
Fig 3.
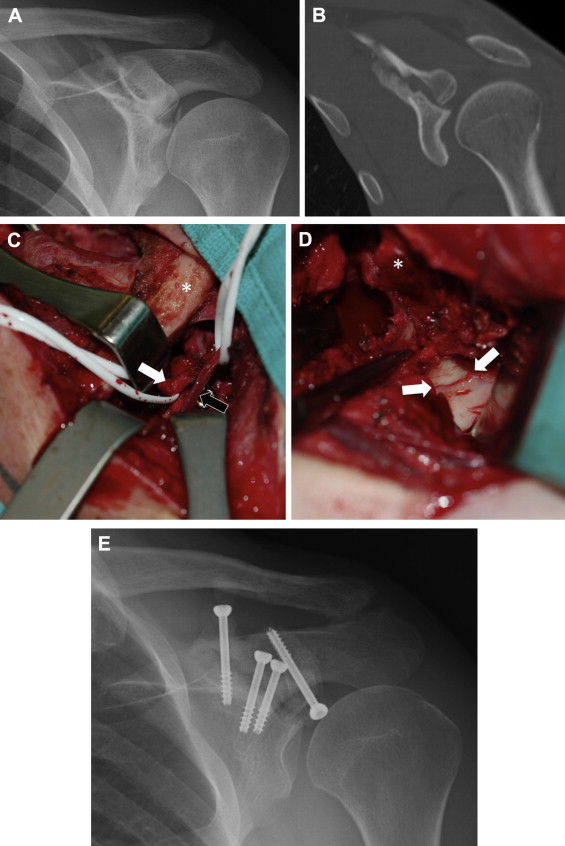
A 26-year-old man with an established nonunion of an Ideberg type III fracture. An open approach was required to mobilize the fibrous nonunion and to free the suprascapular nerve, which had electromyographic changes and was entrapped in callus. Had this case been managed arthroscopically initially, such extensive surgery may not have been required. (A) Anteroposterior radiograph showing both articular step-off and traction of suprascapular nerve at suprascapular notch. (B) Coronal computed tomography scan showing articular incongruity and nonunion. (C) View from superior of combined deltopectoral and supraspinatus fossa approach. The clavicle (asterisk) is medial. The suprascapular nerve (white arrow) is visible, as is the suprascapular artery (black arrow), with an adjacent screw head. (D) View from superolateral showing glenoid articular reduction (arrows) and coracoid osteotomy (asterisk). As in the arthroscopic case, the rotator interval has been opened widely and the supraspinatus is retracted laterally. (E) Final fixation. Multiple screws were used more medially given the need to reduce the suprascapular notch.