
Figure 2.
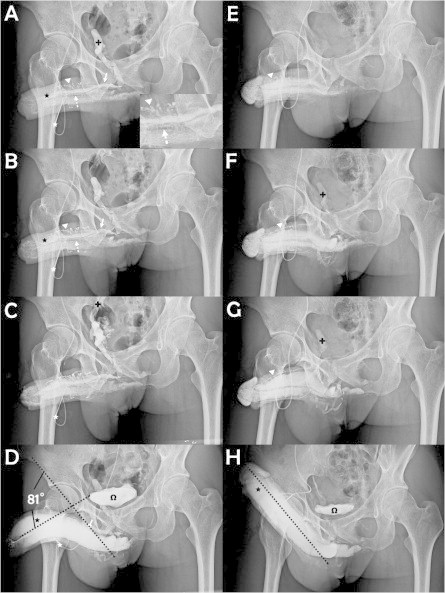
Cavernosography showing the surgical outcomes. (A) A cavernosogram taken immediately after an intracavernous injection with 50% contrast medium into the sinusoids (black asterisk) of the corpora cavernosa (CC) via a 19-G scalp needle (white asterisk). The DDV (white arrow) was depicted, with the CVs (dotted arrow) beneath, whereas the para-arterial veins (PAVs, white arrowhead) had a zigzag appearance. The internal pudendal vein (black cross) appeared rapidly. (B) As the injection (white asterisk) continued both the DDV (white arrow), CVs (dotted arrow), PAVs (white arrowhead) and CC (black asterisk) became pronounced. (C) The injected solution drained rapidly back to the level of internal iliac vein (arrow) which continues the internal pudendal vein. (D) A film taken 15–30 min later after an injection with 20 μg of PGE1. The depicted DDV (white arrow) documented the venous leakage despite the rigid erection; the urinary bladder (omega) is shown. A penile deviation of 81° was estimated. (E) A film of a patient with a similar condition to that in panel A at 1 year after surgery; the CC (black asterisk) was readily inflated, while neither the DDV (white arrow) nor the CVs (dotted arrow) were apparent, but the PAVs (white arrowhead) were smaller. (F) Likewise, comparing with the view in panel B, there were no further leaky veins because the depiction of the internal pudendal vein (black cross) was minimal. (G) For comparison with panel C, the internal iliac vein (black cross) was apparent. (H) A full erection was readily induced after an injection with 10 μg PGE1. The CC (black asterisk) and bladder (omega) were inflated, as compared with panel D. The penile became straight, apparently at an ideal erection angle (dotted line), which should sustain a buckling pressure.