

Abstract
Osteoarthritis is the most prevalent arthritic condition. Systemic inflammatory cytokines appear to have an important role in the onset and maintenance of the disease. Sleep disturbances are prevalent in osteoarthritis and associated with alterations in systemic inflammatory cytokines, suggesting a common pathophysiology across these conditions. A comparative investigation of the effects of insomnia disorder and osteoarthritis on pain-evoked cytokine responses has yet to be undertaken. We examined the influence of symptomatic knee osteoarthritis and insomnia disorder on resting C-reactive protein (CRP), interleukin (IL)-6, and IL-10 levels, and pain-evoked IL-6 and IL-10 responses. Participants were N = 117 older adults (mean age = 59.7 years; 61.8% women) rigorously evaluated for knee osteoarthritis and insomnia disorder using established diagnostic guidelines. Results revealed no association of osteoarthritis or insomnia disorder with CRP. Resting IL-6 was greater in osteoarthritis participants versus those without osteoarthritis, although this association was largely attributable to BMI. IL-10 was highest among participants with osteoarthritis or insomnia disorder. Growth curve modeling revealed that participants with insomnia disorder had greater pain-evoked IL-6 responses than participants without insomnia disorder or osteoarthritis. These findings highlight the utility of laboratory pain testing methods for understanding individual differences in inflammatory cytokines. Moreover, our findings provide evidence for amplified pain-evoked pro-inflammatory cytokine reactivity among older adults with clinically diagnosed insomnia disorder, even after controlling for individual differences in BMI and age. Additional research will be required determine whether an amplified pain-related cytokine response contributes to OA, and possibly other age-related disease, associated with insomnia disorder.
Keywords: osteoarthritis, insomnia disorder, sleep, inflammation, cytokines, pain, stress
1. Introduction
An estimated 27 million individuals in the United States have osteoarthritis (OA) (Neogi, 2013). Although local inflammatory cytokines are a critical pathophysiological component of OA (Wojdasiewicz, 2014), studies support an important role for systemic cytokines concerning incident OA (Livshits et al., 2009) and related joint and muscular pathology among older adults (Barker et al., 2014; Brinkley et al., 2009; Santos et al., 2011; Stannus et al., 2010; Stannus et al., 2013). As a result, it can be hypothesized that variables that influence systemic cytokines, perhaps particularly in the context of acute pain or injury, may enhance risk for OA and other age-related disease processes through elevations in systemic inflammatory cytokines. In the current study, we explored the possibility that a common pathophysiology of insomnia disorder and OA might be represented through associations of these factors with inflammatory markers both at rest and in the context of pain provocation.
The extant literature supports the hypothesis that insomnia and OA may be co-morbid and share reciprocal risk, at least in part, through systemic inflammation. First, sleep problems are evident in OA samples (Abad et al., 2008). OA patients report difficulties with sleep continuity (Wilcox et al., 2000), and these sleep problems have been correlated with greater joint pain, pain-related inference, and depressive symptoms (Leigh et al., 1987; Wilcox et al., 2000). Sleep problems have also been associated with greater pain report in OA samples, in addition to manifold other chronic pain conditions (Edwards et al., 2009a; Haack et al., 2012; Quartana et al., 2010; Smith et al., 2009; Tang et al., 2012; Vitiello et al., 2014). Second, pain-evoked pro-inflammatory cytokine response has been shown to be exaggerated in OA versus pain-free control participants (Lee et al., 2011), and resting levels of the pro-inflammatory cytokine, interleukin (IL)-6 has been linked to prevalent and 5-year incident OA (Livshits et al., 2009). Other inflammatory cytokine markers have been prospectively linked to worsening OA, joint space narrowing, muscular pathology, and poorer physical function (Barker et al., 2014; Brinkley et al., 2009; Santos et al., 2011; Stannus et al., 2010; Stannus et al., 2013). Third, greater non-painful stress-evoked inflammatory cytokine response has been associated with self-reported sleep problems (Heffner et al., 2012; Prather et al., 2013). Finally, there is emerging empirical data supporting the notion that treating insomnia disorder can effectively mitigate pain and functional impairment through early-treatment reductions of sleep problems in OA patients (Vitiello et al., 2014). Moreover, pre-surgical sleep problems are diminished following total hip replacement surgery (Fielden et al., 2003). These data further highlight the possibility that OA and insomnia disorder possess a shared pathophysiology; the extant literature suggests systemic inflammatory markers as a viable candidate.
Systemic levels of C-reactive protein (CRP) and pro-inflammatory cytokines, such as interleukin-6 (IL-6), have been linked to prevalent and incident OA, progression of structural abnormalities, and pain and functional impairment among individuals with and without OA (Barker et al., 2014; Cesari et al., 2004; Livshits et al., 2009; Santos et al., 2011; Stannus et al., 2010; Stannus et al., 2013). These inflammatory biomarkers are also sensitive to stress (Steptoe et al., 2007), sleep disturbance (Faraut et al., 2012) and pain (Edwards et al., 2009a). Systemic inflammation appears to be evident in the context of insomnia disorder as well (Burgos et al., 2006; Vgontzas et al., 2002). Preliminary studies have found interactions between non-painful stress and sleep problems on the pro-inflammatory cytokine, IL-6 (Heffner et al., 2012; Prather et al., 2013). Experimental sleep deprivation increases circulating IL-6 levels and spontaneous pain in healthy participants (Haack et al., 2007), though some studies have shown no effect of total sleep deprivation on resting pro-inflammatory cytokine levels (Matzner et al., 2013; Ruiz et al., 2012). To our knowledge, whether pain-evoked inflammatory cytokines are elevated by the presence of insomnia disorder among individuals with or without OA has not been systematically explored. This is important because pain is the most clinically significant symptom of OA, and many individuals who develop OA have a history of physical trauma (i.e., post-traumatic osteoarthritis; (Schenker et al., 2014). Lastly, no human studies have considered anti-inflammatory cytokine responses to pain. IL-10 is an immunoregulatory, anti-inflammatory cytokine that is believed to have an important role in the modulation of OA pathology (Wojdasiewicz et al., 2014) and sleep-wake regulation (Opp, 2005). Knowing whether OA and insomnia disorder interact with pain to promote differential activity of anti-inflammatory cytokines, such as IL-10, can broaden our understanding of immunoregulatory mechanisms underlying these constructs.
If systemic inflammatory markers emerge as a common pathophysiologic element of OA and insomnia disorder, then we would anticipate additive (i.e., main) effects of these conditions on pain-evoked cytokine response. There are potentially important implications if data support this hypothesis. First, if insomnia disorder is related to greater pain-evoked inflammatory cytokine response compared to good sleepers, then we can tentatively advance the argument that insomnia disorder might enhance risk for the onset (e.g., following acute injury or owing to age-related processes), maintenance, or exacerbation of OA, in part, through common inflammatory mechanisms. It is also stands to reason that if OA is associated with greater pain-evoked inflammatory cytokine response versus pain-free controls, it might represent a risk variable for the onset, maintenance, and exacerbation of insomnia disorder symptoms. A first and important precondition of this line of reasoning, and the goal of the present study, was to determine whether OA and insomnia disorder are associated with exaggerated resting and pain-evoked markers of inflammation relative to appropriate controls. We examined resting CRP, IL-6, and IL-10, as well as pain-evoked IL-6 and IL-10, among participants carefully screened for a diagnosis of symptomatic KOA and/or insomnia disorder. Control groups were participants without evidence of symptomatic KOA and those who met criteria as normal sleepers based on clinical evaluation (Edinger et al., 2004). Based on prior studies (Edwards et al., 2008; Edwards et al., 2009b; Lee et al., 2011), we hypothesized that we would observe pain-evoked increases in IL-6 irrespective of diagnosis. We further hypothesized that the presence of a KOA or insomnia disorder diagnosis would be associated with greater resting levels of CRP and IL-6, and that pain-evoked IL-6 and IL-10 responses would be greater among participants with KOA or insomnia disorder versus those without KOA or normal sleepers.
2. Methods
2.1 Participants
The data for the current study were part of a larger study designed to examine the effects of insomnia and osteoarthritis on laboratory measure pain sensitivity and the efficacy of cognitive behavioral therapy for insomnia disorder among symptomatic KOA patients. The data presented here are from the baseline assessment alone. Intervention data will be presented elsewhere. Participants (N = 117) were recruited via advertisements in community media outlets and physician offices for individuals with and without knee pain and/or individuals with or without trouble sleeping. General and study group-specific inclusion/exclusion criteria are presented in Table 1. Sixty-three participants received a diagnosis of KOA and insomnia disorder (KOA+Insomnia)1, n = 17 met criteria for KOA without insomnia disorder (KOA+ Normal Sleeper), n = 17 met criteria for Insomnia Disorder without KOA (No KOA + Insomnia Disorder), and n = 20 did not meet criteria for either KOA or Insomnia Disorder (No KOA + Normal Sleeper). Demographic, pain, sleep and mood characteristics of these participant groups are provided in Table 2. All participants included in the study provided informed consent in accordance with the Johns Hopkins University Institutional Review Board requirements.
Table 1.
General and Study Group-Specific Study Inclusion and Exclusion Criteria
| General Exclusion Criteria |
|
| Study Group-Specific Inclusion Criteria |
| Knee Osteoarthritis (KOA) |
|
| Insomnia Disorder |
|
| Normal Sleeper |
|
Participants infrequently taking opioids or sedative hypnotics were not excluded from participation in the study, but were required to agree to discontinue use of opioids and/or sedatives for one week prior to the laboratory pain testing session. Individuals using antidepressants were not excluded from participation in the larger study, but were excluded from the present analysis due to potential confounding associated with cytokines.
History, physical examination, and diagnosis were carried out by a board certified rheumatologist.
n = 10 (12.5%) participants with KOA were under 50 years of age (M = 45.8; range: 41–49) in the current study sample.
Table 2.
Participant demographics, medication use, BMI, sleep characteristics, pain testing responses, clinical pain, and self-reported depressive symptoms by study group. Mean (SD) values are reported unless stated otherwise.
| No KOA + No Insomnia (n=20) | KOA + No Insomnia (n=17) | No KOA + Insomnia (n = 17) | KOA + Insomnia (n=63) | p-value | |
|---|---|---|---|---|---|
|
Demographics
|
|||||
| Gender (% female) | 55.0% | 52.9% | 64.7% | 74.6% | ns |
| Age (years) | 57.3 (6.4) | 65.4 (11.0) | 57.2 (7.4) | 59.7 (10.3) | .005a |
| Ethnicity (% Caucasian) | 65.0% | 76.5% | 47.1% | 57.1% | ns |
|
|
|||||
|
Medication Use (% yes)
|
|||||
| NSAID | 10% | 76.4% | 23.5% | 74.6% | <.001a |
| Anti-hypertensives | 15% | 23.5% | 35.3% | 38.1% | ns |
|
|
|||||
|
Anthropometric Measures
|
|||||
| BMI (kg/m2) | 26.1 (4.7) | 28.6 (5.1) | 27.02 (5.6) | 31.2 (6.1) | .008a |
|
|
|||||
|
Sleep Characteristics
|
|||||
| ISI | 1.3 (1.4) | 1.8 (2.7) | 17.8 (5.2) | 16.9 (4.6) | <.001b |
| PSQI | 2.5 (1.7) | 2.7 (1.6) | 11.8 (3.4) | 10.8 (3.0) | <.001b |
| ESS | 3.8 (3.1) | 5.7 (4.4) | 6.9 (6.2) | 9.6 (4.7) | .03a <.001b |
|
|
|||||
|
Quantitative Sensory Testing Responses
|
|||||
| PPTh - Trapezius | 372.1 (153.5) | 376.3 (82.91) | 448.0 (161.7) | 385.4 (167.5) | ns |
| PPTh - Quadriceps | 572.3 (212.4) | 502.2 (145.5) | 736.7 (210.9) | 543.7 (245.0) | .009a .04b |
| Mechanical Pain Rating (0–100) | 40.1 (27.5) | 51.3 (25.3) | 50.0 (32.4) | 50.1 (29.9) | ns |
| HPTh | 42.6 (3.0) | 43.0 (3.6) | 42.7 (3.5) | 42.5 (3.2) | ns |
| Heat Pain Ratings (0–100) | 58.2 (23.8) | 63.9 (15.8) | 74.1 (22.3) | 69.4 (24.4) | ns |
| Cold Pain Ratings (0–100) | 75.7 (31.9) | 83.9 (16.4) | 86.9 (16.4) | 85.5 (14.5) | ns |
|
|
|||||
|
Clinical Pain
|
|||||
| WOMAC | |||||
| Pain | 0.09 (0.18) | 3.17 (1.58) | 0.16 (0.16) | 4.41 (2.28) | <.001a |
| Joint Stiffness | 0.11 (0.25) | 3.84 (3.39) | 0.34 (0.48) | 5.22 (2.74) | <.001a |
| Physical Function | 0.07 (0.12) | 3.19 (1.85) | 0.17 (0.16) | 4.60 (2.24) | <.001a |
| Kellgren-Lawrence Scale (% yes) | |||||
| Grade 1 | - | 28.6% | - | 34.6% | ns |
| Grade 2 | - | 7.1% | - | 11.5% | ns |
| Grade 3 | - | 21.4% | - | 30.8% | ns |
| Grade 4 | - | 42.9% | - | 23.1% | ns |
|
|
|||||
|
Negative Affect
|
|||||
| CES-D | 2.6 (3.2) | 2.5 (2.6) | 11.2 (7.4) | 13.4 (7.1) | .04b |
Notes. NSAID = Non-steroidal Anti-Inflammatory Drug; BMI = Body Mass Index; ISI = Insomnia Severity Index; PSQI = Pittsburgh Sleep Quality Index; ESS = Epworth Sleepiness Scale; PPTh = Pressure Pain Threshold; HPTh = Heat Pain Threshold; WOMAC = the Western Ontario and McMasters Universities Arthritis Index; CES-D = Center for Epidemiological Studies – Depression Scale; ns = not significant (p > .05)
KOA main effect
Insomnia main effect
2.2. Procedures
Eligible participants arrived at the laboratory visit during which they completed a standardized laboratory pain testing protocol with accompanying blood draws (see Figure 1). Sessions were conducted between 14:00 and 16:00 to control for circadian variation in cytokine levels (Vgontzas et al., 2005). At the beginning of the session, and 30 minutes prior to pain testing, an I.V. line was placed in the antecubital vein and a 0.45% saline solution was infused to maintain catheter patency. Blood samples (10 ml) were drawn 5 times throughout the baseline assessment, twice during rest and prior the onset of the pain testing procedures, and 3 times following the pain testing procedures (immediately and 30 and 60 minutes following). All samples were collected with EDTA vacutainers, placed on ice and centrifuged at 4°Celsius within 30 minutes following all blood draws. Plasma was aliquoted and stored at −80°C until batch assayed.
Figure 1.
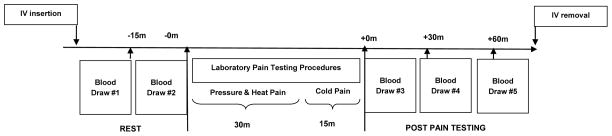
Protocol schematic for pain testing and timing of blood draws.
The pain testing procedures included a battery of standardized mechanical and thermal psychophysical pain tests that have been shown in previous work to evoke a pro-inflammatory cytokine response in healthy (Edwards et al., 2008) and OA participant samples (Lee et al., 2011). The battery lasted approximately 45 minutes. A detailed description of the pain testing procedures used in the current study is presented in Finan et al. (Finan et al., 2013). In summary, assessments of pressure pain thresholds (PPTh) were determined twice at the trapezius and quadriceps using standard digital pressure algometry. Mechanical pain testing involved the assessment of pain ratings (0 “no pain” to 100 “worst pain imaginable”) in response to an initial stimulus, and then following a sequence of 10 stimuli of identically weighted punctate noxious probes (Rolke et al., 2006) applied to the middle finger (non-dominant) and patella. Additional tests included an assessment of thermal Pain Threshold (TPTh), as well as suprathreshold heat and cold pain ratings (0 “no pain” to 100 “worst pain imaginable”) derived from heat delivered to the skin using a peltier-element-based stimulator (Medoc Thermal Sensory Analyzer) with a 9 centimeter2 thermode (TSA-II, Ramat Yishai, Israel) and a repeated hand immersions in a standard cold pressor maintained at 4° Celsius, respectively.
2.3. Measures
2.3.1. Self-Reported Sleep Characteristics
Participant sleep characteristics were assessed using well-validated self-report measures of insomnia symptoms, global sleep quality, and daytime sleepiness. Insomnia severity was assessed using the Insomnia Severity Index (ISI) (Bastien et al., 2001). The ISI is a brief screening measure of insomnia consisting of 7 items scored on a five-point Likert scale. Items were rated retrospectively for the preceding 1-week period. Internal consistency is good and it has demonstrated convergent validity with formal diagnostic criteria (Morin et al., 2011). Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI) (Buysse et al., 1989). The PSQI is a widely used and reliable measure of overall sleep quality. A higher PSQI global score is indicative of poorer sleep quality. Sleepiness was assessed with the Epworth Sleepiness Scale (ESS), a widely used 8-item measure assessing daytime sleepiness (Johns, 1991). A higher score indicates greater sleepiness. All participants maintained a daily sleep diary and had wrist actigraphy for a 2-week period prior to the baseline assessment. A full diagnostic polysomography (PSG) was conducted according to standardized procedures for in-home ambulatory recordings (Redline et al., 2007). Group differences in diary, actigraphy, and PSG data will be presented elsewhere.
2.3.2. Clinical Pain Assessment
Clinical pain was assessed using the Western Ontario and McMasters Universities Arthritis Index (WOMAC, 3.1; (Altman et al., 1996; Bellamy, 1989; Bellamy et al., 1988). The WOMAC is comprised of 24 items and is a well-validated, widely used retrospective outcomes measure that yields three indices specific to knee osteoarthritis: 1) pain severity, 2) disability and 3) joint stiffness. Patient ratings are made on a 10 centimeter visual analogue scale.
2.3.3. Depressive Symptoms
Depressive symptoms were assessed using the Center for Epidemiological Studies Depression (CES-D) scale (Radloff, 1977). The CES-D is a 20-item self-report measure that assesses the frequency of depression symptoms over the past week on a 0–3 Likert-type scale (“Rarely or none of the time” to “Most or all of the time”). Possible scores in the current study ranged from 0 to 27 (see general exclusion criteria above).
2.3.4. Body Mass Index (BMI)
Body weight and height were obtained from participant self-report. BMI was calculated as weight in kilograms (kg) divided by height in meters (m) squared (kg/m2).
2.3.5. Inflammatory Markers
Plasma levels of CRP, IL-6 and IL-10 were quantified in duplicate according to the steps outlined in the respective commercial enzyme immunoassay kits from R&D Systems (Minneapolis, MN). Plasma CRP levels were quantified from the first resting blood draw before pain testing began, and plasma IL-6 and 10 levels were quantified from all pre- and post-pain testing time points. Plasma for CRP was diluted such that the ceiling value was 10,050 ng/mL.
2.4. Data Analysis
All analyses were performed using IBM Software, SPSS Version 21. Preliminary analyses examined group differences in demographics, medication use, BMI, sleep characteristics, pain response, clinical pain, and depression symptoms. Group differences in categorical variables were examined using χ2 analyses. Group differences in continuous variables were examined using 2 KOA (No KOA, KOA) × 2 Insomnia (Normal Sleeper, Insomnia Disorder) analysis of variance (ANOVA). CRP, IL-6 and IL-10 values were log-transformed to normalize their distributions.
Two KOA (No KOA, KOA) × 2 Insomnia (Normal Sleeper, Insomnia Disorder) linear mixed effects analysis was used to examine between-groups differences in CRP, as well as resting (pre-pain testing) levels of IL-6 and IL-10. We utilized growth curve modeling (Singer and Willet, 2003) to model individual changes in pain-evoked IL-6 and IL-10 responses, as well as effects of KOA and Insomnia Disorder on the rate of change (i.e., growth). We first tested an unconditional growth model that examined individual variation in growth rates, which provides an estimate of individual rate of change from before to following the pain testing stress procedures. For this model, we allowed individual intercepts and slopes to vary at random. A significant βtime coefficient would provide evidence for significant changes from baseline across the pain testing procedures. Lastly, we examined whether variability in the rate of change was accounted for by group membership, hence we added KOA (No KOA, KOA) and Insomnia (Normal Sleeper, Insomnia Disorder) factors as Level-2 variables. A significant βtime x group coefficient would provide evidence that group membership accounts for inter-individual variation in the rate of change of cytokine concentrations in the context of the pain testing procedures. All models were fitted using maximum likelihood estimates and utilized an unstructured variance-covariance matrix for random effects.
For all analyses, threshold for statistical significance was set at p < .05 (two-tailed). For all dependent variables, we report unadjusted results, and where significant main or interaction effects emerged, adjusted results are also presented. This allowed us to make preliminary statements concerning possible mediation. We found that BMI and age were significant covariates, whereas participant sex, NSAID use, and CES-D scores did not emerge as statistically significant covariates, nor did they improve model fit. It should also be noted that opioid use was not associated with any of the inflammatory markers under study.
3. Results
3.1. Preliminary Analyses
Descriptive statistics by group membership are provided in Table 2. KOA participants were older, reported using NSAIDs more frequently and had greater BMI values than No KOA participants (all p-values ≤ .05). Based on WOMAC subscale scores, KOA participants had greater clinical pain, joint stiffness and pain-related interference than No KOA participants. KOA participants had lower PPTh values than No KOA participants when assessed at the quadriceps (p = .009). KOA participants had greater ESS scores than No KOA participants (p = .03). Insomnia Disorder participants had lower PPTh assessed at the quadriceps than Normal Sleeper participants (p = .04). No other statistically significant group effects were evident for pain outcomes. Insomnia Disorder participants reported greater insomnia severity, poorer quality sleep, and greater sleepiness than Normal Sleeper participants (all p-values ≤ .001). Insomnia Disorder participants reported more depressive symptoms than Normal Sleeper participants (p = .04). No clinical pain or experimental pain values were associated with resting Log CRP or resting or pain-evoked Log IL-6 or Log IL-10 values (p-values ≥ .20). Hence, individual differences in clinical or experimental pain did not account for group effects on inflammatory markers. All other main effects and interactions (KOA X Insomnia) were not statistically significant (ps > .05).
3.2. Group Differences in resting plasma CRP, IL-6, and IL-10 levels
Results from the unadjusted 2 KOA (No KOA, KOA) × 2 Insomnia (Normal Sleeper, Insomnia Disorder) linear mixed effects model did not reveal statistically significant KOA, Insomnia, or KOA x Insomnia effects on CRP levels (p-values ≥ .15).
KOA participants had greater resting IL-6 levels than No KOA participants (β = .36, SE = .17, p = .04). The KOA main effect was no longer statistically significant in BMI- and age-adjusted models (β = .02, SE = .14, p = .39). Higher BMI (β = .06, SE = .01, p < .001) and older age (β = .01, SE = .004, p = .013) were associated with greater IL-6 levels. There was no evidence for an Insomnia (p = .57) or KOA x Insomnia effect (p = .81) on resting IL-6 levels. These findings suggest that BMI, to a large extent, and age, accounted for individual differences in resting IL-6 levels between the KOA and No KOA participants.
In unadjusted models, KOA participants had greater resting IL-10 levels than No KOA participants (β = .63, SE = .24, p = .011). Insomnia Disorder participants also had greater resting IL-10 levels than Norman Sleeper participants (β = .57, SE = .24, p = .021). The KOA x Insomnia effect was not statistically significant (p = .13). In the BMI- and age-adjusted model, the KOA and Insomnia main effects remained significant. To summarize, participants with KOA and/or Insomnia Disorder had greater resting plasma IL-10 levels than participants without KOA and classified as normal sleepers.
3.3. Group Differences in Pain-Evoked IL-6 and IL-10 Response
The unconditional growth model for IL-6 levels was examined to determine whether there was inter-individual variability in the rate of change across the pain testing procedures. The results of this model revealed that the pain testing procedures resulted in statistically significant increases in IL-6 levels (see Table 3). The random error terms were both significant at p < .001, suggesting that the rate of change randomly varied between subjects. There was a statistically significant association between the intercept and random growth indicator (β = −.02, SE = .006, p = .001), suggesting that participants with higher baseline IL-6 levels had a slower rate of change (increase) across the pain testing protocol than those who had lower baseline IL-6 values. To sum, these findings provide evidence for significant inter-individual variability in the rate of pain-evoked IL-6 change.
Table 3.
Unadjusted raw plasma cytokine mean (SD) levels (pg/ml) by assessment time pre- (resting) and post-pain testing procedures.
| −15 min Pain Testing | − 0 min Pain Pesting | + 0 min Pain Testing | +30 min Pain Testing | +60 min Pain Testing | p-value (two-tailed)a | |
|---|---|---|---|---|---|---|
| IL-6 | 4.61 (9.90) | 4.53 (8.71) | 4.94 (8.27) | 5.78 (7.22) | 5.94 (5.64) | P < .001 |
| IL-10 | 7.13 (8.38) | 7.04 (8.70) | 6.85 (9.33) | 6.61 (9.57) | 6.20 (9.04) | P < .001 |
Notes. Values presented are for all participants collapsed over Study Group
p-values were derived from unconditional growth models. For Log IL-6, the point estimate was .09 with a standard error of .02, yielding a t-statistic of 8.73. For Log IL-10 values, the point estimate was −0.05 with a standard error of .01, yielding a t-statistic of −4.39.
Figure 2, Panel A, shows rate of change for unadjusted IL-6 levels by KOA and Insomnia groups. There was a trend evident for the KOA main effect (β = .32, SE = .18, p = .07), such that KOA participants had greater overall IL-6 levels throughout the pain testing procedures. Insomnia and KOA x Insomnia effects were not statistically significant (p-values ≥ .61). Moreover, KOA, Insomnia and the KOA x Insomnia effects did not moderate the growth rate for IL-6 levels attributable to the pain testing protocol (p-values ≥ .15). In BMI- and age- adjusted models for IL-6 (values presented in Figure 2, Panel B), we observed statistically significant effects of BMI (β = .056, SE = .006, p < .001) and Age (β = .009, SE = .004, p = .016), such that higher BMI and older age were associated with greater IL-6 levels throughout the pain testing procedures. Covariation of BMI and age attenuated the trend for differences between KOA and No KOA participants in IL-6 levels (β = .10, SE = .14, p = .50).
Figure 2.

Unadjusted (Panel A) and BMI- and Age-adjusted (Panel B) Log interleukin (IL)-6 mean (SE) values by assessment time pre- (resting) and post- post-pain testing procedures by study group.
Notes. Resting (pre-pain testing) levels of IL-6 were significantly greater among KOA participants versus No KOA participants in unadjusted models, and KOA participants had greater pain-evoked IL-6 responses than No KOA participants (Panel A). In BMI- and age-adjusted models (Panel B), there were no statistically significant differences in resting IL-6 levels or pain-evoked IL-6 responses between KOA and No KOA participants. Participants with Insomnia Disorder + No KOA had significantly greater pain-evoked IL-6 increases than Normal Sleeper + No KOA participants in unadjusted (Panel A) and adjusted models (Panel B).
We considered the possibility that our ability to detect insomnia-related pain-evoked growth in IL-6 was diminished by the confounding of the insomnia and normal sleep group with the presence of KOA. Supporting this approach was a significant negative association between intercept and growth estimates, which remained evident in both unadjusted (β = −.016, SE = .006, p = .004) and BMI- and age-adjusted (β = −.009, SE = .004, p = .04) conditional growth models with IL-6 as the dependent variable. To directly isolate a potential effect of Insomnia Disorder on pain-evoked IL-6, we performed a comparison between No KOA + Insomnia and No KOA + Normal Sleeper participants on the growth rate of IL-6 in the post-pain testing period. The comparison revealed that the No KOA + Insomnia participants showed greater growth (increase) in IL-6 levels post-pain testing than the No KOA + Normal Sleeper participants (β = .12, SE = .04, p = .002), controlling for BMI and age. An additional comparison of KOA + Insomnia participants versus No KOA + Normal Sleeper on post-pain testing rate of IL-6 growth (increase) was not statistically significant (p = .83), supporting our contention that higher plasma levels of IL-6 across all measurements for KOA participants likely obscured the true effect of insomnia disorder on pain-evoked increases in IL-6 levels.
With IL-10 as the dependent variable, we first examined an unconditional growth model to determine whether there was inter-individual variability in the rate of change in this outcome across the pain testing procedures. The results of this model revealed that pain testing resulted in statistically significant decreases in IL-10 levels (see Table 3). The random error term was significant at p < .001, suggesting that variability in the rate of change can be attributable to individual differences. The intercept-slope correlation was not statistically significant (β = −.017, SE = .01, p = .11), but a similar pattern to that reported for IL-6 was evident, such that higher initial levels of IL-10 were associated with a slower rate of pain-evoked change. These findings support the existence of significant inter-individual variability in the rate of change for IL-10 levels across the pain testing procedures.
We subsequently examined whether KOA and Insomnia accounted for variability in the rate of change in IL-10 levels during and after the pain testing protocol. Figure 3 shows rate of change for unadjusted IL-10 levels by study group. Results from unadjusted models revealed that, irrespective of rate of change, KOA participants had greater overall levels of IL-10 than No KOA participants (β = .71, SE = .23, p = .003). Insomnia participants also had greater overall levels of IL-10 than Normal Sleeper participants (β = .64, SE = .23, p = .008). The KOA x Insomnia effect was not statistically significant, and there was no evidence that KOA and Insomnia accounted for variance in the rate of change (p-values ≥ .13).
Figure 3.

Unadjusted Log interleukin (IL)-10 mean (SE) values by assessment time pre- (resting) and post-pain testing procedures by study group.
Notes. KOA participants had greater significantly resting (pre pain-testing) and overall IL-10 levels than No KOA participants. Insomnia Disorder participants had significantly greater resting and overall levels of IL-10 levels than Normal Sleepers. The group effects on resting and overall IL-10 remained statistically significant even in BMI- and age-adjusted models. There were no statistically significant effects of KOA or Insomnia on pain-evoked IL-10 response.
In BMI- and age-adjusted models, main effects of KOA (β = .742, SE = .232, p = .002) and Insomnia (β = .617, SE = .223, p = .007) were still evident. The KOA x Insomnia interaction was also statistically significant (β = −.61, SE = .30, p = .04). Simple effects analyses examining associations between KOA and overall IL-10 levels revealed that KOA + Normal Sleeper participants had greater IL-10 levels across the entire stress protocol compared No KOA + Normal Sleeper participants (β = .739, SE = .184, p < .001), whereas KOA + Insomnia participants did not (p = .57). However, the rate of change in plasma IL-10 level was not conditional upon KOA or Insomnia (p-values ≥ .11). In summary, there was little evidence that KOA or Insomnia were related to pain-evoked changes in IL-10. However, participants with a diagnosis of KOA, Insomnia, or KOA + Insomnia had significantly greater plasma IL-10 levels throughout the stress protocol than No KOA + Normal Sleeper participants, even adjusting for BMI and age as potential confounders.
4. Discussion
We examined the effects of insomnia disorder and KOA on resting CRP and resting and pain-evoked systemic IL-6 and IL-10. The key findings were: (a) pain testing elicited a significant increase in IL-6 and a decrease in IL-10; (b) the association of KOA with greater overall IL-6 levels was attributable to individual differences in BMI and age; (c) in the absence of a KOA diagnosis, participants with insomnia disorder showed more robust pain-evoked IL-6 responses than participants without KOA or those classified as normal sleepers, independent of individual differences in BMI and age; and (d) IL-10 levels were higher among participants with a diagnosis of KOA or insomnia disorder, compared to participants without KOA and classified as normal sleepers.
Overall, the results did not provide support for the hypothesis that OA and insomnia disorder share exaggerated resting or pain-evoked inflammatory cytokine activity in common; the association between KOA and IL-6 levels (irrespective of insomnia disorder) was attributable to BMI and age. However, the hypothesis that insomnia disorder may be related to risk for incident OA is supported to some degree by the finding that pain-provocation resulted in an exaggerated and protracted IL-6 response in older adults with insomnia disorder compared to normal sleepers in the absence of a concurrent KOA diagnosis, even after controlling for BMI and age. The clinical significance of the insomnia disorder effect on the pain-evoked IL-6 response requires additional study.
IL-6 levels among No KOA + Insomnia Disorder participants had reached levels observed for participants with KOA approximately 60 minutes post-pain testing. These findings suggest that insomnia disorder is associated with exaggerated IL-6 sensitivity to pain, and if considered in the context of the broader literature concerning insomnia disorder, pain, inflammation, and OA, they highlight the possibility that insomnia may interact with pain- or stress-related events to enhance disease risk via activation of inflammatory cytokines. While other research has underscored exaggerated IL-6 responses to non-painful psychosocial stressors among self-reported poor sleepers (Heffner et al., 2012), there has been no prior report of an exaggerated pain-evoked cytokine response among participants meeting rigorous clinical diagnostic criteria for insomnia disorder. This is important because it eliminates the potential confounding effect of other sleep disorders, such as sleep apnea. Hence, these findings point to exaggerated pain-related pro-inflammatory cytokine sensitivity to acutely stressful events as a potentially relevant biomarker for age- and stress-related disease risk or progression that is widely believed to be associated with insomnia disorder (Luyster et al., 2012). The clinical relevance of the changes in IL-6 associated with laboratory pain testing remains unknown. Whether pain-evoked inflammatory response mediates an association between insomnia disorder and health-related outcomes among older adults awaits additional study.
These data replicate studies that highlighted sensitivity of IL-6 to laboratory pain testing (Edwards et al., 2008; Edwards et al., 2009b; Lee et al., 2011). To our knowledge, the effect of pain testing on IL-10 has not been previously reported. Although not a chief focus of the study, we found significant variability in the rate of change of both IL-6 and IL-10, suggesting that standardized pain testing methods might have utility for broadening our understanding of individual differences in pro- and anti-inflammatory cytokines related to sleep, pain, and OA.
The lack of an association between KOA and CRP is consistent with some (Engstrom et al., 2009; Livshits et al., 2009) and inconsistent with other studies (Lee et al., 2011). KOA also did not account for variability in pain-evoked IL-6 response. However, in unadjusted analyses, KOA was correlated with greater overall IL-6 levels. These findings dovetail with those of Lee et al. (2011). Whether we might have observed group differences in local cytokine response to pain (e.g., in joint fluid at the affected knee) should be examined in subsequent research. Nonetheless, systemic inflammatory cytokines, including IL-6, have been prospectively linked to worsening knee pain (Stannus et al., 2013), cartilage loss (Stannus et al., 2010), and incident OA (Livshits et al., 2009). Future studies should continue to examine factors associated with resting and pain- and stress-evoked cytokine activity, such as insomnia disorder, as these factors can be therapeutic targets among older adults that may mitigate risk for incident age- and stress-related disease, perhaps OA among them.
The conclusion that KOA was directly associated with greater IL-6 levels must be tempered. The KOA effect on IL-6 was not statistically significant after adjusting for BMI and age, with BMI emerging as the largest predictor of overall IL-6 levels. These findings suggest that KOA may be, in part, associated with greater IL-6 levels indirectly through elevated BMI. These findings are consistent with some prior studies of OA patients versus controls (Engstrom et al., 2009). However, findings from the Chingford Study identified BMI and circulating IL-6 as independent risk factors for incident OA (Livshits et al., 2009), and other studies have highlighted systemic markers of inflammation as important prospective correlates of OA-related processes among older adults, even after controlling for BMI and other confounders (Santos et al., 2011; Stannus et al., 2010; Stannus et al., 2013). These latter findings suggest that it is unlikely that BMI is the sole culprit that links OA to elevations in pro-inflammatory cytokine levels.
The role of BMI or visceral adiposity in accounting for elevations in markers of inflammation related to OA and insomnia disorder should not be underestimated. OA patients and individuals with poorer sleep are more likely to be overweight than their healthy counterparts (Carman et al., 1994; Coughlin and Smith, 2014; Engstrom et al., 2009; Livshits et al., 2009; Marshall et al., 2008), and recent data suggest that visceral adiposity may interact with stressful events and sleep problems to promote exaggerated pro-inflammatory cytokine activity (Brydon, 2011; Prather et al., 2013). Although the mechanism by which being overweight is related to prevalent and incident OA and insomnia disorder is not well-understood, it is plausible to hypothesize a role for inflammatory cytokines. Adipose tissue contributes substantially to systemic inflammation (Das, 2001) and up to one-third of inflammatory mediators originate from adipose tissue (Mohamed-Ali et al., 1997). Future studies will be required to more systematically examine the manner in which the inflammation-pain-sleep interface is affected by various indicators of body composition.
Participants with KOA or insomnia disorder had greater resting and overall IL-10 levels than participants without KOA and normal sleep. These findings provide some support for two extant lines of research. First, IL-10 has chondroprotective effects via antagonistic actions on pro-inflammatory mediators (Wojdasiewicz et al., 2014), and the magnitude of LPS stimulated IL-10 production in OA patients is negatively associated with OA risk (Riyazi et al., 2005). Second, animal studies suggest a sleep-interfering role for IL-10, possibly via antagonism of somnogenic pro-inflammatory cytokine activity (Fiorentino et al., 1991). Concerning stress responses, a recent study failed to detect stress-related IL-10 reactivity to an acute psychosocial stressor among healthy postmenopausal women, irrespective of sleep quality (Prather et al., 2013). IL-6 stimulates the production of IL-10, which then mitigates further pro-inflammatory activity (Daftarian et al., 1996). It is plausible that in the context of OA and insomnia disorder, there is production of IL-10 that regulates systemic levels of inflammation and also interferes with sleep quality and depth. In fact, our finding of greater pain-evoked IL-6 among insomnia disorder participants without KOA versus normal sleepers controls, coupled with the lack of differences in pain-evoked IL-6 responses between participants with versus without with KOA, lends some general support for this possibility. The findings concerning greater IL-10 levels in KOA and insomnia disorder participants require replication.
A key limitation of the current study concerns the small within-group sample sizes. Sample sizes were determined to have sufficient statistical power to detect main effects of insomnia disorder and OA on resting and pain-evoked cytokines, consistent with our conceptual framework. This limited sample size precluded the examination of additional relevant individual differences related to inflammatory processes, such as sex (Irwin et al., 2010; Prather et al., 2009), adiposity (Prather et al., 2013), exercise and physical activity (Helmark et al., 2010; Taaffe et al., 2000), and possibly more nuanced sleep characteristics (Irwin, 2002; Irwin et al., 2008). In particular, the role of sex relating to the intersection of chronic pain, insomnia disorder, and inflammation should be the focus of future research. Sex differences in pain sensitivity, chronic pain, and stress-related inflammatory mechanisms have been reported between men and women. In short, compared to men, women tend to be more pain sensitive and have greater chronic pain severity (Bartley and Fillingim, 2013; Fillingim et al., 2009; Paller et al., 2009), as well as a more robust inflammatory response to sleep deprivation (Irwin et al., 2010). Hence, it is possible that women are particularly vulnerable for sleep problems in the context of pain, and vice-versa, possibly via inflammatory mediators. Ultimately, it will be important to replicate and extend these findings in studies that can accommodate the study of potentially important moderators of the OA and insomnia disorder effects observed in the present investigation.
Another limitation was a lack of a no-stress (Steptoe et al., 2007) or placebo control condition (Dickerson et al., 2009). It is possible that the growth in IL-6 had little to do with the pain testing per se, and can be attributed more readily to naturalistic variation, or to some other unmeasured variable. This possibility seems unlikely because prior studies that have included control conditions have shown greater cytokine responses to stressful versus control conditions (Steptoe et al., 2007). Moreover, circadian levels of IL-6 decline throughout the afternoon under resting conditions (Vgontzas et al., 2005), and our assessments were conducted from 1400 to 1600 hours. Although we used a pain testing protocol as our stressor, which seems appropriate for understanding the impact of pain on inflammatory processes associated with factors related to OA risk (e.g., insomnia disorder), we recommend that future studies consider tasks that might carry more direct clinical relevance for OA. For instance, physical function tests, such as a six-minute walk test (Ko et al., 2013; Wideman et al., 2014), may elicit differential inflammatory activity in normal sleepers versus those with insomnia disorder. Finally, we evaluated a single pro- and anti-inflammatory cytokine, respectively. We selected IL-6 given its sensitivity to laboratory pain testing methods similar to those employed in the current study (Edwards et al., 2008; Edwards et al., 2009b; Lee et al., 2011) and psychosocial stress (Dickerson et al., 2009; Heffner et al., 2012; Prather et al., 2009; Prather et al., 2013) and various indicators of sleep disturbance (Irwin, 2002; Irwin et al., 2010; Irwin et al., 2008; Redwine et al., 2000), as well as its established role in OA (Livshits et al., 2009; Stannus et al., 2010; Stannus et al., 2013). IL-10 was selected because of its reported role in sleep physiology (Opp, 2005), chondroprotectivity (Wojdasiewicz et al, 2014) and relative risk of developing OA (Riyazi et al., 2005). Future studies should consider examination of a larger set of cytokines related to sleep disturbance, pain, aging and OA.
To conclude, we evaluated the influence of insomnia disorder on resting and pain-evoked markers of inflammation in older adults with or without KOA. We observed that KOA and insomnia disorder were associated with greater IL-6 and IL-10 levels in the context of pain-induction, and that insomnia disorder was associated with exaggerated and protracted pain-evoked increases in IL-6. The association between KOA and IL-6 levels was largely attributable to individual differences in BMI and age. When considered in context with the broader literature on sleep problems, pain and inflammation, these findings may suggest pro-inflammatory cytokines as a mechanism by which insomnia disorder can confer disease risk among older adults, perhaps particular related to painful or stressful events. The careful study of interventions designed to mitigate insomnia disorder and obesity in older adults appear warranted, and the degree to which doing can improve health and well-being through resultant changes in systemic inflammatory activity.
Highlights.
Insomnia disorder predicted pain-evoked IL-6 response
The association between osteoarthritis and IL-6 was accounted for by BMI and age
Insomnia disorder and osteoarthritis were associated with greater IL-10 levels
Laboratory pain testing evokes variability in IL-6 and IL-10 responses
The clinical relevance of a pain-evoked inflammatory response requires further study
Acknowledgments
This research study was supported by grants NIH/NIDA 1K23DA035915 (PHF) and NIH/NIAMS grants R01 AR05487 (MTS) and R01 AR059410 (MTS)
Footnotes
KOA + Insomnia Disorder participants were oversampled for enrollment in a randomized controlled trial of Cognitive Behavioral Therapy for Insomnia (CBT-I) in patients with KOA with Insomnia Disorder. These data will be presented elsewhere.
Disclaimer
The opinions or assertions contained herein are the private views of the authors, and are not to be construed as official, or as reflecting true views, of the Department of the Army or the Department of Defense.
Conflicts of Interest
Dr. Michael Smith holds an equity stake in BMED Technologies, which is managed by the Johns Hopkins Office on Conflict of Interest. The authors have no additional disclosures.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abad VC, Sarinas PS, Guilleminault C. Sleep and rheumatologic disorders. Sleep Med Rev. 2008;12:211–228. doi: 10.1016/j.smrv.2007.09.001. [DOI] [PubMed] [Google Scholar]
- Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis and rheumatism. 1986;29:1039–1049. doi: 10.1002/art.1780290816. [DOI] [PubMed] [Google Scholar]
- Altman R, Brandt K, Hochberg M, Moskowitz R, Bellamy N, Bloch DA, Buckwalter J, Dougados M, Ehrlich G, Lequesne M, Lohmander S, Murphy WA, Jr, Rosario-Jansen T, Schwartz B, Trippel S. Design and conduct of clinical trials in patients with osteoarthritis: recommendations from a task force of the Osteoarthritis Research Society. Results from a workshop. Osteoarthritis Cartilage. 1996;4:217–243. doi: 10.1016/s1063-4584(05)80101-3. [DOI] [PubMed] [Google Scholar]
- Barker T, Rogers VE, Henriksen VT, Aguirre D, Trawick RH, Rasmussen GL, Momberger NG. Serum cytokines are increased and circulating micronutrients are not altered in subjects with early compared to advanced knee osteoarthritis. Cytokine. 2014;68:133–136. doi: 10.1016/j.cyto.2014.04.004. [DOI] [PubMed] [Google Scholar]
- Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. British journal of anaesthesia. 2013;111:52–58. doi: 10.1093/bja/aet127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep medicine. 2001;2:297–307. doi: 10.1016/s1389-9457(00)00065-4. [DOI] [PubMed] [Google Scholar]
- Bellamy N. Pain assessment in osteoarthritis: experience with the WOMAC osteoarthritis index. Semin Arthritis Rheum. 1989;18:14–17. doi: 10.1016/0049-0172(89)90010-3. [DOI] [PubMed] [Google Scholar]
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. [PubMed] [Google Scholar]
- Brinkley TE, Leng X, Miller ME, Kitzman DW, Pahor M, Berry MJ, Marsh AP, Kritchevsky SB, Nicklas BJ. Chronic inflammation is associated with low physical function in older adults across multiple comorbidities. J Gerontol A Biol Sci Med Sci. 2009;64:455–461. doi: 10.1093/gerona/gln038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brydon L. Adiposity, leptin and stress reactivity in humans. Biol Psychol. 2011;86:114–120. doi: 10.1016/j.biopsycho.2010.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burgos I, Richter L, Klein T, Fiebich B, Feige B, Lieb K, Voderholzer U, Riemann D. Increased nocturnal interleukin-6 excretion in patients with primary insomnia: a pilot study. Brain Behav Immun. 2006;20:246–253. doi: 10.1016/j.bbi.2005.06.007. [DOI] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry research. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- Carman WJ, Sowers M, Hawthorne VM, Weissfeld LA. Obesity as a risk factor for osteoarthritis of the hand and wrist: a prospective study. Am J Epidemiol. 1994;139:119–129. doi: 10.1093/oxfordjournals.aje.a116974. [DOI] [PubMed] [Google Scholar]
- Cesari M, Penninx BW, Pahor M, Lauretani F, Corsi AM, Rhys Williams G, Guralnik JM, Ferrucci L. Inflammatory markers and physical performance in older persons: the InCHIANTI study. J Gerontol A Biol Sci Med Sci. 2004;59:242–248. doi: 10.1093/gerona/59.3.m242. [DOI] [PubMed] [Google Scholar]
- Coughlin JW, Smith MT. Sleep, obesity, and weight loss in adults: Is there a rationale for providing sleep interventions in the treatment of obesity? Int Rev Psychiatry. 2014;26:177–188. doi: 10.3109/09540261.2014.911150. [DOI] [PubMed] [Google Scholar]
- Daftarian PM, Kumar A, Kryworuchko M, Diaz-Mitoma F. IL-10 production is enhanced in human T cells by IL-12 and IL-6 and in monocytes by tumor necrosis factor-alpha. J Immunol. 1996;157:12–20. [PubMed] [Google Scholar]
- Das UN. Is obesity an inflammatory condition? Nutrition. 2001;17:953–966. doi: 10.1016/s0899-9007(01)00672-4. [DOI] [PubMed] [Google Scholar]
- Dickerson SS, Gable SL, Irwin MR, Aziz N, Kemeny ME. Social-evaluative threat and proinflammatory cytokine regulation: an experimental laboratory investigation. Psychol Sci. 2009;20:1237–1244. doi: 10.1111/j.1467-9280.2009.02437.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edinger JD, Bonnet MH, Bootzin RR, Doghramji K, Dorsey CM, Espie CA, Jamieson AO, McCall WV, Morin CM, Stepanski EJ American Academy of Sleep Medicine Work G. Derivation of research diagnostic criteria for insomnia: report of an American Academy of Sleep Medicine Work Group. Sleep. 2004;27:1567–1596. doi: 10.1093/sleep/27.8.1567. [DOI] [PubMed] [Google Scholar]
- Edwards RR, Grace E, Peterson S, Klick B, Haythornthwaite JA, Smith MT. Sleep continuity and architecture: associations with pain-inhibitory processes in patients with temporomandibular joint disorder. Eur J Pain. 2009a;13:1043–1047. doi: 10.1016/j.ejpain.2008.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards RR, Kronfli T, Haythornthwaite JA, Smith MT, McGuire L, Page GG. Association of catastrophizing with interleukin-6 responses to acute pain. Pain. 2008;140:135–144. doi: 10.1016/j.pain.2008.07.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards RR, Wasan AD, Bingham CO, 3rd, Bathon J, Haythornthwaite JA, Smith MT, Page GG. Enhanced reactivity to pain in patients with rheumatoid arthritis. Arthritis research & therapy. 2009b;11:R61. doi: 10.1186/ar2684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engstrom G, Gerhardsson de Verdier M, Rollof J, Nilsson PM, Lohmander LS. C-reactive protein, metabolic syndrome and incidence of severe hip and knee osteoarthritis. A population-based cohort study. Osteoarthritis Cartilage. 2009;17:168–173. doi: 10.1016/j.joca.2008.07.003. [DOI] [PubMed] [Google Scholar]
- Faraut B, Boudjeltia KZ, Vanhamme L, Kerkhofs M. Immune, inflammatory and cardiovascular consequences of sleep restriction and recovery. Sleep Medicine Reviews. 2012;16:137–149. doi: 10.1016/j.smrv.2011.05.001. [DOI] [PubMed] [Google Scholar]
- Fielden JM, Gander PH, Horne JG, Lewer BM, Green RM, Devane PA. An assessment of sleep disturbance in patients before and after total hip arthroplasty. J Arthroplasty. 2003;18:371–376. doi: 10.1054/arth.2003.50056. [DOI] [PubMed] [Google Scholar]
- Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL., III Sex, gender, and pain: a review of recent clinical and experimental findings. The Journal of Pain. 2009;10:447–485. doi: 10.1016/j.jpain.2008.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finan PH, Buenaver LF, Bounds SC, Hussain S, Park RJ, Haque UJ, Campbell CM, Haythornthwaite JA, Edwards RR, Smith MT. Discordance between pain and radiographic severity in knee osteoarthritis: findings from quantitative sensory testing of central sensitization. Arthritis and rheumatism. 2013;65:363–372. doi: 10.1002/art.34646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiorentino DF, Zlotnik A, Mosmann TR, Howard M, O’Garra A. IL-10 inhibits cytokine production by activated macrophages. J Immunol. 1991;147:3815–3822. [PubMed] [Google Scholar]
- Haack M, Sanchez E, Mullington JM. Elevated inflammatory markers in response to prolonged sleep restriction are associated with increased pain experience in healthy volunteers. Sleep. 2007;30:1145–1152. doi: 10.1093/sleep/30.9.1145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haack M, Scott-Sutherland J, Santangelo G, Simpson NS, Sethna N, Mullington JM. Pain sensitivity and modulation in primary insomnia. Eur J Pain. 2012;16:522–533. doi: 10.1016/j.ejpain.2011.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heffner KL, Ng HM, Suhr JA, France CR, Marshall GD, Pigeon WR, Moynihan JA. Sleep disturbance and older adults’ inflammatory responses to acute stress. Am J Geriatr Psychiatry. 2012;20:744–752. doi: 10.1097/JGP.0b013e31824361de. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helmark IC, Mikkelsen UR, Borglum J, Rothe A, Petersen MC, Andersen O, Langberg H, Kjaer M. Exercise increases interleukin-10 levels both intraarticularly and peri-synovially in patients with knee osteoarthritis: a randomized controlled trial. Arthritis research & therapy. 2010;12:R126. doi: 10.1186/ar3064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irwin M. Effects of sleep and sleep loss on immunity and cytokines. Brain Behav Immun. 2002;16:503–512. doi: 10.1016/s0889-1591(02)00003-x. [DOI] [PubMed] [Google Scholar]
- Irwin MR, Carrillo C, Olmstead R. Sleep loss activates cellular markers of inflammation: sex differences. Brain Behav Immun. 2010;24:54–57. doi: 10.1016/j.bbi.2009.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irwin MR, Wang M, Ribeiro D, Cho HJ, Olmstead R, Breen EC, Martinez-Maza O, Cole S. Sleep loss activates cellular inflammatory signaling. Biol Psychiatry. 2008;64:538–540. doi: 10.1016/j.biopsych.2008.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–545. doi: 10.1093/sleep/14.6.540. [DOI] [PubMed] [Google Scholar]
- Ko V, Naylor JM, Harris IA, Crosbie J, Yeo AE. The six-minute walk test is an excellent predictor of functional ambulation after total knee arthroplasty. BMC Musculoskelet Disord. 2013;14:145. doi: 10.1186/1471-2474-14-145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee YC, Lu B, Bathon JM, Haythornthwaite JA, Smith MT, Page GG, Edwards RR. Pain sensitivity and pain reactivity in osteoarthritis. Arthritis Care Res (Hoboken) 2011;63:320–327. doi: 10.1002/acr.20373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leigh TJ, Bird HA, Hindmarch I, Wright V. A comparison of sleep in rheumatic and non-rheumatic patients. Clin Exp Rheumatol. 1987;5:363–365. [PubMed] [Google Scholar]
- Livshits G, Zhai G, Hart DJ, Kato BS, Wang H, Williams FM, Spector TD. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: The Chingford Study. Arthritis and rheumatism. 2009;60:2037–2045. doi: 10.1002/art.24598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luyster FS, Strollo PJ, Jr, Zee PC, Walsh JK. Sleep: a health imperative. Sleep. 2012;35:727–734. doi: 10.5665/sleep.1846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall NS, Glozier N, Grunstein RR. Is sleep duration related to obesity? A critical review of the epidemiological evidence. Sleep Med Rev. 2008;12:289–298. doi: 10.1016/j.smrv.2008.03.001. [DOI] [PubMed] [Google Scholar]
- Matzner P, Hazut O, Naim R, Shaashua L, Sorski L, Levi B, Sadeh A, Wald I, Bar-Haim Y, Ben-Eliyahu S. Resilience of the immune system in healthy young students to 30-hour sleep deprivation with psychological stress. Neuroimmunomodulation. 2013;20:194–204. doi: 10.1159/000348698. [DOI] [PubMed] [Google Scholar]
- Mohamed-Ali V, Goodrick S, Rawesh A, Katz DR, Miles JM, Yudkin JS, Klein S, Coppack SW. Subcutaneous adipose tissue releases interleukin-6, but not tumor necrosis factor-alpha, in vivo. J Clin Endocrinol Metab. 1997;82:4196–4200. doi: 10.1210/jcem.82.12.4450. [DOI] [PubMed] [Google Scholar]
- Morin CM, Belleville G, Belanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34:601–608. doi: 10.1093/sleep/34.5.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage. 2013;21:1145–1153. doi: 10.1016/j.joca.2013.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Opp MR. Cytokines and sleep. Sleep Med Rev. 2005;9:355–364. doi: 10.1016/j.smrv.2005.01.002. [DOI] [PubMed] [Google Scholar]
- Paller CJ, Campbell CM, Edwards RR, Dobs AS. Sex-based differences in pain perception and treatment. Pain medicine (Malden, Mass) 2009;10:289–299. doi: 10.1111/j.1526-4637.2008.00558.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prather AA, Carroll JE, Fury JM, McDade KK, Ross D, Marsland AL. Gender differences in stimulated cytokine production following acute psychological stress. Brain Behav Immun. 2009;23:622–628. doi: 10.1016/j.bbi.2008.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prather AA, Puterman E, Epel ES, Dhabhar FS. Poor sleep quality potentiates stress-induced cytokine reactivity in postmenopausal women with high visceral abdominal adiposity. Brain Behav Immun. 2013 doi: 10.1016/j.bbi.2013.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quartana PJ, Wickwire EM, Klick B, Grace E, Smith MT. Naturalistic changes in insomnia symptoms and pain in temporomandibular joint disorder: a cross-lagged panel analysis. Pain. 2010;149:325–331. doi: 10.1016/j.pain.2010.02.029. [DOI] [PubMed] [Google Scholar]
- Redline S, Budhiraja R, Kapur V, Marcus CL, Mateika JH, Mehra R, Parthasarthy S, Somers VK, Strohl KP, Sulit LG, Gozal D, Wise MS, Quan SF. The scoring of respiratory events in sleep: reliability and validity. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine. 2007;3:169–200. [PubMed] [Google Scholar]
- Redwine L, Hauger RL, Gillin JC, Irwin M. Effects of sleep and sleep deprivation on interleukin-6, growth hormone, cortisol, and melatonin levels in humans. J Clin Endocrinol Metab. 2000;85:3597–3603. doi: 10.1210/jcem.85.10.6871. [DOI] [PubMed] [Google Scholar]
- Riyazi N, Slagboom E, de Craen AJ, Meulenbelt I, Houwing-Duistermaat JJ, Kroon HM, van Schaardenburg D, Rosendaal FR, Breedveld FC, Huizinga TW, Kloppenburg M. Association of the risk of osteoarthritis with high innate production of interleukin-1beta and low innate production of interleukin-10 ex vivo, upon lipopolysaccharide stimulation. Arthritis and rheumatism. 2005;52:1443–1450. doi: 10.1002/art.21014. [DOI] [PubMed] [Google Scholar]
- Rolke R, Baron R, Maier C, Tolle TR, Treede RD, Beyer A, Binder A, Birbaumer N, Birklein F, Botefur IC, Braune S, Flor H, Huge V, Klug R, Landwehrmeyer GB, Magerl W, Maihofner C, Rolko C, Schaub C, Scherens A, Sprenger T, Valet M, Wasserka B. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. 2006;123:231–243. doi: 10.1016/j.pain.2006.01.041. [DOI] [PubMed] [Google Scholar]
- Ruiz FS, Andersen ML, Martins RC, Zager A, Lopes JD, Tufik S. Immune alterations after selective rapid eye movement or total sleep deprivation in healthy male volunteers. Innate immunity. 2012;18:44–54. doi: 10.1177/1753425910385962. [DOI] [PubMed] [Google Scholar]
- Santos ML, Gomes WF, Pereira DS, Oliveira DM, Dias JM, Ferrioli E, Pereira LS. Muscle strength, muscle balance, physical function and plasma interleukin-6 (IL-6) levels in elderly women with knee osteoarthritis (OA) Archives of gerontology and geriatrics. 2011;52:322–326. doi: 10.1016/j.archger.2010.05.009. [DOI] [PubMed] [Google Scholar]
- Schenker ML, Mauck RL, Ahn J, Mehta S. Pathogenesis and prevention of posttraumatic osteoarthritis after intra-articular fracture. The Journal of the American Academy of Orthopaedic Surgeons. 2014;22:20–28. doi: 10.5435/JAAOS-22-01-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schramm E, Hohagen F, Grasshoff U, Riemann D, Hajak G, Weess HG, Berger M. Test-retest reliability and validity of the Structured Interview for Sleep Disorders According to DSM-III-R. The American journal of psychiatry. 1993;150:867–872. doi: 10.1176/ajp.150.6.867. [DOI] [PubMed] [Google Scholar]
- Singer JD, Willet JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurence. Oxford University Press; New York: 2003. [Google Scholar]
- Smith MT, Wickwire EM, Grace EG, Edwards RR, Buenaver LF, Peterson S, Klick B, Haythornthwaite JA. Sleep disorders and their association with laboratory pain sensitivity in temporomandibular joint disorder. Sleep. 2009;32:779–790. doi: 10.1093/sleep/32.6.779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stannus O, Jones G, Cicuttini F, Parameswaran V, Quinn S, Burgess J, Ding C. Circulating levels of IL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults. Osteoarthritis Cartilage. 2010;18:1441–1447. doi: 10.1016/j.joca.2010.08.016. [DOI] [PubMed] [Google Scholar]
- Stannus OP, Jones G, Blizzard L, Cicuttini FM, Ding C. Associations between serum levels of inflammatory markers and change in knee pain over 5 years in older adults: a prospective cohort study. Ann Rheum Dis. 2013;72:535–540. doi: 10.1136/annrheumdis-2011-201047. [DOI] [PubMed] [Google Scholar]
- Steptoe A, Hamer M, Chida Y. The effects of acute psychological stress on circulating inflammatory factors in humans: a review and meta-analysis. Brain Behav Immun. 2007;21:901–912. doi: 10.1016/j.bbi.2007.03.011. [DOI] [PubMed] [Google Scholar]
- Taaffe DR, Harris TB, Ferrucci L, Rowe J, Seeman TE. Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur studies of successful aging. J Gerontol A Biol Sci Med Sci. 2000;55:M709–715. doi: 10.1093/gerona/55.12.m709. [DOI] [PubMed] [Google Scholar]
- Tang NK, Goodchild CE, Sanborn AN, Howard J, Salkovskis PM. Deciphering the temporal link between pain and sleep in a heterogeneous chronic pain patient sample: a multilevel daily process study. Sleep. 2012;35:675–687A. doi: 10.5665/sleep.1830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vgontzas AN, Bixler EO, Lin HM, Prolo P, Trakada G, Chrousos GP. IL-6 and its circadian secretion in humans. Neuroimmunomodulation. 2005;12:131–140. doi: 10.1159/000084844. [DOI] [PubMed] [Google Scholar]
- Vgontzas AN, Zoumakis M, Papanicolaou DA, Bixler EO, Prolo P, Lin HM, Vela-Bueno A, Kales A, Chrousos GP. Chronic insomnia is associated with a shift of interleukin-6 and tumor necrosis factor secretion from nighttime to daytime. Metabolism. 2002;51:887–892. doi: 10.1053/meta.2002.33357. [DOI] [PubMed] [Google Scholar]
- Vitiello MV, McCurry SM, Shortreed SM, Baker LD, Rybarczyk BD, Keefe FJ, Von Korff M. Short-term improvement in insomnia symptoms predicts long-term improvements in sleep, pain, and fatigue in older adults with comorbid osteoarthritis and insomnia. Pain. 2014 doi: 10.1016/j.pain.2014.04.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wideman TH, Finan PH, Edwards RR, Quartana PJ, Buenaver LF, Haythornthwaite JA, Smith MT. Increased sensitivity to physical activity among individuals with knee osteoarthritis: relation to pain outcomes, psychological factors, and responses to quantitative sensory testing. Pain. 2014;155:703–711. doi: 10.1016/j.pain.2013.12.028. [DOI] [PubMed] [Google Scholar]
- Wilcox S, Brenes GA, Levine D, Sevick MA, Shumaker SA, Craven T. Factors related to sleep disturbance in older adults experiencing knee pain or knee pain with radiographic evidence of knee osteoarthritis. J Am Geriatr Soc. 2000;48:1241–1251. doi: 10.1111/j.1532-5415.2000.tb02597.x. [DOI] [PubMed] [Google Scholar]
- Wojdasiewicz P, Poniatowski LA, Szukiewicz D. The Role of Inflammatory and Anti-Inflammatory Cytokines in the Pathogenesis of Osteoarthritis. 2014;2014:561459. doi: 10.1155/2014/561459. [DOI] [PMC free article] [PubMed] [Google Scholar]