
Fig. 1.
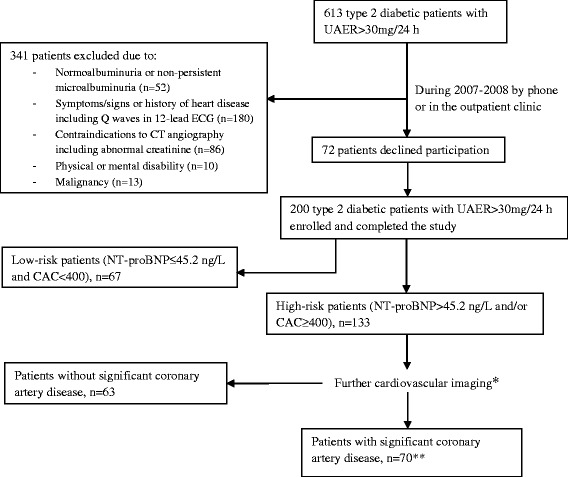
Selection of the study population and algorithm used for risk group assessment with the use of plasma NT-proBNP and coronary artery calcium score (CAC). * (i) patients with P-NT-proBNP >45.2 ng/L underwent myocardial perfusion imaging. Patients with abnormal myocardial perfusion imaging (n = 55) or CAC >100 (n =29) were referred for coronary angiography; (ii) patients with P-NT-proBNP ≤ 45.2 ng/L and CAC 400–1000 underwent CT angiography (n = 20); CT angiography was only used in patients with CAC 400–1000 since severe coronary artery calcifications (CAC > 1000) compromise the validity of CT angiography. Patients with abnormal CT angiography were referred for coronary angiography (n =15) and (iii) patients with P-NT-proBNP ≤ 45.2 ng/L and CAC >1000 underwent myocardial perfusion imaging (n =9). Patients with abnormal myocardial perfusion imaging (n = 6) were referred for coronary angiography.**Significant coronary artery disease was defined as the presence of one or more significant myocardial perfusion defects on myocardial perfusion imaging, and/or one or more significant major epicardial coronary artery stenosis at coronary angiography