

Abstract
Agenesis of the right upper lobe of the lung is a very uncommon congenital anomaly and may be referred to chest clinics in adulthood for an incidental finding of abnormal chest radiograph. The presentations of chest radiograph may imitate many common situations such as right upper lobe collapse presenting as an ipsilateral shifting of the mediastinum or elevation of the right hemidiaphragm due to eventration or subdiaphragmatic lesions. A chest computed tomography is considered the most conclusive examination used to diagnose lung agenesis. Three-dimensional reconstructed images can be particularly helpful in delineating abnormalities of the bronchi and associated arterial and venous structures. We describe here a young woman with allergic rhinitis and bronchial asthma since her early childhood. She was referred to our clinic for an incidental finding of abnormal chest radiograph after a school health checkup. Right upper lobe atelectasis or intra-abdominal lesions were initially suspected. After a thorough image study, she was diagnosed as a case of agenesis of the right upper lobe. Our report emphasizes the importance that a high index of suspicion and adequate image investigation are necessary to diagnose congenital lung anomalies.
Keywords: Congenital anomaly, lobar agenesis
Introduction
Pulmonary agenesis is a very uncommon congenital abnormality that represents the unsuccessful growth of the primitive lung bud. The cause may be a primary embryogenic defect or secondary to situations that restrict fetal lung growth [1]. Pulmonary agenesis has been classified morphologically based on the extent to which bronchopulmonary tissue is absent. Spencer modified earlier classification and divided pulmonary agenesis into three categories: (1) bilateral complete agenesis; (2) unilateral agenesis; and (3) lobar agenesis or lesser forms of congenital anomaly. Almost half of pulmonary agenesis cases accompany congenital defects, which may involve multiple organ systems. The incidence rate is unknown, and there is no gender aptitude. Cases of isolated lobar agenesis have been uncommonly reported [2]. We describe here a young woman who was shown to have agenesis of the right upper lobe.
Case Report
An 18-year-old average-built girl was referred to our department for further evaluation of an abnormal chest radiograph. She has been diagnosed with allergic rhinitis and bronchial asthma since her early childhood. There was no history of orthopnea, palpitation, chest pain, or weight loss. Her perinatal history was insignificant. There was no other significant medical history. A physical examination showed that she had a well-developed stature without any abnormalities. The chest radiograph demonstrated a reduction of the right lung volume with ipsilateral shifting of the mediastinum and elevation of the right hemidiaphragm (Fig. 1). Right upper lobe atelectasis or intra-abdominal lesions were initially suspected.
Figure 1.
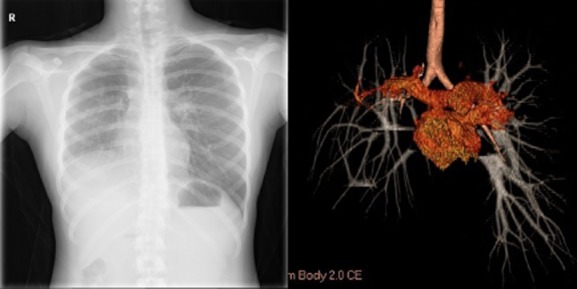
(Left panel) The chest radiograph shows a shift of the mediastinal structures to the right side with elevation of the right hemidiaphragm. (Right panel) Three-dimensional image reconstruction shows the right hyparterial bronchus and the absence of the right upper lobe bronchi.
A contrast-enhanced chest computed tomography (CT) demonstrated bilobed bilateral lungs with two hyparterial bronchi (i.e. bronchi that pass below the pulmonary arteries) and elevation of the right hemidiaphragm. The caliber of the right main pulmonary artery was relatively smaller than the left artery (Fig. 2). The three-dimensional image reconstruction disclosed the right hyparterial bronchus, and the right upper bronchus and pulmonary artery of the upper lobe were absent (Fig. 1). The abdominal ultrasonogram showed no significant anomaly in the liver, spleen, kidney, or other abdominal organs. A transthoracic echocardiogram revealed no evidence of structural abnormalities except the bicuspid aortic valve. Lung function tests disclosed normal pulmonary function. The measured findings were as follows: FVC 82%, FEV1 75%, FEV1/FVC 82%, and FEF25–75 56%. The images suggest the impression of right upper lobe agenesis with ipsilateral hyparterial bronchus. She was diagnosed as a case of agenesis of the right upper lobe.
Figure 2.

(Left panel) Coronal computed tomography scan of the chest shows the right hyparterial bronchus and the absence of the right upper lobe bronchi, volume loss with ipsilateral shift of the heart and mediastinal contents, and elevation of the right hemidiaphragm. (Right panel) The caliber of the right main pulmonary artery was relatively smaller.
Discussion
Lobar agenesis of the lung is a very rare anomaly that may be observed in isolation or may be accompanied with other congenital defects of the cardiovascular, musculoskeletal, or gastrointestinal systems [3]. Genetic defects of the pulmonary system and embryonic disorders of the bronchi contribute to anomaly, but the pathogenesis remains controversial. The rare agenesis–hypoplasia complex represents the failure of lung development at separate stages: agenesis (absence of both bronchus and lung parenchyma), aplasia (absence of lung parenchyma with bronchus present), and hypoplasia (both bronchus and rudimentary lung parenchyma present). Less than 5% of the general population develop bronchial anomalies, and the malformation of the right upper bronchus is the most common abnormality. Pulmonary artery hypoplasia is commonly accompanied with such an anomaly of the lung lobe [4]. An investigation of the associated vascular abnormalities is therefore necessary.
Isolated lobar agenesis is usually asymptomatic and may remain undiagnosed throughout childhood until a referral for an abnormal chest radiograph [5]. In right upper lobe agenesis of the lung, the presentations of a chest radiograph include a decreased right lung volume, shifting of the mediastinum on the right side, and an elevation of the right hemidiaphragm. The differential diagnosis of our patient's chest radiograph includes right upper lobe atelectasis, right hemidiaphragm paralysis, right hemidiaphragmatic eventration, pulmonary hypoplasia/agenesis, lobectomy, subpulmonic effusion, and intra-abdominal volume increase causing right hemidiaphragm elevation. A chest CT is considered to be the most conclusive examination to diagnose congenital abnormalities of the lung and the associated vascular anomalies when a chest radiograph is not diagnostic. Three-dimensional reconstruction can be particularly helpful in delineating abnormalities of the bronchi and associated arterial and venous structures. Angiography is reserved for patients requiring embolization or revascularization surgery. Treatment is necessary for recurrent chest infections. The prognosis is good if there is no other malformation.
Bilobed right lung includes one lobe agenesis of right lung and “bilateral” left lungs that commonly have associated cardiac defects and polysplenia (so-called heterotaxy syndrome). Our patient does not match the definition of heterotaxy syndrome except for the bilateral presence of two lobes. The absence of the right upper bronchus and pulmonary artery of the upper lobe was confirmed via chest CT and three-dimensional reconstruction, and no evidence of other organ anomalies was found. The patient was finally shown to have agenesis of the right upper lobe. To conclude, in a patient demonstrating an abnormal chest radiograph with or without respiratory symptoms, we should always consider a congenital anomaly of the lung. CT may be useful in determining the extent of the lesion and to define associated abnormalities.
Disclosure Statements
No conflict of interest declared.
Appropriate written informed consent was obtained for publication of this case report and accompanying images.
References
- Mardini MK. Nyhan WL. Agenesis of the lung: report of four patients with unusual anomalies. Chest. 1985;87:522–527. doi: 10.1378/chest.87.4.522. [DOI] [PubMed] [Google Scholar]
- Schwartz M. Ramachandran P. Congenital malformations of the lung and mediastinum – a quarter century of experience from a single institution. J. Pediatr. Surg. 1997;32:44–47. doi: 10.1016/s0022-3468(97)90090-7. [DOI] [PubMed] [Google Scholar]
- Clements BS. Congenital malformations of the lungs and airways. In: Landau LI, editor; Taussing LM, editor. Pediatric respiratory medicine. St. Louis, MO, USA: Mosby; 1999. pp. 1106–1136. [Google Scholar]
- Stovin PGI. Early lung development. Thorax. 1985;40:401–405. doi: 10.1136/thx.40.6.401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zack MS. Eber E. Adult outcome of congenital lower respiratory tract malformations. Thorax. 2001;56:65–72. doi: 10.1136/thorax.56.1.65. [DOI] [PMC free article] [PubMed] [Google Scholar]