
Figure 2.
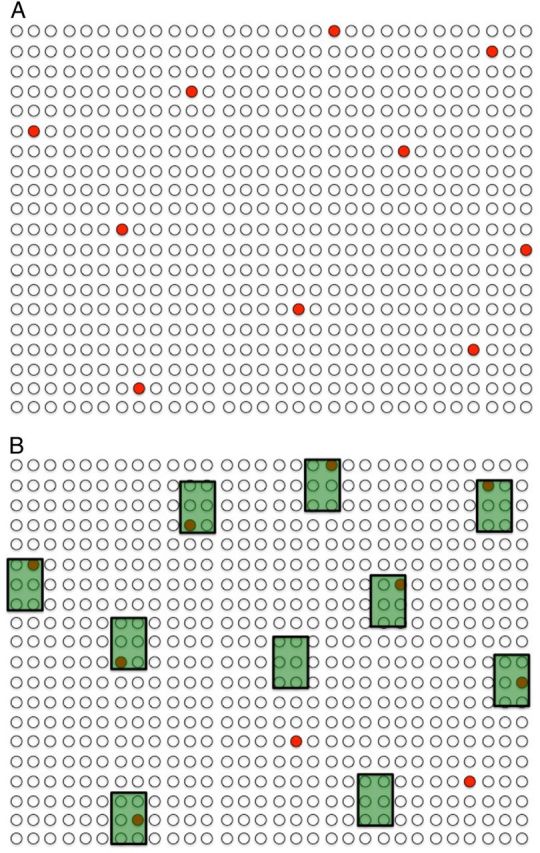
Catalysts of tuberculosis transmission. Closed (or black) dots represent 10 cases of prevalent infectious tuberculosis in a community of 600 individuals (ie, prevalence of >1600 per 100 000—note that tuberculosis is a rare disease even at a prevalence >10 times the global average). These individuals represent the “tuberculosis infectious pool” responsible for ongoing transmission in the community. A, A naive evaluation considers these tuberculosis cases to be randomly distributed, suggesting that 60 people without tuberculosis would need to be screened to find and treat 1 case of active tuberculosis (10% of the infectious pool). B, In reality, tuberculosis cases in a community often cluster according to transmission catalysts—shown as shaded boxes—that increase contact rates, infectiousness, and susceptibility. These catalysts may not be immediately recognizable to local disease control officials without additional data. However, if data can be collected and the key catalysts identified, screening (or other tuberculosis control efforts) can be targeted accordingly. In this hypothetical example, screening the 10% of the population that was associated with specific catalysts (eg, sites of high transmission [eg, prison, public transit], increased susceptibility profiles [eg, low body mass index, human immunodeficiency virus], or long infectious periods [eg, long distance from clinic, poor access to care]) would identify 80% of infectious tuberculosis cases.