
Figure 2.
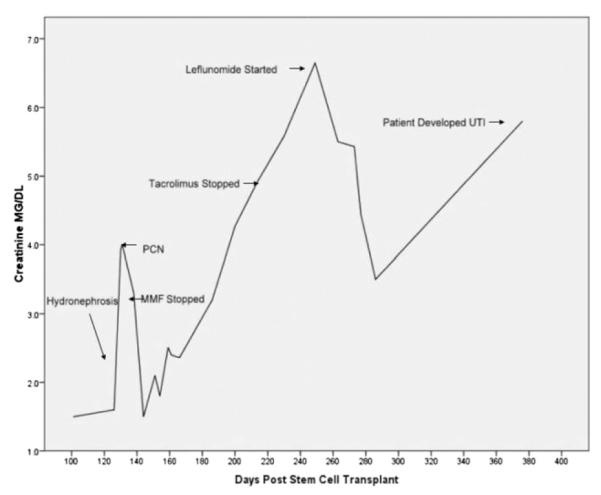
Serum creatinine measurements beginning 100 days following transplantation in patient diagnosed with BK-associated hemorrhagic cystitis and nephropathy following a double cord blood transplant. The patient developed BK viruria, with >5 × 108 virus copies/mL urine, associated with hemorrhagic cystitis, 39 days post-HCT. At 105 days post-HCT, there was a rise in creatinine up to 3.6 mg/dL that was noted to be because of bilateral hydronephrosis, diagnosed by renal ultrasound, in the setting of persistent BK viruria, with improvement in creatinine following placement of bilateral percutaneous nephropathy tubes. Immunosuppression was also discontinued at this time. The presence of renal failure prohibited the use of cidofovir, so leflunomide was initiated on day +263, and over the course of 3 weeks, the creatinine decreased from 6.7 mg/dL to 3.5 mg/dL, with a 75% reduction in BK viruria from >5 × 108 to 1.25 × 108 copies of virus/mL urine. At approximately 1 year posttransplantation, 6.86 × 105 copies of virus/mL of urine was noted after taking leflunomide for approximately 15 weeks. However, the patient subsequently developed another rise in her creatinine concurrent with the development of a pseudomonas urinary tract infection. The patient remains on leflunomide at 20 mg daily, with no liver or bone marrow toxicities noted.