
Figure 2a.
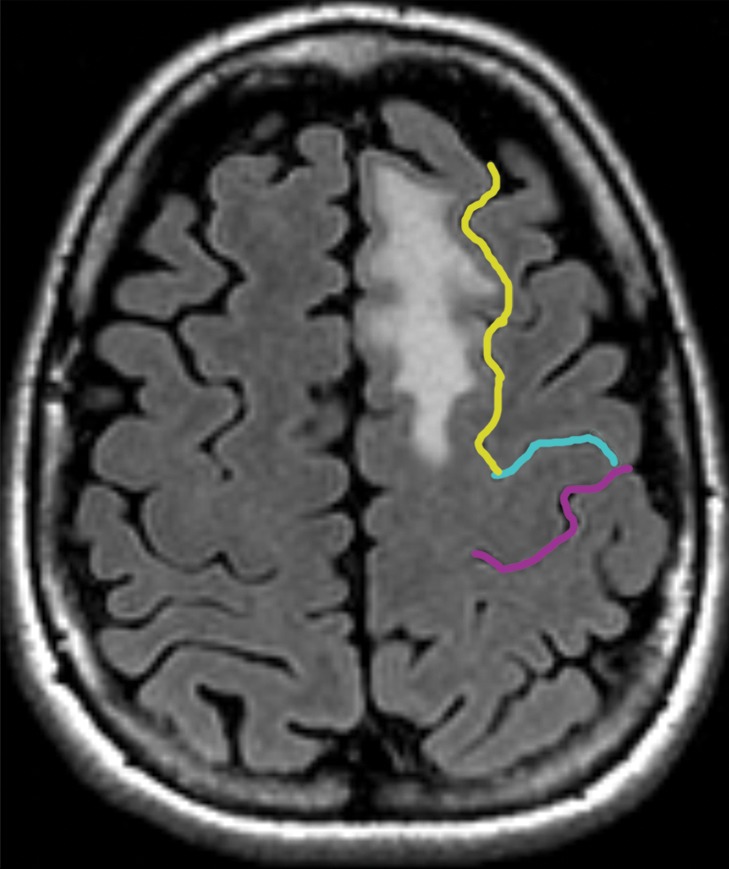
Partial SMA syndrome after glioma resection. A 22-year-old woman underwent magnetic resonance (MR) imaging because of seizures. She reported increasing incoordination, causing difficulty typing and walking her dogs. Resection of the SMA tumor revealed anaplastic astrocytoma. Postoperatively, she experienced a debilitating naming deficit, which improved, in keeping with partial SMA syndrome. (a) Axial fluid-attenuated inversion-recovery (FLAIR) MR image shows nonenhancing tumor confined to the superior frontal gyrus (yellow). (See Table for color coding of sulcal lines.) (b) Axial functional MR image obtained during a right-hand motor task shows normal blood oxygen level–dependent (BOLD) activation in the central sulcus at the hand knob (lateral white pixels) and in the SMA (medial white pixels) at the position of the upper extremity (UE) motor cortex region. The lower extremity (LE) region of the SMA should be somatotopically arranged posterior to the upper extremity SMA region, and the speech region is located anterior to it. (c) Axial functional MR image obtained during a category-naming task shows normal BOLD activation in the speech region of the SMA at the margin of the tumor. (d) Axial T1-weighted MR image shows the appearance after gross total resection of the anaplastic astrocytoma involving the speech region of the SMA.