

Abstract
Extraskeletal osteosarcoma (ESOS) is a rare soft tissue sarcoma, typically characterized by a bone-producing neoplasm. Low-grade extraskeletal osteosarcoma (LGESOS) is an extremely rare soft tissue tumor, and patients with LGESOS tend to have a better prognosis. Here, we reported a case of LGESOS of the mediastinum with lung metastasis, and describe its clinical, pathological and radiological features, and compared them with those of the reported cases.
Keywords: Diagnosis, differential diagnosis, extraskeletal osteosarcoma
Introduction
Low-grade extraskeletal osteosarcoma (LGESOS) is an extremely rare soft tissue tumor first described by Umiker in 1953 [1]. To date, only 10 cases have been published in the literature. Here, we report one case of LGESOS with lung metastasis in the mediastinum.
Case report
A 38-year-old woman underwent a surgical resection of mediastinal tumor in local hospital in 2007. Postoperative pathological diagnosis was of ossifying fibroma, and no follow-up was done after surgery. She was referred to our hospital because of persistent cough for 1 month in 2011. Chest computed tomography (CT) scan showed a 5 cm diameter mass in the left mediastinum wrapping around the left phrenic nerve, adhesion and the left lung (Figure 1). In addition, another irregular mass about 2.5 cm in diameter in left lung is likely to be a metastasis (Figure 2). Bone marrow biopsy and laboratory tests demonstrated no abnormalities. Mediastinal and lung resection was carried out to remove masses. The patient received 8 consecutive courses of methotrexate chemotherapy after surgery. No local recurrence was observed in 28 months after tumor removal and adjuvant chemotherapy.
Figure 1.

Computed tomography images of an irregular mass of high-density in the left mediastinum.
Figure 2.
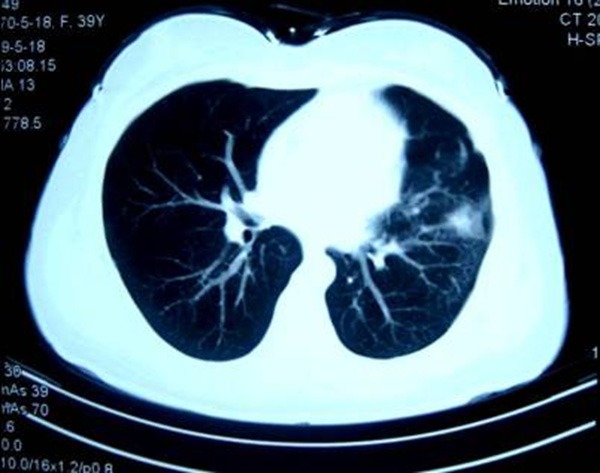
Computed tomography images of another irregular mass accompanied by calcification in left lung.
Grossly, removed primary and metastatic tumors were 5.5 cm × 4.5 cm × 4.5 cm and 2.5 cm × 2.0 cm × 1.5 cm in size, respectively. The cut surface of tumor was solid and tough with gritty feeling, but no fish flesh-like appearance. Histologically, the morphological properties removed of primary and metastatic tumors were similar to those resected 6 year ago, and the basic forms of resection specimens were alike, namely fibroblast and osteoblastic lesions. Tumor cells showed bundles and/or woven arrangement, and morphology of tumor cells were mild, similar to fibroblast/fiber cells. Occasional mitotic figures are almost always identified. The new bone trabeculae were composed of woven bone and bone like tissue with parallel tendency, and no osteoblasts around. Directly transitional phenomenon of fiber cells and bone trabeculae were observed (Figures 3 and 4). Pathological diagnosis was Low-grade extraskeletal osteosarcoma.
Figure 3.
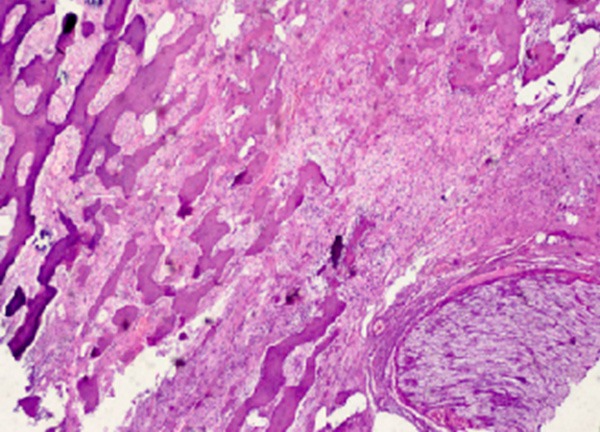
Histopathologic features of the present case. The lesion shows the formation of fiber and bone with a local invasion of host nerve (hematoxylin and eosin, × 100).
Figure 4.
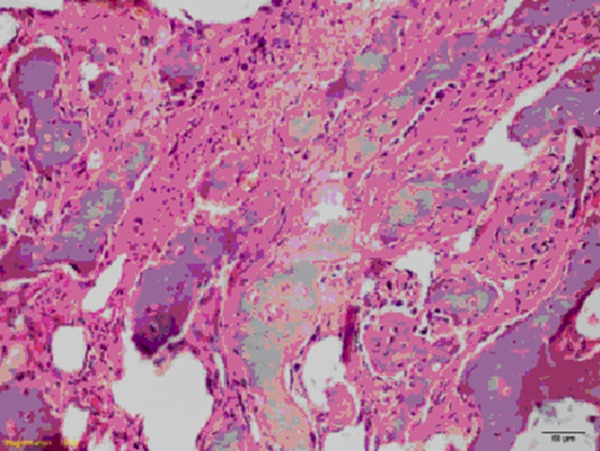
Histopathologic features of the present case. The lesion shows slightly arranged in parallel of new bone trabecula, with directly transitional phenomenon of mild atypia fiber cells and bone trabecula (hematoxylin and eosin, × 200).
ESOS is a rare malignant mesenchymal neoplasm, accounting for 1%~2% of all soft tissue sarcomas [2]. The tumor is located in soft tissue, without attachment to skeletal bones as determined by radiographic examination or inspection during surgery. The vast majority of ESOS cases published in the literature was typically characterized by high-grade histological features and prone to local recurrence and distant metastasis and have poor prognosis. LGESOS is extremely rare. In 1953, Umiker first reported 1 cases of LGESOS, so far only 10 cases have been reported, including 3 male patients and 7 female patients; the mean age was 51.4 years old (range 30~77 years); the minimum size of tumor was 5 cm × 3 cm × 2 cm, and the maximum size of tumor was 30 cm × 18 cm × 5 cm; the primary tumor site: 2 cases in the thigh, 2 in the leg, 1 in the popliteal fossa, 1 in the axillary, 1 in the back, 1 in the anterior mediastinum, 1 in the abdominal cavity, and 1 in the left shoulder. One case died in 12 months after diagnosis due to huge unresectable tumor. The other 9 cases were underwent tumor resection, and only 1 case was treated with chemotherapy after surgery. Five cases were free of disease after follow-up for 2, 12, 24, 47, and 60 months, respectively. The other 4 cases died of tumor extensive metastasis after operation for 4, 33, 48, and 48 months, respectively. In the present case, local recurrence and lung metastasis occurred within four years after the first resection because of the misdiagnosis. The resection of the recurrence and metastasis lesion was performed. During 28-month follow-up after the second resection, she was free of disease and is undergoing follow-up.
As mentioned above, these ten cases together with the case we reported suggest that LGESOS represents an extremely rare but distinct form of ESOS. It is important to recognize this tumor, because other neoplasms and tumor-like lesions may mimic the radiological and histological features of LGESOS. LGESOS needs to be discriminated from benign neoplasms, including myositis ossificans, ossifying lipoma and ossifying fibromyxoid tumor, classical ESOS, parosteal osteosarcoma, malignant mesenchymoma, synovial sarcoma and malignant fibrous histiocytoma. In brief, LGESOS may be easily misdiagnosed as benign lesions due to mild cytological atypia in the tumor cells. How to avoid the misdiagnosis of this kind of tumor? According to our experience, when fibrous lesions with bone-producing were found in the soft tissue, it should be carefully evaluate whether spindle cells with mature lineage, bone trabecula surrounded by osteoblasts, directly transitional phenomenon of fiber cells and bone trabecula, and invasion evidence were presented or not under light microscope. In a word, the biological behavior of lesions should be carefully evaluated under microscope and closely combined with lesions characteristics of clinical and imaging.
In conclusion, LGESOS appears to represent a low-grade malignant tumor with better biologic behavior than classical ESOS. However more patient cases will be needed to clearly identification of the exact biobehavioral criteria for this disease, to determine the best treatment and to evaluate the prognosis.
Disclosure of conflict of interest
None.
References
- 1.Umiker W, Jaffe HL. Ossifying fibrosarcoma (extraskeletal osteogenic sarcoma) of thigh muscle; report of a case with recurrence and widespread metastases more than four and a half years after excision. Ann Surg. 1953;138:795–800. doi: 10.1097/00000658-195311000-00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Abramovici LC, Hytiroglou P, Klein RM, Karkavelas G, Drevelegas A, Panousi E, Steiner G. Well-differentiated extraskeletal osteosarcoma Report of 2 cases, 1 with dedifferentiation. Hum Pathol. 2005;36:439–43. doi: 10.1016/j.humpath.2005.01.023. [DOI] [PubMed] [Google Scholar]
- 3.Hishida T, Yoshida J, Nishimura M, Ishii G, Nakao M, Nagai K. Extraskeletal osteosarcoma arising in anterior mediastinum: brief report with a review of the literature. J Thorac Oncol. 2009;4:927–9. doi: 10.1097/JTO.0b013e3181a52c63. [DOI] [PubMed] [Google Scholar]
- 4.Sabatier R, Bouvier C, de Pinieux G, Sarran A, Brenot-Rossi I, Pedeutour F, Chetaille B, Viens P, Weiller PJ, Bertucci F. Low-grade extraskeletal osteosarcoma of the chest wall: case report and review of literature. BMC Cancer. 2010;10:645. doi: 10.1186/1471-2407-10-645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Arai H, Rino Y, Nishii T, Yukawa N, Wada N, Oshiro H, Ishida T, Nakaigawa N, Masuda M. Well-differentiated extraskeletal osteosarcoma arising from the retroperitoneum that recurred as anaplastic spindle cell sarcoma. Case Rep Med. 2010;2010:327591. doi: 10.1155/2010/327591. [DOI] [PMC free article] [PubMed] [Google Scholar]