

Abstract
Background:
Nursing continuing education with development of knowledge, skill, and attitude results in improvement of nursing activity, and thus improves the health care in the society. If the education is not planned and implement properly, it affects the patient care. This study was designed to explore the challenges of nursing continuing education in Isfahan University of Medical Sciences hospitals.
Materials and Methods:
The research was conducted from April 2012 to February 2013 in Isfahan, Iran. The sampling was begun with purposeful method and continued with snowball method. Thirty-nine participants were selected among the nurses of Alzahra, Kashani, and Noor hospitals, nursing and midwifery faculty, continuing education center, and the vice-chancellery for treatment. The participants were both learners and planners of continuing education program. In this descriptive explorative qualitative research, we interviewed 39 participants in five focus group and five individual interviews, until data saturation was achieved. We used semi-structured interviews and field notes for data gathering, and members checking, triangulation (data and method), peer debriefing, and peer review to increase the strength of data. Data were analyzed with thematic analysis method that was proposed by Broun and Clarke in 2006.
Results:
Data analysis produced 175 initial codes, 8 subthemes, and 5 main themes. The main themes included: Learners related factors, teachers related factors, educational process related factors, inadequate facilities, and defective evaluation.
Conclusions:
According to the results, we need to revise the educational process in nursing continuing education. To achieve this goal, we need a team for needs assessment, planning, and evaluation. In addition, we must pay attention to educators’ and learners’ issues.
Keywords: Continuing education, Iran, nursing, qualitative, research, staff development
INTRODUCTION
Continuing education includes planned learning experiences which lead to improvement of nurses’ attitude, skills, and knowledge and, consequently, promote nurses’ function and care plan in the society.[1] Seminars, workshops, and conferences provide a chance for constant professional development and empowerment.[2]
Knowledge of nurses should be updated. As the core of the activities of nurses, as the staffs who have knowledge of care, is focused on humans, investment on continuing education is essential for nurses’ competency in organizations.[3] Nursing texts show that continuing education is a basic component of professionalism in nurses and can act as an organizing element in nursing function.[4] American Medical Institute reported that skillful and educated nurses should be trained for the future of nursing. Obviously, skillful nurses cause promotion in quality of services; therefore, the obstacles and challenges of nurses’ education should be clarified.[5] Various studies point to nurses’ continuing education challenges as the following: Being an obligatory education and lack of motivation for learning in some nurses,[6] high number of participants in classes, financial resources restriction, restriction in the number of clinical places, shortage of educational budget, nursing school work overload which leads to lack of adequate time for educational courses,[5] type of planning for continuing education activities, time limitation and lack of workforce,[7] lack of satisfaction with time and schedule of the educational classes conducted, low applicability of lectures, no coincidence between educational needs and conferences outlines, and lack of familiarity with nurses’ educational needs among physicians.[8]
On the other hand, nurses should yearly pass 40–60 h of education in Iran which is much more than the specified educational hours in developed countries (average of 24 h in a year),[9] while neither nurses nor the authorities are satisfied with the results of education and the way of holding that. Most of the research conducted in continuing education context has been related to nurses’ approaches, perception, and attitudes toward continuing education, the effect of continuing education on nurses’ professional competencies, assessment of continuing education needs, provision of continuing education models, and professional nurses’ challenges and educational strategies. Therefore, it is needed to investigate nurses’ continuing education further and more precisely to clarify the problems existing in this context. As most of the research conducted in this field has been quantitative and descriptive, and few qualitative studies have been already conducted on continuing education, conducting such a study seems essential. There are the individuals who either use continuing education for their professional promotion or plan this education for other individuals to use. This study aimed to explore existing challenges in nursing continuing education.
MATERIALS AND METHODS
This is an explorative descriptive study conducted on nursing continuing education challenges among nurses of three hospitals (Kashani, Alzahra, and Noor va Hazrate Aliasghar) and the education authorities of Isfahan University of Medical Sciences, Iran. The study was conducted from March 2012 to January 2013 in Isfahan University of Medical Sciences.
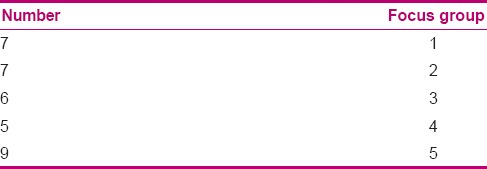
Sampling was purposive, and the participants comprised the nurses who had to undergo continuing education, including educational supervisors, head nurses, staff nurses, and all continuing education program related personnel. In the present study, firstly, the researcher referred to each of the university hospitals affiliated to Isfahan University of Medical Sciences one by one to explain the project to the educational supervisors who were responsible for providing continuing education in hospitals. They were asked to introduce the nurses who met the inclusion criteria. Five homogenous focus group sessions (with regard to work experience) containing from five to nine participants in each session were held. Based on either the educational supervisors’ decision on how many nurses who met the inclusion criteria could be introduced to the researcher or their own desire to attend the research, the number of participants differed in the focus group sessions.
The numbers of participants in each session has been presented on Table 1. Five semi-structured individual interviews with open questions were held for five persons from the university continuing education program related personnel and nursing association, as well as the vice-chancellery for medical treatment. Group semi-structured interviews and individual interviews were held with 34 and 5 participants, respectively. There were a total of 39 participants in the study. Inclusion criteria were the nurses under continuing education rule, educational supervisors, head nurses, the authorities responsible for holding continuing education courses, and the nurses who were interested in and had adequate time to attend the study.
Table 1.
Number of participants in focus group
Exclusion criteria was the cases who was excluded during the study. Data were collected from June 2012 to September 2012.
At the beginning of focus groups session, some explanations about the discussion goals and regulations were given to the participants. The interviews started with open questions and were followed with other related questions until their complete. Duration of focus group sessions was 90–120 min, while it was 20–35 min for individual interviews. Interviews were recorded by two digital voice recorders in focus group sessions and one in personal interview sessions. Data collection continued until data saturation. The location of the interviews was selected based on participants’ preference at their work place. The time of interviews was arranged based on participants’ interest. After holding interviews, in case of any further questions, the researcher contacted the participants through referring to them by phone calls or e-mail concurrent to data collection. The data were analyzed by Brown and Clark thematic inductive content analysis (2006).[10] The researcher listened to the focus group or individual interview sessions immediately after recording them, and after finding a sense of whole, transcribed all the interviews verbatim word by word so that analysis units were formed. Then, the data were read line by line, and key sentences and phrases were allocated, underlined, and coded. Similar codes were combined and primary categories were made. Data reduction was conducted in all analyzed units until categories emerged, so that general, conceptive, and inductive data were put in the main category. For conducting a proper content analysis in this study, a 15-item checklist, made by the above-mentioned writers and used in a qualitative research, was adopted.[11] Regarding rigor of the data, member check was used. The data were collected through interviews, non-official observations, and fieldwork notes (combination of methods).
In data analysis, narrations and extracted codes were referred to some qualitative research experts in relation with the subject of study and their indications were considered and followed. Ethical considerations were met by obtaining permission from the ethics committee of the university, and a written informed consent from the participants and consideration of their rights to cancel their attendance in the research.
RESULTS
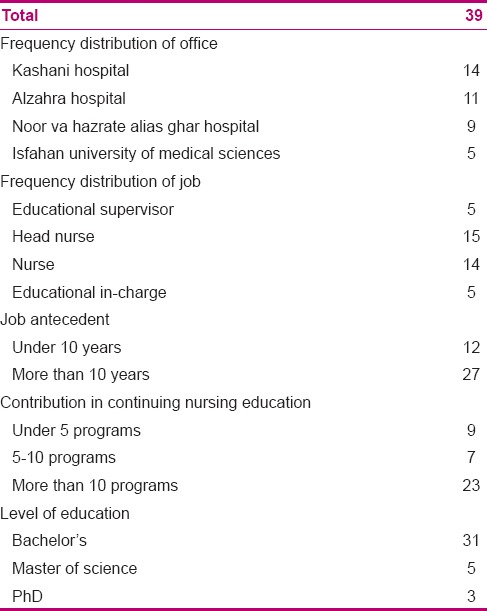
There were 30 female and 9 male participants with a work experience of 2–30 (14.5) years and age of 25–50 (36.5) years. Six participants were from nursing office, 27 from various wards of the hospitals (Alzahra, Kashani, and Noor va Hazrate Aliasghar), 1 participant from the nursing association, 3 from the university continuing education office and nursing school, and finally, 1 participant was from the vice-chancellery for medical treatment. Participants’ education levels were MS of nursing, PhD of nursing, and medical doctorate. The participants spoke Persian. Their demographic characteristics have been presented in Tables 1 and 2. The findings of the present study included 175 primary codes, eight subthemes, and five themes.
Table 2.
Demographic data of participants
Themes obtained in this study were learners related factors, teachers related factors, educational process related factors, inadequate facilities, and defective evaluation. Each obtained theme had its own subthemes [Figure 1].
Figure 1.
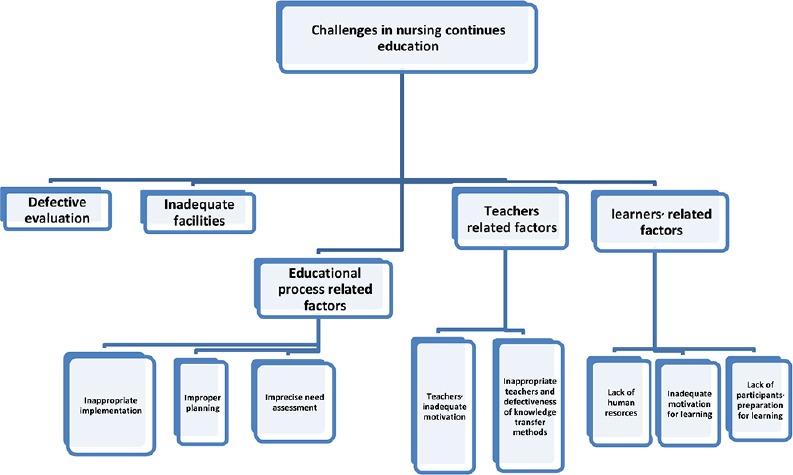
Themes and subthemes
Learners related factors
Most of participants’ remarks were about the fact that their attendance to educational classes had no quality outcome due to their working shift being parallel to the educational classes, having night shift before the classes, and being involved in familial responsibility. They also pointed out the existing obligation in attendance to classes and lack of any relation between the educational courses and their needs. Almost all the participants pointed out inadequate nursing personnel as an indirect element reducing the expected quality of these educational courses.
Lack of participants’ preparation for learning
Based on their experience, the participants mentioned tiredness of personnel due to working shifts, high number of night shift personnel in continuing education classes, lack of concentration among night shift personnel in the classes, high educational and work-related pressure imposed on the personnel, familial responsibilities, and many other factors as the existing problems in this context. In relation with lack of preparation for learning, participant no. 24 stated:
“… Most of us look at one another to see how much the attendees are listening, they are either day dreaming or hardly listening. Most of the attendees are working in night shifts.”
Inadequate motivation for learning
Participants indicated their constraint to attend the classes to get a better grade, lack of motivation to attend intra-ward classes due to inappropriate arrangement, the decreased interest of personnel in learning due to unexpected changes of schedules and instructions, and lack of motivation to attend classes due to inappropriate time of classes for some of the participants.
In relation with lack of motivation, participant no. 24 stated:
“… The time of education (continuing education) is awful; most of the nurses are female and have children, they have to be out of home for 12 hours as they should either be in the class, and then, at their shift or first at their work, and then, in the class. So, nobody comes to classes with motivation.”
Lack of human resources
Participants pointed to inadequate number of nursing personnel as a factor for reduction of personnel's attendance in the educational classes. In this regard, participant no. 19 said:
“… We face shortage of personnel and they do not have so much motivation. Taking the personnel out of the ward for education is one on the challenges of our educational supervisor.”
Teachers related factors
The participants talked about inappropriate teachers, defective knowledge transfer methods, teachers’ inadequate motivation and their lack of familiarity with nursing, limitations in abilities of some of the teachers in education, lack of variety in educational methods, and delayed and low payment of teachers. It should be noted that some of the teachers were from medical school and based on many participants’ viewpoints, they did not know nurses’ educational needs.
Inappropriate teachers and defective knowledge transfer methods
Participants indicated lack of familiarity of some of teachers with nursing education, lack of appropriate teachers, high payment of skillful teachers, low payment given to the teachers by hospitals, lack of teaching skills among all teachers, lack of variety in educational program outlines, and inappropriate teaching method as the factors causing problems in provision of appropriate education.
With regard to the issue of inappropriate teachers, participant no. 12 said:
“… Most of the times, the teacher is a physician. We know what ICP or IICP is, but they want to work more on our terminology, explain types of hematomas. When I show him our reference for respiratory diseases and say we know all of these, the teacher says, really, I did not know nurses also study these issues.”
With regard to defective knowledge transfer methods, participant no. 13 said:
“… I think teaching methods are wrong too. For example, for education about a ventilation device, it would be better if they would bring a device and educate nurses one by one in a group of six, but as they want to educate 100 nurses in one course, they have a wrong teaching method.”
Teachers’ inadequate motivation
The word “teachers” refers to all educational agents in the wards, educational supervisors, head nurses, every individual who teaches in hospitals, and academic members.
The participants pointed to tiredness of educational agents due to overloaded educational responsibilities in addition to working in the ward concurrently, lack of teachers’ spiritual and monetary motivation, and the delay in teachers’ payment. In relation to the delay in teachers’ payment, participant no. 36 stated:
“… The registration fee obtained from participants should be given to continuing education offices as it is online. As we have to return the money to the university, the payments are delayed, and these are among the problems created for the teachers in the faculty.”
The above-mentioned problem exists in organizational bureaucracy, ultimately leading to teachers’ delayed payment which is an existing challenge in this context.
Educational process related factors
Imprecise need assessment
From the viewpoints of the participants, needs assessment is not properly done. They think it should be done individually and correctly. They also indicated that although needs assessment forms are completed, they are considered generally and the needs of each individual and each ward are not separately and adequately noted. So, the outline of educational subjects is not selected according to needs assessments. Participant no. 11 stated:
“…. We fill a needs assessment form, and then, educational supervisor arranges the classes for us. The assessments are not categorized and the classes are held for the whole staffs in hospital.
Education can be also sorted like a ventilation device class for the staffs of ICU or an ECG interpretation course for cardiac ICU ward staffs. This can be also categorized in hospitals….”
Improper planning
Participants pointed to holding educational programs without consideration of attendees’ viewpoints, lack of adequate supervision on educational contents, low consideration or ignoring promotion of nursing personnel's attitude toward education, lack of an education committee, and inadequate personnel to plan education programs. In this regard, participant no. 38 stated:
“… We here cover a province of which the treatment section contains over 20,000 working staffs. When I, as the head of a unit, want to plan for 20,000 working staffs in treatment section, how many personnel do you think I need? If we calculate one personnel for each 1000 working staffs, it will be 20 education officers. Meanwhile, I work with only four education officers, this is not logical at all!”
Inappropriate implementation
Participants pointed to inapplicability of some classes, impossibility of holding education classes, lack of relevancy between educational content and length of class, inappropriate time of classes, prolonged time of education, and lack of group education. In this regard, participant no. 11 stated:
“… Educational classes are short in time, but contain a lot of materials. They want to teach us a load of materials in one day or one hour, I think it is not efficient.”
Inadequate facilities
Participants indicated no relevancy between education and the existing facilities, shortage of educational budget, inappropriate location of intra-ward education, high number of participants in some of the educational classes, and inadequate education assistive equipments as the main factors creating challenges in correct provision of educational classes.
In this regard, participant no. 38 said:
“… The most important problem in quality of education is the budget which does not exist. This causes challenges for everybody in any educational course and educational program in any of its stages, as every stage needs a budget to be conducted.”
Defective evaluation
Participants pointed to lack of a pre-test post-test in some classes, lack of giving a feedback to the learners even in classes with a pre-test post-test, lack of educational evaluation of the personnel in relation with the held education program, lack of supervision on the educational content of continuing education by the authorities, and lack of efficacy of the education.
Participant no. 35 stated:
“… Programs are not evaluated well although we have been appointed to do so as educational officers. Precise evaluation of the programs is impossible due to load of work. This needs a team. I cannot attend all the programs or supervise them due to high load of work.”
DISCUSSION
Based on the obtained findings, the results were assigned to five themes of learners related factors, teachers related factors, educational process related factors, inadequate facilities, and defective evaluation.
In relation with learners related factors, preparation for learning was one of the main concerns of the participants. Some stated that they could not concentrate well in the class due to having a working shift before classes or family-related responsibilities. Some others mentioned that there should be an educational shift for the personnel. Chong, in a cross-sectional study on the factors effective on Malaysian nurses’ attendance in continuing education, reported that they mentioned their work overload and familial responsibilities as the obstacles causing tiredness and restricting their attendance.[7]
Mohamadi and Dadkha, in a descriptive study on evaluation of continuing education from the viewpoint of nursing personnel, showed that 28.2% of the nurses were dissatisfied with the time table of educational classes, actually due to being tired in the class, which resulted from a working shift or having familial responsibilities.[8]
In relation with learners’ motivation in learning and attending educational classes, as in some occasions and in some wards, education was held in nursing station and nurses were concurrently involved in patients’ affairs, they lost their motivation. On the other hand, obligatory classes in addition to obligatory overtime and familial responsibilities were among the factors which decreased nurses’ motivation. Farmani, in a cross-sectional descriptive study on nurses’ viewpoints concerning continuing education, showed that when educational programs interfere with learners’ occupational and familial duties to a lesser extent, the nurses may have higher motivation to attend the programs, which consequently leads to improvement in the quality and efficacy of continuing education programs.[12]
Griscti and Jacono mentioned that what motivates nurses for learning should be clarified and considered. Nurses should also play a role in their own learning, and a team work is needed to conduct continuing education appropriately.[6] In relation with shortage of human resources, the participants believed that the shortage of nursing personnel is a factor that affects personnel's voluntary attendance in education programs such that when the personnel attend the courses obligatorily and concurrently with working shifts, the education programs do not result in an appropriate effect. Chong showed that low number of nurses causes time limitation which is one of the challenges in continuing education.[7] Shortage of work force is a factor which can highly affect other sides of the work. Many authorities believe that nursing work force is adequate based on their outdated existing protocols for the number of work force and, consequently, resist against an increase in the number of personnel. Meanwhile, the work force also complains of work overload. Trained personnel leaving the organizations due to lack of job satisfaction is another challenge the health organization faces. Nursing authorities claim that the organizations cannot contribute to fulfillment of staffs’ spiritual and monetary needs. As a result, the organizations act as training centers in which the nurses are trained and then leave to immigrate to other countries for a better working condition.
Participants’ experiences concerning inappropriate teachers showed they preferred to be educated by higher rank nurses instead of physicians. They believed nurses understand their needs, abilities, and university education better. They also believed that nurse educators should have appropriate teaching method and skills of the related specialty.
Farmani et al. showed that familiarity of the teachers of continuing education with new teaching methods and models, especially collaborative and workshop methods, is essential to attract and motivate the learners,[12] and can act as an effective factor on the quality of education.
Mohamadi and Dadkha showed that 55.2% of nurses evaluated the education conducted by physicians as moderate, possibly due to lack of homogeneity of the teacher and the learner.[8] Fairchild et al., in a qualitative study on the educational needs of nurses in rural areas, showed that nurses’ learning needs should be based on either skill or knowledge. This comes true when the teacher is well acquainted with nursing skills and needs.[13] In relation with the knowledge transfer methods, participants pointed to lack of proper practical workshop education. Some of them complained about lack of different teaching methods and the use of just lectures and a slideshow in many of the educational classes, which was so tiring in these classes. Fitzgerald et al. mentioned the increase of simulation in education as a strategy to improve the quality of education.[5] Farmani also showed that 67.4% of nurses believed that combination of attendance and non-attendance education was the best method of receiving education. They (66.7%) also mentioned lecture method and group discussion as the most appropriate methods of education.[14] Many of the participants in the present study also requested for discussion in educational sessions. Mohamadi and Dadkha reported that 27.7% of nurses stated that practical examples were given in educational classes, while only 28.8% reported that questions and answers method was used to complementary the education.[8] Mohamadhoseini also showed that over 50% of the participants pointed to workshops as the best way to hold continuing education programs.[15] In relation to continuing education methods, Griscti and Jacono showed that workshops, in which there is an interaction, have the best effect on professional function changes, compared to lecture method and university education.[6] With regard to the motivation of teachers, our obtained results showed that due to delayed payment and not obtaining notable advantages through classes, the teachers are not so interested in conducting education sessions. Most of the participants, who were among learners, also pointed to this issue. They claimed that as the teachers are not given any extra promotion according to their ability, they have no motivation to conduct the education. Fitzgerald showed that the considered budget for teachers is not adequate, and in fact, there is a wide gap between the budget and the work done.[5] The participants also believed that the responsibilities of education agents and educational supervisors (who also are involved in education) are too many. The responsibilities of education agents should be reduced, for example having some circulating shifts specified for education in a month, so that they can keep in touch with all personnel while either not being in charge for a patient or having fewer responsibilities, in order to educate the personnel more conveniently. The number of educational supervisors can be increased according to the number of personnel to let them have more time to hold education sessions more conveniently. On the other hand, facilitation of and speeding up the process of teachers’ payment and giving them adequate advantages can act as a factor to increase their motivation to be involved in education. Although a motivation may not be just monetary, giving advantages to the teachers by the related universities can motivate them to be more active in education.
Literature review showed that low attention has been paid to learners related problems, and as they are one of the basic elements in continuing education, this can be one of the main challenges in this context. Their problems must be given more attention.
In relation with educational process related factors, the present study showed that (in the section of needs assessment) the method of needs assessment should be revised. Chong showed that continuing education activities should meet the least educational and professional needs of the nurses.[7] Farmani et al. showed that 90.9% of nurses mentioned the needs assessment, conducted on them, as the best method to select the outline of continuing education programs and 52.3% mentioned the relevancy between the content of continuing education programs and their professional needs as average.[12] Mohamadi and Dadkha concluded that 59.8% of nurses do not find the subjects of conferences related to their professional needs.[8] Ghasemi et al. determined educational needs of personnel through use of a questionnaire, concluding that their most important need was patient education. Then, all educational programs were designed and implemented in the frame of personnel education needs in the form of an educational model. Results showed that quality of patient care was notably higher in the experimental group, possibly due to the needs assessment and planning conducted accordingly.[14] Griscti and Jacono stated that continuing education programs should be based on every individual's needs, and if a needs assessment has to estimate essential needs, it should be precise.[6] Fitzgerald reported the basic changes made in curriculum as a strategy to improve the quality of education to support capability and problem-based learning.[5] As most of the participants in the present study pointed out needs assessment to be in a correct, basic, and realistic way, it can be noted that nurses’ educational needs can be revealed through interview method. The participants in our study asked for personal needs assessment. Therefore, needs assessment in continuing education is a crucial element which affects the quality of education to a greater extent. Educational needs assessment is possible through various ways. For instance, Fairchild et al. conducted a qualitative study on nursing managers (administrators) concerning nurses’ educational needs.[13]
With regard to planning, the present study showed that shortage of personnel for precise planning of the education and lack of consideration of learners’ attitudes are among the educational challenges. Fitzgerald reported work overload of the faculty as one of the educational challenges. Increased work overload of the faculty may disturb planning of education programs.[5]
Chong pointed to the type of continuing education activities planning as one of the obstacles in nurses’ attendance in education programs.[7] Mohamadi and Dadkha reported that personnel's viewpoints (35.5% of the staffs) are not considered in planning.[8] Therefore, it can be noted that the implemented education programs for these personnel did not meet the needs of the ward where they worked. If educational planning can be conducted by the owners of the process (educational supervisors in each hospital), or they can be somehow involved in this process, the challenges of planning may be reduced. They should also be empowered in this direction. In Ghasemi's study on a new educational model, outlines, priorities, and educational methods, the length of education and location of education were determined by personnel's request and based on the ward facilities. In fact, all issues that were considered for planning were arranged according to personnel's viewpoints. Their findings showed that the mean and SD of nursing care quality in relation with recording nurses’ notes, patients’ clinical condition, quality and quality of patient education increased in both experimental and control groups after intervention, but the increase was more significant in the experimental group.[14] In the above-mentioned study, education was in balance with the related ward. As all the personnel were involved in planning, it can be noted that the number of planners was higher than usual. Falmer et al. stated that if a model for educational planning is designed by university teachers, nursing authorities, and nurses correctly and is implemented precisely, it can improve the quality of nurses’ education and, ultimately, their function.[16]
In relation with the conducted education programs, the present study showed that lack of implementation for some education programs and the inapplicability of some others are among the existing challenges in this context, which can be associated with shortage of organizational budget. Meanwhile, in such a condition, inapplicability of some education programs, with regard to shortage of personnel and time, is a challenge which wastes the consumed sources such as teachers’ and learners’ time. On the other hand, lack of implementation of the education can be associated with the issue of needs assessment, so that with a correct needs assessment, applicability and implementation of education are possible. In the study of Ghasemi et al., as the design of the model was based on the existing facilities in the ward, it was applicable and led to promotion of quality of education.[14] Mohamadi and Dadkha showed that 25% of the individuals evaluated the applicability of lectures as low, while 45.2% of the subjects found it average. About 56.5% of the subjects found the condition of materials’ presentation in continuing education as average, while 28.2% were dissatisfied with the time of educational classes.[8] Farmani et al. also stated that 67.4% of nurses mentioned a combination of attendance and non-attendance method of education as the most appropriate one.[12] Mohamadhoseini found that half of the participants evaluated the correctness of holding education sessions as very high. The content of the programs was evaluated as average, which reveals that the programs were not completely applicable.[15]
Regarding the facilities, the present study showed that shortage of educational assistive equipments and treatment facilities in hospitals, as well as shortage of educational budget were among the other challenges for the participants. Fitzgerald mentioned that shortage of educational budget results in restriction of financial resources, limitations in the number of clinical places, high number of participants who register in classes, and inadequate educational payment.[5] Ghasemi showed that if the education sessions are fitted with the ward facilities, they can promote the quality of patient care.[14] Chong pointed to costs of continuing education programs as one of the obstacles in nurses’ attendance in continuing education programs.[7] Mohamadi and Dadkha also stated that only 46.6% of participants reported that the facilities of the conference were in an appropriate level. Only 12.7% claimed that educational assistive equipments are used in education. About 75.4% believed that new books which are needed in nursing did not exist in hospitals’ libraries, and 10.1% stated that educational CDs are available for personnel.[8] Mohamadhoseini showed that 47.8% of participants believed that the place of educational classes was highly appropriate, and 47% mentioned that timely use of educational assistive equipment was highly appropriate.[15] Farmani reported average level of satisfaction with the place of educational classes. The nurses also believed facilities for attendance of learners of different shifts in educational classes are essential for promotion and efficacy of continuing education programs.[12]
Regarding evaluation, the present study showed that the participants asked for periodical evaluation, precise supervision on evaluations, measurement of the efficacy of education, and administration of a pre-test post-test in all education sessions. Falmer et al., through having group discussion sessions before suggesting the model and after that, showed that after suggesting any educational model, evaluation should be conducted about its results to declare whether it is applicable or not.[16] Bloos et al., in a descriptive study on the effect of staffs’ education on the care of patients under mechanical ventilation, showed that we can estimate the degree of achievement of the goals through a pre-test post-test, so that after implementation of any education, its results should be evaluated.[17] Latter et al., in a descriptive study on the evaluation of nurses administering medication, reported that 82% of the participants were satisfied that they were supervised by a pharmacist.[18]
In fact, nurses were frequently evaluated after education and this evaluation reinforced learning, and consequently, promotion of the quality of education.
In other words, the staffs’ practice should be supervised after education to determine whether they have achieved the educational goal or not.
CONCLUSION
This study showed that the present approach of nurses’ continuing education needs modification so as to meet nurses’ needs. Therefore, management and planning of education should be based on a new approach concentrating on nurses’ needs. Special attention should also be paid to teachers related problems. The goal can be better achieved by formation of an educational committee in hospitals, as well as in planning and evaluation teams. An educational courses logbook should be prepared in which nurses’ already passed courses can be recorded so that according to that, planning can be made for the individuals. It is suggested to design further studies in the context of management and educational planning to achieve the goal of nursing continuing education modification.
Limitations
This study was conducted among nurses and continuing education authorities in Isfahan. Although our research environment had a condition similar to many other areas in Iran, its results cannot be generalized for all nurses and education authorities.
It was tried to increase the rigor of data through numerous methods. It should be noted that our goal was not generalization of the results to other societies, although these results can be generalized to other similar societies.
ACKNOWLEDGMENT
This article was derived from a master thesis of (Marzie soleimani) with project number 391129 Isfahan University of Medical Sciences, Isfahan, Iran. The authors extend their thanks to all the participants for their valuable information.
Footnotes
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Ellis J, Hartley C. 10th ed. China: Lippincott Williams and Wilkins; 2012. Nursing in today's world Trends, issues, and management; pp. 68–71. [Google Scholar]
- 2.Yoder-Wise P. 4th ed. Carada: Mosby; 2007. Leading and managing in nursing; p. 176. [Google Scholar]
- 3.Huber DL. 3rd ed. Lowa city: Saunders; 2006. Leadership and nursing care management; p. 66. [Google Scholar]
- 4.Gallagher L. Continues education in nursing: A concept analysis. Nurse Educ Today. 2007;27:466–73. doi: 10.1016/j.nedt.2006.08.007. [DOI] [PubMed] [Google Scholar]
- 5.Fitzgerald C, Kantrowitz-Gordon I, Katz J, Hirsch A. Advanced Practice Nursing Education: Challenges and Strategies. Nurs Res Pract. 2012;2012:854918. doi: 10.1155/2012/854918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Griscti O, Jacono J. Effectiveness of continues education programmes in nursing: Literature review. J Adv Nurs. 2006;55:449–56. doi: 10.1111/j.1365-2648.2006.03940.x. [DOI] [PubMed] [Google Scholar]
- 7.Chong MC, Sellick K, Francis K, Abdullah KL. What influences Malaysian nurses to participate in continuing professional education activities? Asian Nurs Res (Korean Soc Nurs Sci) 2011;5:38–47. doi: 10.1016/S1976-1317(11)60012-1. [DOI] [PubMed] [Google Scholar]
- 8.Mohamadi A, Dadkha B. Assessment of continues education process nurse point of view in Ardebil Hospital. J Ardabil Univ Med Sci. 2005;5:271–4. [Google Scholar]
- 9.Kelly-Heidenthal P. Canada: Thomson; 2003. Nursing leadership and management. [Google Scholar]
- 10.Pretorius G, Patricia A, Morgan B. The Lived Experiences of Mothers whose Children were Sexually Abused by Their Intimate Male Partners. Indo-Pacific J Phenomenology. 2011;11:1–14. [Google Scholar]
- 11.Braun V, Clarke V. Using thematic analysis in psychology. [Last accessed on 2012 March 10];Qual Res Psycho. 2006 3:77–101. Available from: http://www.informaworld.com . [Google Scholar]
- 12.Farmani P, Zaghimi Mohamadi SH. Point of view nurses in tamin ejtemai hospital in Karaj and Shahriyar related to continues nursing education. Iran J Educ Med Sci. 2009;11:326–38. [Google Scholar]
- 13.Fairchild M, Everly M, Bozarth L, Bauer R, Walters L, Sample M, et al. A qualitative study of continues education needs of rural nursing unit staff: The nurse administrator's perspective. NET. 2012. [Last accessed on 2012 May 23]. Available from: http://www.elsevier.com/nedt . [DOI] [PubMed]
- 14.Emamzade-Ghasemi H, Vanaki Z, Memariyan Z. The effect of use nursing continues education pattern on quality of nursing care in surgery unit. Iran J Educ Med Sci. 2004;4:13–21. [Google Scholar]
- 15.Mohamadhoseini S, Karimi Z, Momeni E, Abasi A, Sadat S. Nurses point of view about continues education in kohkiloye and boyerahmad hospital. Med J Hormozgan. 2012;16:73–80. [Google Scholar]
- 16.Fulmer T, Cathcart E, Glassman K, Budin W, Naegle M, Van N. The attending Nurse: An Evolving Model for Integration Nursing Education and Practice. Open Nurse J. 2011;5:9–13. doi: 10.2174/1874434601105010009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bloos F, Muller S, Harz A. Effects of staff training on the care of mechanically ventilated patients: A prospective cohort study. Br J Anaesth. 2009;103:232–7. doi: 10.1093/bja/aep114. [DOI] [PubMed] [Google Scholar]
- 18.Latter S, Maben J, Myall M. Evaluating nurse prescribers education and coutinuing professional development for independent prescribing practice: Finding from a national survey in England. [Last accessed on 2011 Nov 30];Nurse Educ Today. 2007 27:685–96. doi: 10.1016/j.nedt.2006.10.002. Available from: http://www.intl.elsevierhealth.com/journals/nedt . [DOI] [PubMed] [Google Scholar]