

An 80-year-old man was found to have a 1.4 cm lesion on right side of the lower lobe central parenchymal lung nodule on chest computed tomogram (CT) while undergoing evaluation for a cough [Figure 1a and b]. The lesion was metabolically active on positive emission tomography without any evidence to suggest involvement of mediastinal/hilar nodes or distant metastasis. Flexible bronchoscopy with transbronchial biopsies confirmed this lesion to be lung adenocarcinoma. The patient's comorbidities precluded surgical resection, and he was scheduled to have stereotactic body radiation therapy (SBRT). Given the central location of the nodule and its close proximity to the esophageal wall, fiducial markers placement inside the tumor was recommended. Convex probe endobronchial ultrasound (CP-EBUS) was used to place three fiducial gold markers (0.35 mm × 5 mm, Visicoil, IBA) using a 22 Gauge EBUS needle (Olympus, NA-201SX-4022). The fiducials were loaded into the EBUS needle distally (front-load), and bone wax was applied to secure the fiducials in place [Figure 1c and d]. Under real-time CP-EBUS guidance [Video 1], each fiducial was placed inside the tumor at a peripheral location forming a triangular shape inside the tumor [Figure 2a–c]. Color Doppler was used to prevent vascular puncture or accidental intravascular fiducial placement. The procedure time was about 30 min, and the patient reported no operation-related complications and the fiducials showed no evidence of migration [Figure 2d–f]. The patient underwent SBRT (how many fractions) without any complications.
Figure 1.
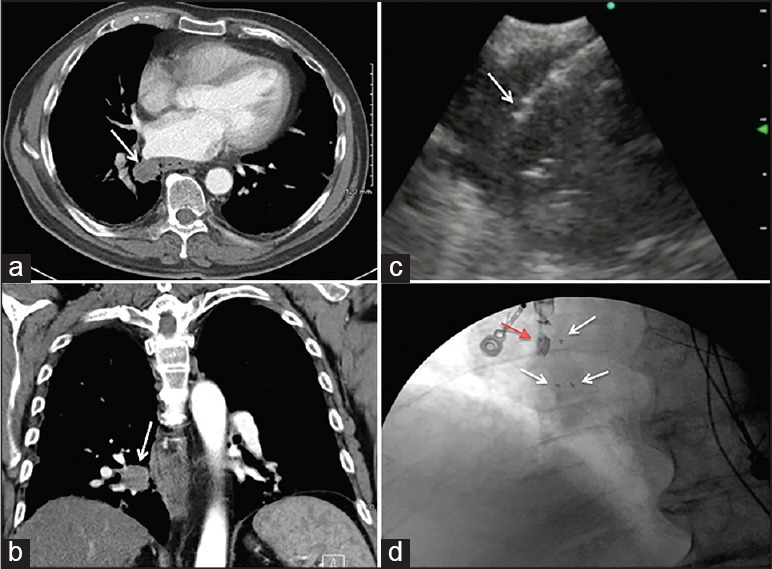
(a and b) Chest computed tomography axial and coronal views showing the right lower lobe central nodule. (c) Convex probe endobronchial ultrasound (CP-EBUS) image showing the fiducial marker inside the tumor (arrow). (d) Intraoperative fluoroscopic image showing the tip of the EBUS scope (red arrow) and the three fiducial markers that were placed using CP-EBUS (white arrows)
Figure 2.
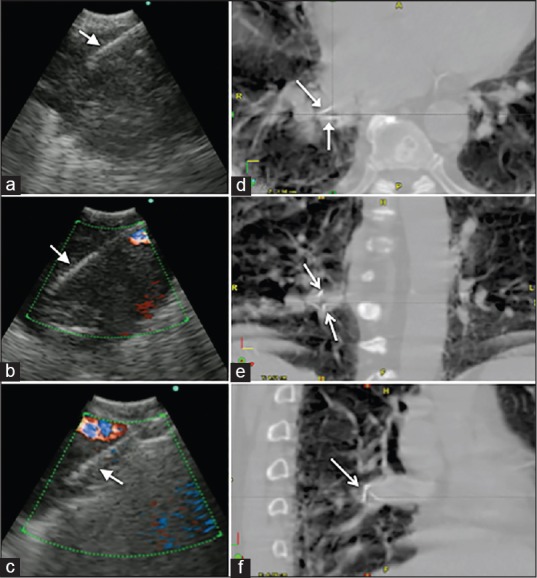
(a-c) Convex probe endobronchial ultrasound images showing the EBUS needle (arrows) at different locations inside the tumor representing where the three fiducials markers were deployed. (d-f) Images from the stereotactic body radiation therapy planning scan showing the fiducial markers inside the tumor (arrows)
Surgical resection remains the first-line treatment for early-stage peripheral lung cancer.
In patients with multiple comorbidities that preclude surgery, alternative therapy such as SBRT is considered. Fiducial markers placement for lung cancers is commonly performed to guide SBRT or surgical resection. Percutaneous CT-guided fiducial placement is associated with pneumothorax rate up to 48%.[1] Since advanced bronchoscopic techniques provide improved diagnostic accuracy and fewer complications over conventional bronchoscopy, they are now more commonly used for fiducial markers placement to guide radiation therapy. Both radial probe EBUS and electromagnetic navigation have been used for implanting of fiducial markers.[2] These devices may be used as markers to guide radiation therapy. The complication rate such as migration and pneumothorax is, usually, low.[3] In one group, 90% of the markers remained in place during the time of radiosurgery.[4]
CP-EBUS is widely used for the diagnosis and mediastinal staging of lung cancer. CP-EBUS has been also used to guide fiducial markers placement in the peribronchial and mediastinal lymph nodes.[5] CP-EBUS can be utilized for diagnosis of central parenchymal lung nodules and masses, along with simultaneous mediastinal staging. In these cases, fiducial markers placement can be performed in the same setting using CP-EBUS as no complications have been reported.[5,6]
Convex probe endobronchial ultrasound placement of fiducial markers is a safe and useful procedure to guide stereotactic radiosurgery for centrally located lung cancers.
Video available on www.eusjournal.com
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Pennathur A, Luketich JD, Heron DE, et al. Stereotactic radiosurgery for the treatment of stage I non-small cell lung cancer in high-risk patients. J Thorac Cardiovasc Surg. 2009;137:597–604. doi: 10.1016/j.jtcvs.2008.06.046. [DOI] [PubMed] [Google Scholar]
- 2.Harley DP, Krimsky WS, Sarkar S, et al. Fiducial marker placement using endobronchial ultrasound and navigational bronchoscopy for stereotactic radiosurgery: An alternative strategy. Ann Thorac Surg. 2010;89:368–73. doi: 10.1016/j.athoracsur.2009.09.048. [DOI] [PubMed] [Google Scholar]
- 3.Toba H, Kondo K, Miyoshi T, et al. Fluoroscopy-assisted thoracoscopic resection after computed tomography-guided bronchoscopic metallic coil marking for small peripheral pulmonary lesions. Eur J Cardiothorac Surg. 2013;44:e126–32. doi: 10.1093/ejcts/ezt220. [DOI] [PubMed] [Google Scholar]
- 4.Anantham D, Feller-Kopman D, Shanmugham LN, et al. Electromagnetic navigation bronchoscopy-guided fiducial placement for robotic stereotactic radiosurgery of lung tumors: A feasibility study. Chest. 2007;132:930–5. doi: 10.1378/chest.07-0522. [DOI] [PubMed] [Google Scholar]
- 5.McGuire R, Liming J, Ochran T, et al. Real-time endobronchial ultrasound-guided implantation of radiotherapy monitoring devices. J Bronchology. 2007;1:59–62. [Google Scholar]
- 6.Tobias L, Decker R, Puchalski J. Convex probe endobronchial ultrasound for placement of intraparenchymal fiducial markers to guide stereotactic radiosurgery. Chest. 2011;140:164A. [4_MeetingAbstracts] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.