
Figure 2.
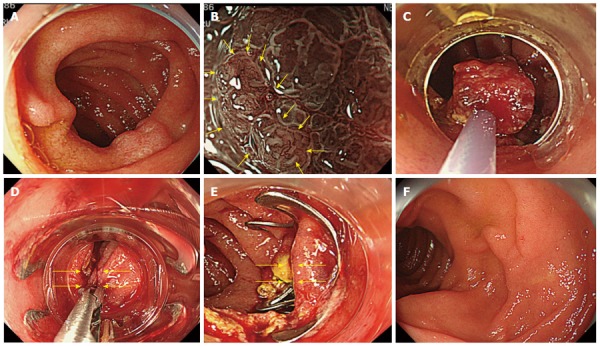
White light endoscopic image, magnifying narrow band image, resection method, closure method of case 6 (over-the-scope clip). A: An approximately 13-mm depressed lesion is observed in the posterior wall side of the slightly anal side of the major duodenal papilla in the descending portion of the duodenum; B: The magnifying narrow band image shows a clear boundary between the tumor and normal mucosa, and a mildly irregular surface structure of the tumor. The microvascular pattern (yellow arrows) shows expansion, winding, and caliber variation, which we evaluated as an inflammatory change caused by pancreatic juice and bile acid rather than malignant findings; C: After circumferential resection, en bloc resection was conducted by hybrid endoscopic submucosal dissection using a snare resection when two-thirds of the submucosal trimming was finished; D: As the artificial ulcer floor occupied half of the circumference and was close to the major duodenal papilla, closure in the minor axial direction toward the intestinal tract was attempted by grasping the mucosa in the anal and mouth sides with a twin Grasper® (yellow arrows); E: Complete suture closure was performed in the minor axial direction using an over-the-scope clip (OTSC) (yellow arrows); F: The OTSC was not visible on the ulcer floor, which had recovered within the mucosa with chorioepithelium 6 mo later.