

Abstract
Bacillus Calmette-Guerin (BCG) is considered the most effective adjunctive treatment available to treat superficial bladder carcinoma. Although BCG is well tolerated by most patients, it may be associated with adverse effects. One of these is BCG granulomas in the kidney. We herein report a case of a 52-year-old patient who, during a surveillance contrast-enhanced computed tomography (CT) scan, was found to have multiple hypodense lesions in the left kidney. Ultrasound-guided biopsy proved it to be BCG granulomas. After 3 months of anti-tubercular treatment, a repeat CT showed complete resolution of the lesions.
Keywords: Bladder carcinoma, intravesical Bacillus Calmette-Guerin treatment, BCG complications, granulomatous disease
INTRODUCTION
Intravesical instillation of Bacillus Calmette-Guérin (BCG) is an important adjunct to transurethral resection of bladder tumor in patients with superficial disease to reduce the risk of recurrence and progression. BCG is used in patients with stage T1 tumors, carcinoma in situ or stage Ta tumors of high grade. BCG is well tolerated by most of the patients, but this can be associated with a legion of adverse effects. Minor toxicities like frequency, urgency, dysuria and hematuria have been reported in 27–90% of the patients. Granulomatous complications like prostatitis, epididymo-orchitis, cystitis, pyelonephritis and abscess have been reported uncommonly. The incidence of significant renal toxicity varies from 0.2% to 2%. We herein report a case of asymptomatic BCG granulomatosis of the kidney in a patient receiving intravesical BCG treatment.
CASE REPORT
A 52-year-old male patient was referred to us for maintenance intravesical BCG immunotherapy. He had undergone transurethral resection of bladder tumor (TURBT) for low-grade T1 tumor on the left lateral wall and another small tumor near the left ureteric orifice at another hospital. One month later, he underwent restaging TURBT that was negative for malignancy. He also received an induction course of intravesical BCG in the same center. At our center, the patient was started on monthly maintenance BCG therapy with regular surveillance cystoscopy and urine cytology. Further, as the patient was in the high-risk category and one of the tumors was near the ureteric orifice, a contrast-enhanced computed tomography (CT) scan with urogram as a surveillance protocol was performed at the end of 1 year. This showed multifocal hypodense lesions in the left kidney [Figure 1]. Urine cytology showed inflammatory neutrophils only. An ultrasound-guided biopsy was taken from the left renal lesion. Histopathology revealed a necrotizing granulomatous lesion consistent with BCG granulomatosis [Figures 2 and 3]. After 3 months of antituberculous treatment, a repeat contrast-enhanced CT scan showed complete resolution of lesions in the left kidney [Figure 4].
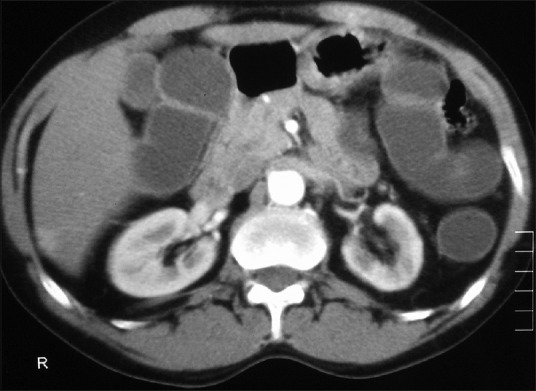
Figure 1.

Axial contrast-enhanced computed tomography image of the abdomen showing multiple hypodense masses in the left kidney
Figure 2.
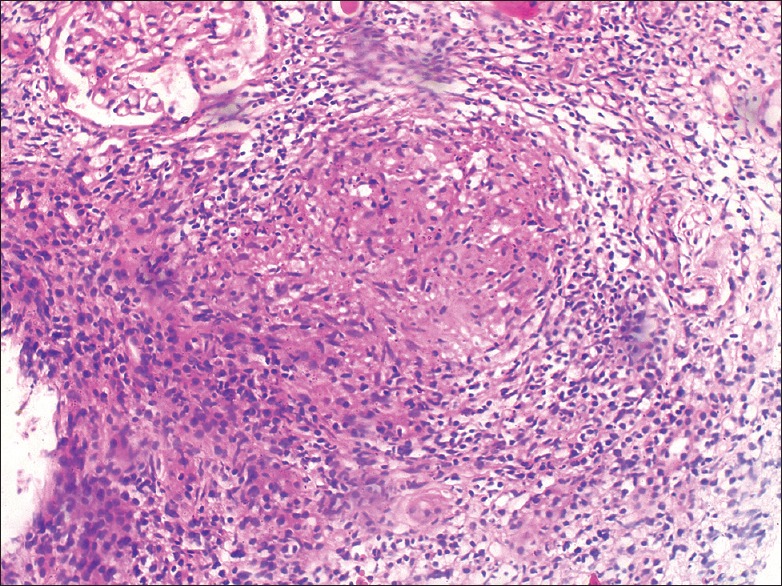
Hemotoxylin and eosin staining showing necrotizing granuloma (arrow) and adjacent normal glomerulus. Magnification, 10 X
Figure 3.
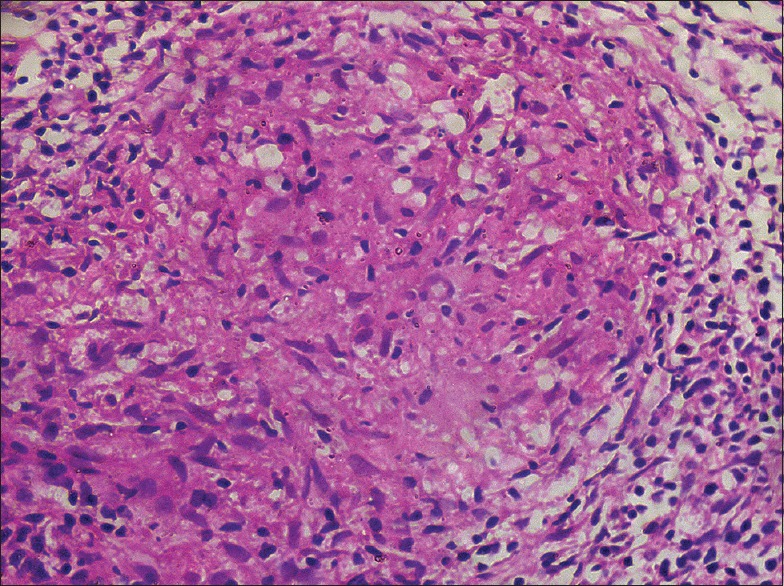
Hematoxylin and eosin staining showing necrotizing granuloma with a surrounding collar of macrophages and lymphocytes. Magnification, 40 X
Figure 4.
Axial contrast-enhanced computed tomography image of the abdomen 3 months after anti tuberculous treatment showing complete resolution of the lesions
DISCUSSION
Intravesical BCG is the most effective adjunctive agent in the management of superficial bladder cancer. It has been widely used since the initial report by Morales et al. in 1976 for reducing the recurrence and progression rate. Even though most patients (>95%) tolerate it well, both local and systemic effects can occur. The local toxicities like irritative lower urinary tract symptoms (LUTS), gross hematuria, etc., are common and usually occur after 3rd instillation when the lymphokine release causes maximal inflammatory response. Systemic complications like flu-like symptoms, myalgia, high-grade fever (2.9%), significant hematuria (1%), granulomatous prostatitis (0.9%), pneumonitis and/or hepatitis (0.7%), arthralgia (0.5%), epididymitis (0.4%), sepsis (0.4%), rash (0.3%), ureteral obstruction (0.3%), contracted bladder (0.2%), renal abscess (0.1%) and cytopenia (0.1%) also occur.[1]
Renal affliction by intravesical BCG instillation occurs in <0.1% of patients. In most of the reported cases, the renal lesions presented as pyelonephritis at 3rd or 4th dose of BCG instillation. Our patient remained asymptomatic throughout the course of BCG instillations. Ma et al. reported two patients with asymptomatic renal masses suggestive of BCG granulomas.[2] The mechanism of renal affliction of kidney by BCG has been postulated to be due to vesicoureteric reflux or by the hematogenous route. Vesicoureteric reflux is common following TURBT. A review of the literature by Mazemen et al. showed the presence of reflux in 237 of 899 patients treated by transurethral resection (TUR).[3] Some authors believe that reflux might be theoretically beneficial as it might prevent upper tract recurrences in patients with bladder cancer.[4] In our case, one of the tumors was situated very close to the left ureteric orifice, and resection of this might have led to reflux leading to granuloma formation.
BCG granulomas usually appear as enhancing lesions on contrast-enhanced CT. Some are segmental in appearance and associated with minimal perinephric stranding. Expansile and mass-like lesions mimicking tumor have also been described.[2] Senes et al. have described a “central unaffected calyx sign,” which the authors claim to be specific for renal BCG granulomas. Their study showed BCG granulomatosis in the form of a solid mass in the kidney with a central normal calyx within it.[5] In our case, CT showed multiple hypodense lesions in the left kidney, which was proved to be BCG granulomatosis by biopsy. This report emphasizes the need for strict follow-up imaging, wherein lesions can be picked up in the asymptomatic stage and can be treated early and promptly.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Lamm DL. Efficacy and safety of bacille Calmette-Guérin immunotherapy in superficial bladder cancer. Clin Infect Dis. 2000;31(Suppl 3):S86–92. doi: 10.1086/314064. [DOI] [PubMed] [Google Scholar]
- 2.Ma W, Kang S K, Hricak H, Gerst SR, Zhang J. Imaging appearance of granulomatous disease after intravesical Bacille Calmette-Guerin (BCG) treatment of bladder carcinoma. AJR Am J Roentgenol. 2009;192:1494–500. doi: 10.2214/AJR.08.1962. [DOI] [PubMed] [Google Scholar]
- 3.Mazeman E, Gilliot P. Vesicorenal reflux and intravesical chemotherapy. Prog Clin Boil Res. 1989;303:517–22. [PubMed] [Google Scholar]
- 4.Gonzlez JA, Marcol BR, Wolf MC. Complications of intravesical BCG: A case report. J Urol. 1992;142:1892–3. doi: 10.1016/s0022-5347(17)37062-3. [DOI] [PubMed] [Google Scholar]
- 5.Senés AT, Badet L, Lyonnet D, Rouvière O. Granulomatous renal masses following intravesical bacillus Calmette–Guérin therapy: The central unaffected calyx sign. Br J Radiol. 2007;80:e230–3. doi: 10.1259/bjr/42250860. [DOI] [PubMed] [Google Scholar]