

Abstract
Social support is an important extra-therapeutic context of depression treatment, yet no overall estimate is available on how depression treatment affects social support or the size of such an effect. We conducted a meta-analysis of clinical trials of psychotherapy for depression that reported results for social support at post-treatment. A total of 1,579 adults with depression from 11 trials comparing psychotherapy to care-as-usual or waiting list were included. The majority of these studies assessed the participants’ perceptions of social support. Specifically, three studies targeted women with postpartum depression, and four studies targeted individuals with chronic disease. In all these studies, psychotherapy had a small to moderate, yet consistent effect on social support compared to care-as-usual or waiting list at post-treatment (g = 0.38; 95% CI: 0.29~0.48) and at 3–6 month follow-up (g= 0.38; 95% CI: 0.14~0.63). Little evidence of heterogeneity was found across studies, and the results were consistent in several sensitivity analyses. No significant publication bias was detected (Egger’s test p > 0.1). The result of meta-regression showed that improvement in depression symptoms was associated with improvement in social support, but this was not statistically significant.
Introduction
Depression is a common (Kessler et al., 2010), disabling (Murray & Lopez, 2013), yet treatable disease (Cipriani et al., 2009; P. Cuijpers, Dekker, Hollon, & Andersson, 2009; P. Cuijpers, Smit, Bohlmeijer, Hollon, & Andersson, 2010). Psychological treatments for depression have shown comparable effect with—or, in some cases, better long-term effect than—pharmacological treatment (De Maat, Dekker, Schoevers, & De Jonghe, 2006; Imel, Malterer, McKay, & Wampold, 2008). Unfortunately, depression remains a chronic disease with high rates of recurrence. Mueller et al. (1999) concluded that up to 85% of individuals who recover from depression experience recurrence within 15 years. The likelihood of recurrence and of treatment resistance increases as the number of episodes of depression increases; an additional episode increases the risk of recurrence by 18%. Thus, there is an urgent need to identify ways to prevent relapse after the successful treatment of depression.
Existing literature (DeRubeis & Crits-Christoph, 1998; DeRubeis et al., 2005; Dobson et al., 2008; Gloaguen, Cottraux, Cucherat, & Blackburn, 1998; Kovacs, Rush, Beck, & Hollon, 1981; Paykel et al., 2005; Simons, Murphy, Levine, & Wetzel, 1986) suggests that individuals who previously received psychotherapy had generally lower rates of relapse and recurrence than those treated with antidepressants alone or care-as-usual. However, the mechanism of such an enduring effect of psychotherapy has not yet been fully examined. In the context of depression relapse and recurrence prevention, identifying factors associated with the long-term effect of depression treatment is an important and worthwhile endeavor.
Social support is an important extra-therapeutic context of depression treatment. However, the relationship between social support and the course of depression is one marked by complexity. A compelling body of evidence has shown that social support decreases the risks for depression (Lee, Crittenden, & Yu, 1996; Martire & Schulz, 2007) and depression relapse (George, Blazer, Hughes, & Fowler, 1989), increases adherence to depression treatment (Smith, Francis, Gray, Denham, & Graffy, 2003; Voils, Steffens, Flint, & Bosworth, 2005), and improves treatment outcomes. Conversely, a lack of social support generally increases the risk for depression (Hinrichsen & Emery, 2005; National Alliance for Caregiving/AARP, 2004, 2009; J. G. Sandberg & Harper, 2000; Jonathan G. Sandberg & Harper, 1999; Jonathan G. Sandberg, Miller, & Harper, 2002; Seaburn, Lyness, Eberly, & King, 2005; Talley & Crews, 2007) and relapse (Denton et al., 2010; Keitner et al., 1995) and the likelihood of poor response to treatment. Moreover, depression can disturb an individual’s existing social support system, and such a disruption can, in turn, undermine the long-term effects of depression treatment and increase the risk for relapse. Therefore, treating depression may improve social support, and improvement of social support through treatment may be related to better long-term outcome of depression treatment.
Psychotherapy has a greater potential to modify a patient’s social support than care-as-usual or pharmacotherapy. A therapist may work with (1) a patient to improve the patient’s social skills and social functioning or to amend the patient’s perception about one’s social environment, (2) a patient’s friends or family to alter the patient’s social environment (e.g., psychoeducation to help family interacts with the patient more supportively), or (3) a patient-family dyad to modify maladaptive couple or family functioning (e.g., couples therapy).
Although several studies have examined the effects of psychotherapies for depression on social support, no meta-analysis has yet integrated this research; moreover, no overall estimate is available on whether or not these treatments affect social support or the size of such an effect. This promoted us to conduct a meta-analysis of randomized clinical trials of psychotherapies, which featured social support as an outcome.
The concept of social support is heterogeneous in its definition and operationalization. Generally, social support includes three broad categories: instrumental, emotional, and informational. In addition, various instruments are available to assess the level of social support that include single-item assessment of social support availability, Likert scales for level of social support, and surveys to measure the frequency of supportive interactions with others. While the majority of these instruments assess perceived social support, other instruments assess more objective components of social support such as proximity of social support sources and size of social network (Landerman, George, Campbell, & Blazer, 1989). Still others assess both positive and negative sides of social interactions (Stansfeld & Marmot, 1992). Considering that this study is one of the first to examine the effects of psychotherapy on social support, we tried to include as many studies as possible. Therefore, we did not have inclusion or exclusion criteria regarding how social support is defined and/or assessed.
Our primary hypothesis was that psychotherapies for depression would have greater effects on social support than comparison conditions (i.e., care-as-usual, waiting lists, and pharmacotherapy). Considering the potential bi-directional relations between depression and social support, our secondary hypothesis was that the effects of psychotherapies on social support would be associated with the effects of psychotherapy on depressive symptoms.
Methods
Identification and Selection of Studies
We constructed a database of papers on the psychotherapy of depression. This database has not only been previously described in detail (P. Cuijpers, van Straten, Warmerdam, & Andersson, 2008), but also has been used in a series of earlier published meta-analyses (Pim Cuijpers et al., 2014). Additionally, this database has been continuously updated through comprehensive literature searches (from 1966 to January 2013). In these searches, we examined 14,164 abstracts from PubMed (3,638 abstracts), PsycInfo (2,824), Embase (4,682) and the Cochrane Central Register of Controlled Trials (3,020). These abstracts were located by combining terms indicative of psychological treatment and depression (i.e., both MeSH terms and text words). In constructing this database, we also checked the primary studies from 42 meta-analyses of psychotherapy for depression to ensure that no published studies were missed. From the 14,164 abstracts (10,474 after removal of duplicates), we retrieved 1,476 full-text papers for possible inclusion in the database.
We included randomized controlled trials in which (1) a psychological intervention was compared to a control condition (i.e., waiting list, care-as-usual, placebo, and other) in depressed people and (2) outcomes were reported on social support. Depression could be either defined according to diagnostic interview or based on a cut-off score on a self-report measure. We excluded studies in which the effects of two or more psychotherapies were compared to each other and to studies of inpatients and adolescents (i.e., ≤ 18 years). Comorbid general medical or psychiatric disorders were not used as an exclusion criterion.
We also wanted to include not only studies in which psychotherapy was compared to pharmacotherapy, but also studies comparing combined treatment with either psychotherapy alone or pharmacotherapy alone. Although we identified 79 studies examining one or more of these comparisons, none of them included social support as an outcome measure. Therefore, we did not include these studies in our meta-analysis.
Quality Assessment and Data Extraction
We assessed the validity of included studies in the meta-analysis using four criteria from the ‘Risk of bias’ assessment tool developed by the Cochrane Collaboration. This tool assesses possible sources of bias in randomized trials including (1) the adequate generation of allocation sequence, (2) the concealment of allocation to conditions, (3) the prevention of knowledge of the allocated intervention (i.e., masking of assessors), and (4) the treatment of incomplete outcome data, which was assessed as positive when intention-to-treat analyses were conducted (i.e., all randomized patients were included in the analyses).
We also coded additional aspects of the studies, which included (a) participant characteristics (i.e., recruitment method [e.g., community, clinical samples, or other] and definition of depression [e.g., diagnosed depressive disorder or scoring above a cut-off on a self-rating depression scale]), (b) intervention characteristics (i.e., format [e.g., individual, group, or guided self-help], number of sessions, and type of psychotherapy), and (c) study characteristics (i.e., type of control group [e.g., care-as-usual or other]).
Meta-Analyses
All measures of social support were pooled into one effect size (Hedges’s g), which indicates the difference in social support between a group receiving a particular psychotherapy protocol and a control group at post-test and at follow-up (1–3 months and 6–12 months). Hedges’s g was calculated by subtracting the average score of the psychotherapy group from the average score of the control group and dividing the result by the pooled standard deviation.
We also calculated the Hedges’s g for the effects of the treatments on depression. In these calculations, we used only those instruments that explicitly measured symptoms of depression such as the Beck Depression Inventory (Beck, Steer, & Carbin, 1988) or the Hamilton Rating Scale for Depression (HAM-D). If dichotomous outcomes were reported without means and standard deviations, we used the following procedures (Comprehensive Meta-Analysis software version 2.2.021) to calculate the standardized mean difference. Binary results were first converted to log odds ratios and then to standardized mean differences (Cohen’s d). This Cohen’s d was then converted into bias-corrected standardized mean differences (Hedges’s g). Because we expected considerable heterogeneity among the studies, we employed a random effects pooling model.
As a test of homogeneity of effect sizes, we calculated the I2 statistic as an indicator of heterogeneity in percentages. A value of 0% indicates no observed heterogeneity, and larger values indicate increasing heterogeneity, with 25% as low, 50% as moderate, and 75% as high heterogeneity. We calculated 95% confidence intervals (CI) around I2 (Higgins & Thompson, 2002), using the non-central chi-squared-based approach within the heterogi module for Stata. We conducted several sensitivity analyses. Using leave-one out analyses (Wallace, Schmid, Lau, & Trikalinos, 2009), we examined the magnitude of influence of each study on pooled effect size. Because several studies had relatively small sample sizes, we corrected Hedges’s g for small sample bias according to the procedures suggested by Hedges and Olkin (1985). If more than one measure of social support was reported in the study, we pooled the outcomes within the study before pooling the outcomes across studies.
Subgroup analyses were conducted according to the mixed effects model (Borenstein, Hedges, Higgins, & Rothstein, 2009) in which studies within subgroups are pooled with the random effects model, while tests for significant differences between subgroups are conducted with the fixed effects model. For continuous variables, we used meta-regression analyses according to the procedures described by Borenstein et al. (2009) to test whether or not there was a significant relation between the continuous variable and effect size.
Publication bias was tested by inspecting the funnel plot (Sterne & Egger, 2001) on primary outcome measures and by Duval and Tweedie’s (2000) trim and fill procedure, which yields an estimate of the effect size after the publication bias has been taken into account. We also conducted Egger’s test of the intercept to quantify the bias captured by the funnel plot and tested whether or not it was significant.
Results
Characteristics of Included Studies
Figure 1 presents the study selection process for our meta-analysis. Eleven studies met the inclusion criteria and were, therefore, included in our meta-analysis. Characteristics of these studies are presented in Table 1. Among the eleven studies, 1,579 patients participated (i.e., 888 in the treatment groups and 691 in the control groups). One of these studies (Rahman, Malik, Sikander, Roberts, & Creed, 2008) included more participants (n = 818) than the rest of the trials combined (n = 761). This trial was also the only cluster-randomized trial, with communities randomized to either the intervention or control condition.
Figure 1.

Flowchart of inclusion of studies
Table 1.
Selected Characteristics of Randomized Controlled Trial of Psychotherapy for Adult Depression Reporting Outcomes on Social Support
| Recr | Diagnosis | Target group | Therapy | Form | Nse | N | Control | N | Quala) | Social support measure | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Allart, 2003 | Community | BDI score ≥ 10, no MDD | Adults in general | CBT | grp | 12 | 61 | CAU | 41 | − − + − | Social Support List (SSL)–interaction and perception |
| Chen, 2000 | Postnatal wards at 2 hospitals | BDI score ≥ 10 | Women with PPD | SUP | grp | 4 | 30 | CAU | 30 | − − + − | Interpersonal Support Evaluation List (ISEL) Short Form |
| Chesney, 2003 | Community | CES-D score ≥ 10, no MDD | Men living with HIV | CBT | grp | 10 | 46 | WL | 38 | − − + − | Social Relationships Scale |
| Cramer, 2011 | Community | PHQ-9 score 10–24 | Women aged 30–55 | CBT | grp | 12 | 46 | CAU | 19 | + + + + | Medical Outcomes Study Social Support Survey |
| Dobkin, 2011 | Community | Mood disorder | Patients with | CBT | ind | 10 | 41 | CAU | 39 | + + + + | Social Feedback |
| Evans, 1995 | Through hospital | (SCID) CES-D score ≥ 16 | Parkinson’s Disease Cancer patients | CBT | grp | 8 | 27 | CAU | 24 | − − + − | Questionnaire Social provisions scale |
| Forsyth, 2000 | Through university classes | BDI score 10–29 (no current mood disorder) | Students at risk for depression | SUP | grp | 8 | 21 | WL | 28 | − − + − | Interpersonal Support Evaluation List (ISEL) |
| IPT | grp | 4 | 31 | ||||||||
| Kelly, 1993 | Community | CES-D score ≥ 16 | Men living with HIV | CBT | grp | 8 | 27 | CAU | 27 | − − + − | Social provisions scale |
| SUP | grp | 8 | 14 | ||||||||
| Milgrom, 2005 | Community screening program | Mood disorder (CIDI) | Women with PPD | CBT | ind | 6 | 31 | CAU | 18 | + + − + | Social provisions scale |
| SUP | grp | 6 | 34 | + + − + | |||||||
| SUP | ind | 6 | 38 | + + − + | |||||||
| Mulcahy, 2010 | Referrals from clinicians | MDD (MCMI-III) | Women with PPD | IPT | grp | 11 | 23 | CAU | 27 | + − + − | Interpersonal Support Evaluation List (ISEL) |
| Rahman, 2008 | Through community health workers | MDD (SCID) | Women with PPD | CBT | grp | 8 | 418 | CAU | 400 | + + + + | Multidimensional scale for perceived social support |
In this column a positive or negative sign is given for four quality criteria, respectively: allocation sequence; concealment of allocation to conditions; blinding of assessors; and intention-to-treat analyses.
Abbreviations: BDI: Beck Depression Inventory; CAU: care-as-usual; CBT: cognitive behavior therapy; CES-D: center for epidemiological studies depression scale; CIDI: Compositve International Diagnostic Interview; Form: treatment format; grp: group format; Ind: individual treatment format; IPT: interpersonal psychotherapy; MCMI-III: Millon Clinical Multiaxial Inventory-III; MDD: major depressive disorder; Nse: number of sessions; PHQ: patient health questionnaire; PPD: postpartum depression; SCID: Structured Clinical Interview for DSMIV; SUP: non-directive supportive counseling; WL: waiting list.
Four studies were specifically aimed at women with postpartum depression, four were aimed at patients with medical conditions (i.e., HIV, Parkinson’s disease, and cancer) and the remaining three studies were aimed at other populations (i.e., adults in general, women aged 30–55, and students at risk for depression). In four of the studies, participants were required to meet diagnostic criteria for a depressive disorder; in four of the other studies, participants were included if they scored above a cut-off on a self-report measure; the remaining three studies targeted participants with subclinical depression (i.e., individuals who scored above a cut-off on a self-report measure and met the diagnostic criteria for a depressive disorder were excluded from the study). Care-as-usual control groups were used in nine of the studies; the other two studies featured a waiting-list control group.
In the eleven studies, a total of fifteen psychotherapies were assessed relative to a control group. Eight of these therapies were cognitive-behavioral, five were non-directive counseling, and two were interpersonal psychotherapy. In twelve of the therapies, a group format was used, and three of the therapies featured an individual treatment format. The number of therapy sessions ranged from four to twelve.
Social Support Measures
Measures of social support used in the studies included in our meta-analysis are summarized in Table 1. Three of the studies (Evans & Connis, 1995; Kelly et al., 1993; Milgrom, Negri, Gemmill, McNeil, & Martin, 2005) used the original or an adapted version of the Social Provision Scale, a 24-item Likert scale that assesses six dimensions of perceived social support: social attachment, social integration, reassurance of worth, reliable alliance with others, guidance, and nurturance of others. Three of the studies (Chen, Tseng, Chou, & Wang, 2000; Forsyth, 2000; Mulcahy, Reay, Wilkinson, & Owen, 2010) featured the Interpersonal Support Evaluation List (ISEL), which measured four dimensions of social support: tangible aid, appraisal, self-esteem, and belonging. Allart et al. (2003) used two sub-scales of the Social Support List (SSL). The SSL–Perception subscale was used to measure perceived support in case of problems and perceived negative support; the SSL—Interaction subscale was used to measure frequency of supportive interaction. Chesney et al. (2003) modified the Social Relationships Scale to assess emotional and material support, affirmation, and subjective and objective social integration. Cramer et al. (2011) used a shortened Medical Outcome Study (MOS) Social Support Survey. The full-length MOS Social Support Survey is a 19-item self-report assessing four domains of social support (i.e., emotional/informational support, instrumental support, positive social interaction, and affection), and the authors did not clarify how they modified the MOS social support survey for use in their study. Finally, Rahman et al. (2008) used the Multidimensional scale for perceived social support, which is a 12-item self-report assessment tool, and Dobkin et al. (2011) used the Social Feedback Questionnaire.
Quality of the Studies Included in the Current Meta-Analyses
The quality of the included studies varied. Five studies reported an adequate sequence generation. Four studies reported allocation to conditions by an independent (third) party. Ten studies reported blinding of outcome assessors and in four studies intention-to-treat analyses were conducted. Three studies met all four quality criteria, two met two or three criteria, and the remaining six studies had a lower quality (i.e., none or only one of the four criteria were met).
Effects on Social Support
The overall effect size (i.e., Hedges’s g) indicating the difference between the treatment and control groups on social support outcomes was 0.38 (95% CI: 0.29~0.48)(Table 2). Heterogeneity was zero, but the 95% CI was broad (0~54%). The forest plot of effect sizes is provided in Figure 2.
Table 2.
Effects of psychological treatments of adult depression on social support: Hedges’ g
| N | g | 95% CI | I2 | 95% CI | pa) | ||
|---|---|---|---|---|---|---|---|
| All studies: effects on social support | 15 | 0.38 | 0.29~0.48 | 0 | 0~54 | ||
| Sensitivity analyses | |||||||
| One effect size per study (only highest) | 11 | 0.40 | 0.30~0.51 | 0 | 0~60 | ||
| One effect size per study (only lowest) | 11 | 0.37 | 0.27~0.48 | 0 | 0~60 | ||
| One large study excluded (Rahman et al., 2008) | 14 | 0.31 | 0.18~0.45 | 0 | 0~55 | ||
| Only Social Provisions Scale | 7 | 0.33 | 0.11~0.54 | 0 | 0~71 | ||
| Only Interpersonal Support Evaluation List (ISEL) | 3 | 0.56 | 0.25~0.86 | 0 | 0~90 | ||
| Subgroup analyses | |||||||
| Target group | - Women with PPD | 6 | 0.47 | 0.34~0.59 | 0 | 0~75 | 0.08 |
| - General medical | 6 | 0.20 | −0.00~0.41 | 0 | 0~75 | ||
| - Other | 3 | 0.29 | 0.02~0.56 | 15 | 0~91 | ||
| Depression | - Diagnosis | 7 | 0.44 | 0.32~0.55 | 0 | 0~71 | 0.11 |
| - High score | 8 | 0.26 | 0.09~0.44 | 0 | 0~68 | ||
| Type of psychotherapy | - CBT | 8 | 0.36 | 0.25~0.47 | 0 | 0~68 | 0.70 |
| - Supportive counseling | 5 | 0.46 | 0.21~0.71 | 0 | 0~79 | ||
| - IPT | 2 | 0.47 | 0.10~0.85 | 0 | b) | ||
| Format | - Group | 12 | 0.38 | 0.28~0.49 | 0 | 0~58 | 1.00 |
| - Individual | 3 | 0.38 | 0.09~0.68 | 18 | 0~91 | ||
| Control group | - Care-as-usual | 13 | 0.38 | 0.28~0.49 | 0 | 0~57 | 0.98 |
| - Waiting list | 2 | 0.38 | 0.05~0.71 | 30 | b) | ||
| Study quality | - 0–2 | 9 | 0.32 | 0.16~0.49 | 0 | 0~65 | 0.39 |
| - 3–4 | 6 | 0.41 | 0.30~0.53 | 1 | 0~75 | ||
| Effect on depression | |||||||
| All studies | 15 | 0.68 | 0.52~0.85 | 49 | 0~72 | ||
| Sensitivity analyses | |||||||
| One effect size per study (only highest) | 11 | 0.73 | 0.51~0.95 | 63 | 29~81 | ||
| One effect size per study (only lowest) | 11 | 0.65 | 0.44~0.85 | 60 | 23~79 | ||
| One large study excluded (Rahman et al., 2008) | 14 | 0.69 | 0.50~0.90 | 52 | 12~74 | ||
| Long-term outcomes | |||||||
| Effect on social support at 1–3 months | 6 | 0.38 | 0.14~0.63 | 30 | 0~71 | ||
| Effect on social support at 6–12 months | 5 | 0.32 | −0.00~0.64 | 67 | 13~87 | ||
the p-value in this column indicates whether the subgroups differ significantly from each other.
In subgroups with two studies the 95% CI of I2 cannot be calculated
Figure 2.

Effects of psychological treatment of adult depression on social support: Hedges’ g
In three of the studies, more than one psychological intervention was compared to the same control group. Because these effect sizes are not independent of each other, they may artificially reduce heterogeneity and influence the effect size. Therefore, we conducted a sensitivity analysis in which we included only one effect size (i.e., the largest effect size) per study. We then conducted another analysis in which we included only the smallest effect size. As can be seen from Table 2, this procedure did not influence the overall mean effect size or levels of heterogeneity.
Because we included one very large study (Rahman et al., 2008), we also conducted another sensitivity analysis in which we removed this study (Table 2). Although the overall effect size was somewhat smaller than the overall effect size, the difference was small, and the effect size still differed significantly from zero.
We conducted 15 separate leave-one-out analyses, in which each of studies is left out once (Table 3). When Dobkin et al. (2011)’s study was left out; the pooled effect size was increased to 0.40. When Rahman et al (2008)’s study was left out; the pooled effect size was decreased to 0.31. These are the two studies with the highest impact on the overall result.
Table 3.
Leave-one-out analyses
| g | Lower limit | Higher limit | p | |
|---|---|---|---|---|
| Allart, 2003 | 0,39 | 0,29 | 0,50 | 0,00 |
| Chen, 2000 | 0,37 | 0,27 | 0,47 | 0,00 |
| Chesney, 2003 | 0,39 | 0,29 | 0,49 | 0,00 |
| Cramer, 2011 | 0,40 | 0,30 | 0,49 | 0,00 |
| Dobkin, 2011 | 0,40 | 0,30 | 0,50 | 0,00 |
| Evans, 1995 cbt | 0,39 | 0,29 | 0,49 | 0,00 |
| Evans, 1995 sup | 0,38 | 0,28 | 0,48 | 0,00 |
| Forsyth, 2000 | 0,38 | 0,28 | 0,47 | 0,00 |
| Kelly, 1993 cbt | 0,39 | 0,29 | 0,49 | 0,00 |
| Kelly, 1993 sup | 0,39 | 0,29 | 0,49 | 0,00 |
| Milgrom, 2005 cbt | 0,38 | 0,28 | 0,48 | 0,00 |
| Milgrom, 2005 group | 0,39 | 0,29 | 0,49 | 0,00 |
| Milgrom, 2005 ind | 0,38 | 0,28 | 0,48 | 0,00 |
| Mulcahy, 2010 | 0,39 | 0,29 | 0,49 | 0,00 |
| Rahman, 2008 | 0,31 | 0,18 | 0,45 | 0,00 |
|
| ||||
| POOLED | 0,38 | 0,29 | 0,48 | 0,00 |
Because certain measures of social support might have been more sensitive to the changes in this social support over time than others, we conducted sensitivity analysis comparing the effect size of studies using the Social Provision Scale (Evans & Connis, 1995; Kelly et al., 1993; Milgrom et al., 2005) with those using ISEL (Chen et al., 2000; Forsyth, 2000; Mulcahy et al., 2010). The former studies appear to have smaller effect size compared to the latter (g = 0.33; 95% CI: 0.11~0.54 vs. g = 0.56; 95% CI: 0.25~0.86).
In six of the studies (Chesney et al., 2003; Cramer et al., 2011; Forsyth, 2000; Kelly et al., 1993; Mulcahy et al., 2010; Rahman et al., 2008), outcomes on social support at 1- to 3-month follow-up were reported (Table 2). The effect on social support (i.e., Hedges’s g) was 0.38 (95% CI: 0.14~0.63; p < 0.05), with low heterogeneity. The five studies (Chesney et al., 2003; Cramer et al., 2011; Evans & Connis, 1995; Kelly et al., 1993; Rahman et al., 2008) reporting outcomes at 6 to 12 month follow-up resulted in an effect size on social support of 0.32 (95% CI: -0.00~0.64). This was not significant (p = 0.51). Heterogeneity was moderate to high.
Subgroup Analyses
Although the number of studies was limited, we nonetheless conducted a small number of moderator analyses to examine whether or not the effect sizes differed in specific subsets of studies. We found no indication that target group, depression diagnosis, type of psychotherapy, treatment format, type of control group, or study quality was significantly associated with the effect size (Table 2). However, this may have been caused by the limited statistical power to find significant differences between subgroups.
Effects on Depression
We also calculated the effects of the interventions on depression (Table 2). The overall effect size (i.e., Hedges’s g) was 0.68 (95% CI: 0.50~0.86) with moderate heterogeneity (I2 = 54; 95% CI: 14~75). We did conduct the same sensitivity analyses as we did with the outcomes on social support, but we did not find that the inclusion of multiple comparisons from one study or the exclusion of the large study significantly affected the overall outcomes.
We also conducted a meta-regression analysis with the effects on social support as the dependent variable and the effects on depression as the predictor, but we did not find that depression was a significant predictor of social support (slope = 0.13; 95% CI: −0.21~0.48; p = 0.44; Figure 3).
Figure 3.
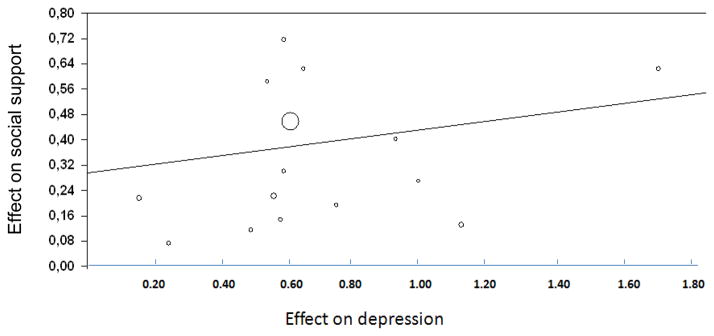
Regression of effect on depression on effect on social support
Publication Bias
Figure 4 illustrates the results of the funnel plot using Duval and Tweedie’s (2000) procedure. First, upon visual inspection, we did not observe notable asymmetry in the shape of forest plot. Duval & Tweedie’s (2000) trim and fill analysis further suggested that zero studies were missing. Additionally, the result of Egger's regression intercept approach was not significant (p > 0.1).
Figure 4.

Funnel Plot
Discussion
The central finding of this study is that psychotherapies had a small to moderate yet consistent effect on social support compared to care-as-usual or waiting list at post-treatment and 1 to 3 month follow-up. Similar magnitudes of effect were observed at 6 to 12 month follow-up, although this was not statistically significant. Little evidence for heterogeneity was found across studies, and the results were consistent in several sensitivity tests, which included the leave-one-out analyses. Our findings, however, suggest that the conceptualization and measurement of social support may have affected the effect size of social support. Our results were also consistent when examining the following potential moderators: target group, measures of depression, type of psychotherapy, format, types of control group, and study quality. We found no evidence for publication bias. As mentioned earlier, due to the lack of trials that met the inclusion criteria, we could not compare the effects of psychotherapies and of pharmacotherapies on social support.
We hypothesized that improvements in social support would be associated with improvement in depressive symptoms through psychological treatment. This hypothesis was not supported from the results of our analysis: we did not find statistically significant associations between support and symptom improvements. This counterintuitive result could have stemmed from relations between the severity of depressive symptom and the social support being mediated by social functioning. Additionally, the number of studies included in our meta-analysis may have been too small to allow sufficient statistical power to test such relations. Renner et al.’s (2014) recent meta-analysis of 31 clinical trials demonstrated that psychotherapy for depression was associated with improved social functioning. Furthermore, depressive symptoms and social support may be confounded by demographic characteristics such as gender and ethnicity, and these gender and ethnic variations are difficult to examine with study-level meta-analyses.
Depressed individuals tend to perceive their social support more negatively and/or underestimate the level of existing support. Improvement in mood may improve the perceived level of social support. Some researchers have suggested that the perceived level of social support maybe more important to an individual’s mental health than the objective level of social support. However, in our meta-analysis, we cannot make a conclusion about whether or not the form of psychotherapy is the only impact on perceived level of social support because the majority of studies measured perceived social support. Only Allart-van Dam et al. (2003) measured both subjective and objective dimensions of social support.Allart-van Dam et al. (2003) concluded that, compared to the control group, the CBT group showed a significant improvement in the frequency of supportive interaction (SSL-I) but no significant changes in perceive social support scores (SSL-P). Further research is needed to examine the underlying mechanisms of how psychotherapy affects different dimensions of social support.
In the studies featured in our meta-analysis, different psychological treatments were developed based on diverse theoretical frameworks. Additionally, relationship-oriented treatment modalities, such as IPT or couples therapy, may have greater effects on social support compared to individual-oriented CBTs. Unfortunately, no studies on couples therapies were identified in our meta-analysis. Only 2 of the 11 studies included in our meta-analysis had specific social support components in their intervention: Dokin et al. (2011) included separate caregiver education sessions for patients with Parkinson’s disease, and Milgrom et al. (2005) included sessions for partners. However, the specifics of these sessions were not described. Two studies (Allart-van Dam et al., 2003; Milgrom et al., 2005) used a modified version of Coping with Depression (Lewinsohn, Antonuccio, Steinmetz, & Teri, 1984). Two studies (Cramer et al., 2011; Evans & Connis, 1995) used CBT with a specific focus on problem solving approaches. The remaining studies included sessions on adjusting to motherhood for new mothers (Chen et al., 2000; Milgrom et al., 2005; Mulcahy et al., 2010) or managing disease for individuals with chronic conditions (Chesney et al., 2003; Dobkin et al., 2011; Evans & Connis, 1995; Kelly et al., 1993).
In the sub-group analysis of our study, the effect sizes for counseling and IPT were greater compared to CBT (.50, .47, and .37, respectively). However, these differences were not statistically significant, and the 95% CI range was quite wide. The effect size of the 12 group therapy studies was similar to the one of the three individual therapy studies (g = 0.38 vs. 0.38; p = 1.00). The lack of statistical significance and the unstable point estimates for these subgroups may be due to the small sample sizes. Future studies with larger sample sizes may generate different results.
Our study has several limitations. First, despite our best efforts to capture all relevant publications, we may have overlooked studies that (1) are published in journals that are not indexed in the databases we used to conduct searches, (2) are published in non-journal venues, or (3) have been recently published. However, as mentioned earlier, we found no indication of publication bias. Second, we pooled the treatment outcomes assessed using different measurement tools that may have different sensitivities and specificities. There were, however, insufficient descriptions in the studies about modified and/or shortened social support measures. Moreover, the conceptualizations of social support were not uniform among the studies, and effect sizes were estimated using different covariates. Collectively, these limitations may have increased the risk for heterogeneity. Nonetheless, the lack of heterogeneity and of variation in the sensitivity tests suggests that these differences in controlling for potential confounders across studies are unlikely to have weakened our findings. Third, the studies included in our analysis are those of special circumstances; therefore, our findings may have limited applicability to the general population. Four of the studies targeted women with or at high risk for postpartum depression, and another four included individuals living with chronic disease (i.e., HIV, Parkinson’s disease, and cancer). Nonetheless, our findings still hold clinical and scientific significance because individuals in these special circumstances experience increased risks for developing depression (Bennett, Einarson, Taddio, Koren, & Einarson, 2004; Ciesla & Roberts, 2001; Massie, 2004), greater cumulative burden of depression (Arun, Bharath, Pal, & Singh, 2011; Do et al., 2014), and can benefit from receiving social support.
Despite its limitations, our study contributes significantly to the literature on social support and depression. First, this is the first meta-analysis to estimate the effect of psychotherapy on social support. We found not only that psychological depression treatment has positive effects on social support, but also that such effects were not significantly associated with improvements of depressive symptoms. Second, this study revealed paucities of data in several important areas of depression care. Despite the robust evidence in the literature for the positive impact of social support on treatment adherence and on treatment outcomes, we found that surprisingly few studies have examined how depression treatments affected dimensions of the patients’ social support systems. Among the 1,476 studies screened for possible inclusion in our meta-analysis, only eleven studies met the inclusion criteria regarding outcomes being reported on social support. This sort of information deficit limits our ability to elucidate the underlying mechanisms of how and why psychotherapies have better long-term depression treatment outcomes. Moreover, there was insufficient information to establish the comparative efficacy on social support among the various depression treatment modalities. For example, due to the lack of data, we could not compare the effects on social support between psychotherapies and pharmacotherapies or between individual-psychotherapies and family/couples therapies. One advantage of psychotherapy over pharmacotherapy is its flexibility regarding the target of treatment (i.e., patient, patient’s family, and patient-family dyad). Moreover, working with the patient-family dyad to modify maladaptive functioning could be an ideal strategy to improve social support and prolong the effect of the depression treatment. (Barbato & D'Avanzo, 2008) meta-analysis concluded that although marital therapy had equal effects on treating depression compared to individual-psychotherapy or pharmacotherapy, it had better effect on improving relationship of distressed couple. However, Barbato and D'Avanzo (2008) did not examine whether or not marital therapy had better long-term effect on depression compared to individual-psychotherapy or pharmacotherapy. This absence of data on the comparative efficacy of diverse therapeutic modalities for depression limits our ability to identify the best strategies for depression treatment and relapse prevention that are tailored for given patient characteristics—a clinically and theoretically important question. Therefore, future studies should include secondary outcomes associated with social support and social functioning. Finally, as mentioned earlier, although social support comprises several components, the majority of studies included in this meta-analysis exclusively targeted perceived social support. Although we were unable to compare how different measures of social support impacted the overall effect sizes of psychotherapy on social support, the effect size of ISEL was greater compared to studies using SPS. In addition, multi-component approaches to measuring social support may also significantly enhance our understanding of underlying mechanisms of how psychotherapies improve social support
Conclusion
The results of this meta-analysis provide evidence that psychotherapy has small to moderate—yet consistent—effect on social support compared to care-as-usual or waiting list. Moreover, despite robust evidence in the existing literature to support the importance of social support on an individual’s mental health, few studies have measured the impact of psychosocial treatment on social support. Further studies are needed to examine the underlying mechanism of how and why psychotherapies improve social support and supply long-term effects.
Footnotes
Ethical Standards and Declarations
Conflict of Interest: All authors declare that they have no conflicts of interest. Charles F. Reynolds III is supported by the National Institutes of Health through Grant Numbers P60 MD000207; P30MH090333; UL1RR024153, UL1TR000005; and the UPMC Endowment in Geriatric Psychiatry
Informed Consent: We used published data and do not include human subjects.
References
- Allart-van Dam Esther, Hosman Clemens MH, Hoogduin Cees AL, Schaap Cas PDR. The coping with depression course: Short-term outcomes and mediating effects of a randomized controlled trial in the treatment of subclinical depression. Behavior Therapy. 2003;34(3):381–396. doi: 10.1016/s0005-7894(03)80007-2. [DOI] [Google Scholar]
- Arun MP, Bharath S, Pal PK, Singh G. Relationship of depression, disability, and quality of life in Parkinson's disease: a hospital-based case-control study. Neurol India. 2011;59(2):185–189. doi: 10.4103/0028-3886.79133. [DOI] [PubMed] [Google Scholar]
- Barbato A, D'Avanzo B. Efficacy of couple therapy as a treatment for depression: a meta-analysis. Psychiatr Q. 2008;79(2):121–132. doi: 10.1007/s11126-008-9068-0. [DOI] [PubMed] [Google Scholar]
- Beck Aaron T, Steer Robert A, Carbin Margery G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review. 1988;8(1):77–100. [Google Scholar]
- Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic review. Obstet Gynecol. 2004;103(4):698–709. doi: 10.1097/01.AOG.0000116689.75396.5f. [DOI] [PubMed] [Google Scholar]
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. Chichester UK: Wiley; 2009. [Google Scholar]
- Chen CH, Tseng YF, Chou FH, Wang SY. Effects of support group intervention in postnatally distressed women. A controlled study in Taiwan. J Psychosom Res. 2000;49(6):395–399. doi: 10.1016/s0022-3999(00)00180-x. http://dx.doi.org/10.1016/S0022-3999(00)00180-X. [DOI] [PubMed] [Google Scholar]
- Chesney MA, Chambers DB, Taylor JM, Johnson LM, Folkman S. Coping effectiveness training for men living with HIV: results from a randomized clinical trial testing a group-based intervention. Psychosom Med. 2003;65(6):1038–1046. doi: 10.1097/01.psy.0000097344.78697.ed. [DOI] [PubMed] [Google Scholar]
- Ciesla Jeffrey A, Roberts John E. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. American Journal of Psychiatry. 2001;158(5):725–730. doi: 10.1176/appi.ajp.158.5.725. [DOI] [PubMed] [Google Scholar]
- Cipriani Andrea, Furukawa Toshiaki A, Salanti Georgia, Geddes John R, Higgins Julian, Churchill Rachel, McGuire Hugh. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. The Lancet. 2009;373(9665):746–758. doi: 10.1016/S0140-6736(09)60046-5. [DOI] [PubMed] [Google Scholar]
- Cramer Helen, Salisbury Chris, Conrad Joel, Eldred James, Araya Ricardo. Group cognitive behavioural therapy for women with depression: pilot and feasibility study for a randomised controlled trial using mixed methods. BMC Psychiatry. 2011;11(1):82. doi: 10.1186/1471-244X-11-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuijpers P, Dekker J, Hollon SD, Andersson G. Adding psychotherapy to pharmacotherapy in the treatment of depressive disorders in adults: a meta-analysis. J Clin Psychiatry. 2009;70(9):1219–1229. doi: 10.4088/JCP.09r05021. [DOI] [PubMed] [Google Scholar]
- Cuijpers P, Smit F, Bohlmeijer E, Hollon SD, Andersson G. Efficacy of cognitive-behavioural therapy and other psychological treatments for adult depression: meta-analytic study of publication bias. Br J Psychiatry. 2010;196(3):173–178. doi: 10.1192/bjp.bp.109.066001. [DOI] [PubMed] [Google Scholar]
- Cuijpers P, van Straten A, Warmerdam L, Andersson G. Psychological treatment of depression: a meta-analytic database of randomized studies. BMC Psychiatry. 2008;8(1):36. doi: 10.1186/1471-244X-8-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuijpers Pim, Karyotaki Eirini, Weitz Erica, Andersson Gerhard, Hollon Steven D, van Straten Annemieke. The effects of psychotherapies for major depression in adults on remission, recovery and improvement: A meta-analysis. Journal of Affective Disorders. 2014;159:118–126. doi: 10.1016/j.jad.2014.02.026. [DOI] [PubMed] [Google Scholar]
- De Maat Saskia, Dekker Jack, Schoevers Robert, De Jonghe Frans. Relative efficacy of psychotherapy and pharmacotherapy in the treatment of depression: A meta-analysis. Psychotherapy Research. 2006;16(5):566–578. [Google Scholar]
- Denton WH, Carmody TJ, Rush AJ, Thase ME, Trivedi MH, Arnow BA, Keller MB. Dyadic discord at baseline is associated with lack of remission in the acute treatment of chronic depression. Psychological Medicine. 2010;40(03):415–424. doi: 10.1017/S0033291709990535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeRubeis Robert J, Crits-Christoph Paul. Empirically supported individual and group psychological treatments for adult mental disorders. Journal of Consulting and Clinical Psychology. 1998;66(1):37. doi: 10.1037//0022-006x.66.1.37. [DOI] [PubMed] [Google Scholar]
- DeRubeis Robert J, Hollon Steven D, Amsterdam Jay D, Shelton Richard C, Young Paula R, Salomon Ronald M, Brown Laurel L. Cognitive therapy vs medications in the treatment of moderate to severe depression. Archives of General Psychiatry. 2005;62(4):409. doi: 10.1001/archpsyc.62.4.409. [DOI] [PubMed] [Google Scholar]
- Do Ann N, Rosenberg Eli S, Sullivan Patrick S, Beer Linda, Strine Tara W, Schulden Jeffrey D, Skarbinski Jacek. Excess Burden of Depression among HIV-Infected Persons Receiving Medical Care in the United States: Data from the Medical Monitoring Project and the Behavioral Risk Factor Surveillance System. PLoS ONE. 2014;9(3):e92842. doi: 10.1371/journal.pone.0092842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dobkin Roseanne D, Menza Matthew, Allen Lesley A, Gara Michael A, Mark Margery H, Tiu Jade, Friedman Jill. Cognitive behavior therapy for depression in Parkinson’s disease: A randomized controlled trial. The American journal of psychiatry. 2011;168(10):1066. doi: 10.1176/appi.ajp.2011.10111669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dobson Keith S, Hollon Steven D, Dimidjian Sona, Schmaling Karen B, Kohlenberg Robert J, Gallop Robert J, Jacobson Neil S. Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the prevention of relapse and recurrence in major depression. Journal of Consulting and Clinical Psychology. 2008;76(3):468–477. doi: 10.1037/0022-006x.76.3.468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duval Sue, Tweedie Richard. Trim and Fill: A Simple Funnel-Plot–Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics. 2000;56(2):455–463. doi: 10.1111/j.0006-341X.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- Evans RL, Connis RT. Comparison of brief group therapies for depressed cancer patients receiving radiation treatment. Public Health Rep. 1995;110(3):306–311. [PMC free article] [PubMed] [Google Scholar]
- Forsyth K. The design and implementation of a depression prevention program (Unpublished doctoral dissertation) University of Rhode Island; 2000. [Google Scholar]
- George LK, Blazer DG, Hughes DC, Fowler N. Social support and the outcome of major depression. Br J Psychiatry. 1989;154(4):478–485. doi: 10.1192/bjp.154.4.478. [DOI] [PubMed] [Google Scholar]
- Gloaguen V, Cottraux J, Cucherat M, Blackburn IM. A meta-analysis of the effects of cognitive therapy in depressed patients. J Affect Disord. 1998;49(1):59–72. doi: 10.1016/s0165-0327(97)00199-7. [DOI] [PubMed] [Google Scholar]
- Hedges LV, Olkin I. Statistical methods for meta-analysis. San Diego, CA: Academic Press; 1985. [Google Scholar]
- Higgins Julian PT, Thompson Simon G. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine. 2002;21(11):1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- Hinrichsen Gregory A, Emery Erin E. Interpersonal Factors and Late-Life Depression. Clinical Psychology: Science and Practice. 2005;12(3):264–275. doi: 10.1093/clipsy.bpi027. [DOI] [Google Scholar]
- Imel Zac E, Malterer Melanie B, McKay Kevin M, Wampold Bruce E. A meta-analysis of psychotherapy and medication in unipolar depression and dysthymia. Journal of Affective Disorders. 2008;110(3):197–206. doi: 10.1016/j.jad.2008.03.018. [DOI] [PubMed] [Google Scholar]
- Keitner GI, Ryan CE, Miller IW, Kohn R, Bishop DS, Epstein NB. Role of the family in recovery and major depression. Am J Psychiatry. 1995;152(7):1002–1008. doi: 10.1176/ajp.152.7.1002. [DOI] [PubMed] [Google Scholar]
- Kelly Jeffrey A, Murphy Debra A, Bahr Richard, Kalichman Seth C, Morgan Michael G, Stevenson Yvonne S, Bernstein Barry M. Outcome of cognitive-behavioral and support group brief therapies for depressed, HIV-infected persons. Am J Psychiatry. 1993;150(1):1679–1686. doi: 10.1176/ajp.150.11.1679. [DOI] [PubMed] [Google Scholar]
- Kessler Ronald C, Birnbaum Howard G, Shahly Victoria, Bromet Evelyn, Hwang Irving, McLaughlin Katie A, Stein Dan J. Age differences in the prevalence and co-morbidity of DSM-IV major depressive episodes: results from the WHO World Mental Health Survey Initiative. Depression and Anxiety. 2010;27(4):351–364. doi: 10.1002/da.20634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kovacs Maria, Rush A John, Beck Aaron T, Hollon Steven D. Depressed outpatients treated with cognitive therapy or pharmacotherapy: a one-year follow-up. Archives of General Psychiatry. 1981;38(1):33. doi: 10.1001/archpsyc.1981.01780260035003. [DOI] [PubMed] [Google Scholar]
- Landerman Richard, George Linda K, Campbell Richard T, Blazer Dan G. Alternative models of the stress buffering hypothesis. American Journal of Community Psychology. 1989;17(5):625–642. doi: 10.1007/BF00922639. [DOI] [PubMed] [Google Scholar]
- Lee Mee Sook, Crittenden Kathleen S, Yu Elena. Social support and depression among elderly Korean immigrants in the United States. International Journal of Aging and Human Development. 1996;42(4):313–327. doi: 10.2190/2VHH-JLXY-EBVG-Y8JB. [DOI] [PubMed] [Google Scholar]
- Lewinsohn Peter M, Antonuccio DO, Steinmetz J, Teri Lin. The coping with depression course: A psychoeducational intervention for unipolar depression. Castalia Eugene, OR: 1984. [Google Scholar]
- Martire Lynn M, Schulz Richard. Involving Family in Psychosocial Interventions for Chronic Illness. current directions in psychological science. 2007;16(2):90–94. [Google Scholar]
- Massie Mary Jane. Prevalence of depression in patients with cancer. JNCI Monographs. 2004;2004(32):57–71. doi: 10.1093/jncimonographs/lgh014. [DOI] [PubMed] [Google Scholar]
- Milgrom Jeannette, Negri Lisa M, Gemmill Alan W, McNeil Margaret, Martin Paul R. A randomized controlled trial of psychological interventions for postnatal depression. British Journal of Clinical Psychology. 2005;44(4):529–542. doi: 10.1348/014466505X34200. [DOI] [PubMed] [Google Scholar]
- Mueller Timothy I, Leon Andrew C, Keller Martin B, Solomon David A, Endicott Jean, Coryell William, Maser Jack D. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. American Journal of Psychiatry. 1999;156(7):1000–1006. doi: 10.1176/ajp.156.7.1000. [DOI] [PubMed] [Google Scholar]
- Mulcahy Rhiannon, Reay RebeccaE, Wilkinson RossB, Owen Cathy. A randomised control trial for the effectiveness of group interpersonal psychotherapy for postnatal depression. Archives of Women's Mental Health. 2010;13(2):125–139. doi: 10.1007/s00737-009-0101-6. [DOI] [PubMed] [Google Scholar]
- Murray Christopher JL, Lopez Alan D. Measuring the global burden of disease. New England Journal of Medicine. 2013;369(5):448–457. doi: 10.1056/NEJMra1201534. [DOI] [PubMed] [Google Scholar]
- National Alliance for Caregiving/AARP. Caregiving in the US. Washington, DC: 2004. [Google Scholar]
- National Alliance for Caregiving/AARP. Caregiving in the US 2009. Washington, DC: 2009. [Google Scholar]
- Paykel ES, Scott J, Cornwall PL, Abbott R, Crane C, Pope M, Johnson AL. Duration of relapse prevention after cognitive therapy in residual depression: follow-up of controlled trial. Psychological Medicine. 2005;35(01):59–68. doi: 10.1017/S003329170400282X. [DOI] [PubMed] [Google Scholar]
- Rahman Atif, Malik Abid, Sikander Siham, Roberts Christopher, Creed Francis. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: a cluster-randomised controlled trial. The Lancet. 2008;372(9642):902–909. doi: 10.1016/S0140-6736(08)61400-2. http://dx.doi.org/10.1016/S0140-6736(08)61400-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renner Fritz, Cuijpers Pim, Huibers Marcus. The effect of psychotherapy for depression on improvement in social functioing: A meta-analysis. Psychological Medicine. 2014:1–14. doi: 10.1017/S0033291713003152. [DOI] [PubMed] [Google Scholar]
- Sandberg JG, Harper JM. In search of a marital distress model of depression in older marriages. Aging & Mental Health. 2000;4(3):210–222. [Google Scholar]
- Sandberg Jonathan G, Harper James M. DEPRESSION IN MATURE MARRIAGES: IMPACT AND IMPLICATIONS FOR MARITAL THERAPY. Journal of Marital and Family Therapy. 1999;25(3):393–406. doi: 10.1111/j.1752-0606.1999.tb00256.x. [DOI] [PubMed] [Google Scholar]
- Sandberg Jonathan G, Miller Richard B, Harper James M. A Qualitative Study of Marital Process and Depression in Older Couples. Family Relations. 2002;51(3):256–264. [Google Scholar]
- Seaburn David B, Lyness Jeffrey M, Eberly Shirley, King Deborah A. Depression, Perceived Family Criticism, and Functional Status Among Older, Primary-Care Patients. American Journal of Geriatric Psych. 2005;13(9):766–772. doi: 10.1176/appi.ajgp.13.9.766. [DOI] [PubMed] [Google Scholar]
- Simons AD, Murphy GE, Levine JL, Wetzel RD. Cognitive therapy and pharmacotherapy for depression: Sustained improvement over one year. Archives of General Psychiatry. 1986;43(1):43–48. doi: 10.1001/archpsyc.1986.01800010045006. [DOI] [PubMed] [Google Scholar]
- Smith Felicity, Francis Sally-Anne, Gray Nicola, Denham Michael, Graffy Jonathan. A multi-centre survey among informal carers who manage medication for older care recipients: problems experienced and development of services. Health & Social Care in the Community. 2003;11(2):138–145. doi: 10.1046/j.1365-2524.2003.00415.x. [DOI] [PubMed] [Google Scholar]
- Stansfeld Stephen, Marmot Michael. Deriving a survey measure of social support: the reliability and validity of the Close Persons Questionnaire. Social Science & Medicine. 1992;35(8):1027–1035. doi: 10.1016/0277-9536(92)90242-i. [DOI] [PubMed] [Google Scholar]
- Sterne Jonathan AC, Egger Matthias. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. Journal of Clinical Epidemiology. 2001;54(10):1046–1055. doi: 10.1016/s0895-4356(01)00377-8. [DOI] [PubMed] [Google Scholar]
- Talley Ronda C, Crews John E. Framing the Public Health of Caregiving. Am J Public Health. 2007;97(2):224–228. doi: 10.2105/ajph.2004.059337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voils Corrine I, Steffens David C, Flint Elizabeth P, Bosworth Hayden B. Social Support and Locus of Control as Predictors of Adherence to Antidepressant Medication in an Elderly Population. American Journal of Geriatric Psych. 2005;13(2):157–165. doi: 10.1176/appi.ajgp.13.2.157. [DOI] [PubMed] [Google Scholar]
- Wallace BC, Schmid CH, Lau J, Trikalinos TA. Meta-Analyst: software for meta-analysis of binary, continuous and diagnostic data. BMC Med Res Methodol. 2009;9(1):80. doi: 10.1186/1471-2288-9-80. [DOI] [PMC free article] [PubMed] [Google Scholar]