
Figure 2.
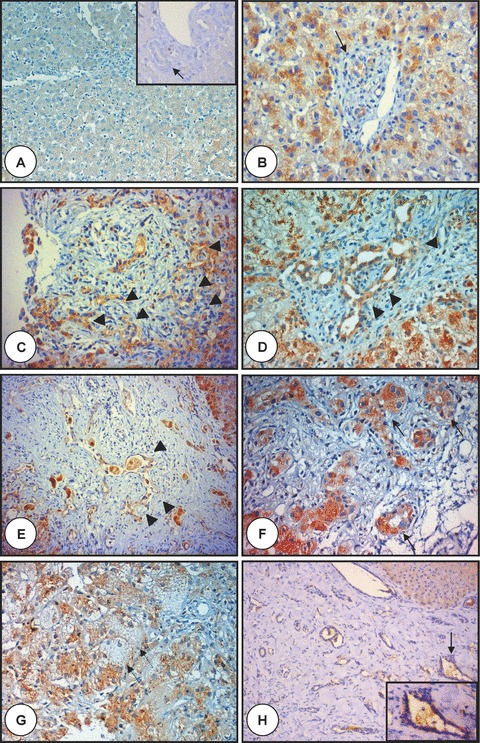
Polyductin expression in liver disease of newborns and infants. In (A), there is liver tissue with a baseline staining (anti-FP2, ×100) with no staining of the interlobular bile duct (arrow) (inset, anti-FP2, ×320); (B) and (C) show two examples of biliary atresia with ductular proliferation without ductal plate malformation at early (B) (the arrow points to a bile duct) and advanced (C) stage showing the ductular proliferation (arrowheads) of biliary atresia with a moderate FP2 staining (anti-FP2, ×400); (D) and (E) show two examples of biliary atresia with ductal plate malformation showing biliary structures (arrowheads) at early (D) and advanced (E) stage showing moderate FP2 staining (anti-FP2, d:×400, e:×200); (F) and (G) show liver tissue affected with neonatal hepatitis with mostly an intense staining of both pseudorosettes and neoductuli (arrows with continuous line), whereas giant cells show mostly very faint staining (arrow with dotted line) (anti-FP2, ×400). In (H) is shown liver tissue from an infant with congenital liver fibrosis (note the lack of ductular proliferation at the edges of the portal tracts) showing moderate diffuse FP2 staining of the biliary structures, whereas the hepatocytes show a mild diffuse staining. The arrows point to a selected region shown in inset. Note the enlarged biliary structure with moderate FP2 staining (anti-FP2, ×200 and ×320 in the inset).