
The authors’ appreciation goes to the nurses who participated in this study for their cooperation.
Footnotes
Source of Support: The study was funded by both Isfahan University of Medical Sciences and Shahrekord University of Medical Sciences.
Conflict of Interest: The authors had no conflicts of interest.
REFERENCES
- 1.Brunsma D, Picou JS. Disasters in the Twenty-First Century: Modern destruction and future instruction. Soc Forces. 2008;87:983–91. [Google Scholar]
- 2.Veenema TG. Chemical and biological terrorism preparedness for staff development specialists. J Nurses Staff Dev. 2003;19:218–25. doi: 10.1097/00124645-200309000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Subbarao I, Lyznicki JM, Hsu EB, Gebbie KM, Markenson D, Barbara B, et al. A consensus-based educational framework and competency set for the discipline of disaster medicine and public health preparedness. Disaster Med Public Health Prep. 2008;2:57–68. doi: 10.1097/DMP.0b013e31816564af. [DOI] [PubMed] [Google Scholar]
- 4.Guha-Sapir D, Vos F, Below R, Ponserre S. Brussels: Centre for Research on the Epidemiology of DisastersCRED; 2012. Annual disaster statistical review 2011: The Numbers and Trends. [Google Scholar]
- 5.Brussels, Belgium: [Last accessed on 2013 Feb 05]. Centre for Research on the Epidemiology of Disasters 2012. EM-DAT: OFDA/CRED. Universitécatholique de Louvain. Available from: http://www.cred.be . [Google Scholar]
- 6.Peduzzi P, Chatenoux B, Dao H, De Bono U, Deichmann G, Giuliani C, et al. Davos: Extended summary for the International Disaster and Risk Conference IDRC; The Global Risk Analysis for the 2009 Global Assessment Report on Disaster. Risk Reduction. [Google Scholar]
- 7.Cooke MW, Brace SJ. Training for disaster. Resuscitation. 2010;81:788–9. doi: 10.1016/j.resuscitation.2010.04.026. [DOI] [PubMed] [Google Scholar]
- 8.Magnaye B, Lindsay Muñoz MS, Muñoz MA, Muñoz RG, Muro JH. The Role, Preparedness and Management of Nurses during Disasters. Int Sci Res J. 2011;3:269–94. [Google Scholar]
- 9.Fung WM, Claudia Lai KY, YuenLoke A. Nurses’ perception of disaster: Implications for disaster nursing Curriculum. J Clin Nurs. 2009;18:3165–71. doi: 10.1111/j.1365-2702.2008.02777.x. [DOI] [PubMed] [Google Scholar]
- 10.Bahrami M, Fatemeh Aliakbari F, Aein F. Iranian nurses’ perception of essential competences in disaster response: A qualitative study. J Educ Health Promot. 2014;3:1–9. doi: 10.4103/2277-9531.139247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hassmiller S, Cozine M. Addressing the nurse shortage to improve the quality of patient care. Health Aff (Millwood) 2006;25:268–74. doi: 10.1377/hlthaff.25.1.268. [DOI] [PubMed] [Google Scholar]
- 12.Bergin A, Khosa B. Are we ready? Health care preparedness for catastrophic terrorism. Aust Strateg Policy Inst. 2007;1:1–19. [Google Scholar]
- 13.Baack S, Alfred D. Nurses’ preparedness and perceived competence in managing disasters. J Nurs Scholarsh. 2013;45:1–7. doi: 10.1111/jnu.12029. [DOI] [PubMed] [Google Scholar]
- 14.Meretoja R, Koponen L. A systematic model to compare nurses’ optimal and actual competencies in the clinical setting. J Adv Nurs. 2012;68:414–22. doi: 10.1111/j.1365-2648.2011.05754.x. [DOI] [PubMed] [Google Scholar]
- 15.Arbon P, Bobrowski C, Zeitz K, Hooper C, Williams J, Thitchener J. Australian nurses volunteering for the Sumatra-Andaman earthquake and tsunami of 2004: A review of experience and analysis of data collected by the Tsunami Volunteer Hotline. Australas Emerg Nurs J. 2006;9:171–8. [Google Scholar]
- 16.O’Sullivan TL, Dow D, Turner MC, Lemyre L, Corneil W, Krewski D, et al. Disaster and Emergency Management: Canadian Nurses’ Perceptions of Preparedness on Hospital Front Lines. Prehosp Disaster Med. 2008;23:11–8. [PubMed] [Google Scholar]
- 17.Idrose AM, Adnan WA, Villa GF, Abdullah AH. The use of classroom training and simulation in the training of medical responders for airport disaster. Emerg Med J. 2007;24:7–11. doi: 10.1136/emj.2006.036202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khankeh H, Falahi M, Ranjbar M, Ahmadi F. Health management in natural disaster. J Rehabil. 2008;9:66–72. [Google Scholar]
- 19.Suserud BO, Haljamae H. Acting at a disaster site: Experiences expressed by Swedish nurses. J Adv Nurs. 1997;25:155–62. doi: 10.1046/j.1365-2648.1997.1997025155.x. [DOI] [PubMed] [Google Scholar]
- 20.Murray V, Clifford J, Seynaeve G, Fisher JM. Disaster health education and training: A pilot questionnaire to understand current status. Prehosp Disaster Med. 2006;21:156–67. doi: 10.1017/s1049023x00003629. [DOI] [PubMed] [Google Scholar]
- 21.Greenberg MI, Jurgens SM, Gracely EJ. Emergency department preparedness for the evaluation and treatment of victims of biological or chemical terrorist attack. J Emerg Med. 2002;22:273–8. doi: 10.1016/s0736-4679(02)00427-4. [DOI] [PubMed] [Google Scholar]
- 22.Nasrabadi AN, Naji H, Mirzabeigi G, Dadbakhsh M. Earthquake relief: Iranian nurses’ responses in Bam, 2003 and lesson learned. Int Nurs Rev. 2007;54:13–8. doi: 10.1111/j.1466-7657.2007.00495.x. [DOI] [PubMed] [Google Scholar]
- 23.Slepski LA. Emergency preparedness and professional competency among health care providers during hurricanes Katrina and Rita: Pilot study results. Disaster Manage Response. 2007;5:99–110. doi: 10.1016/j.dmr.2007.08.001. [DOI] [PubMed] [Google Scholar]
- 24.Faraji A, Khankeh HR, Hosseini MA, Abdi A, Rezasoltani P. Effect of simulated training course on preparedness of nurses to do pre-hospital triage. J Health Promot Management. 2013;2:24–30. [Google Scholar]
- 25.Fung OW, Loke AY, Lai CK. Disaster preparedness among Hong Kong nurses. J Adv Nurs. 2008;62:698–703. doi: 10.1111/j.1365-2648.2008.04655.x. [DOI] [PubMed] [Google Scholar]
- 26.Wolf L, Everson FP. Does your staff really got initial patient assessment? Assessing competency in triage using simulated patient encounters. J Emerg Nurs. 2010;36:370–4. doi: 10.1016/j.jen.2010.04.016. [DOI] [PubMed] [Google Scholar]
- 27.Chapman K, Arbon P. Are nurses ready? Disaster preparedness in the acute setting. Australasian Emerg Nurs J. 2008;11:135–44. [Google Scholar]