

Abstract
Retained surgical sponge (gossypiboma) following an inguinal herniorrhaphy is a rare condition and may cause medicolegal problems. Differential diagnosis for the lesion should be made meticulously. We report a case of a 45-year-old man who had a herniorrhaphy about 8 years previously. He presented one episode of painless gross hematuria. Laboratory and imaging studies excluded any significant lesion in the urological organs. Abdominal CT scan demonstrated a heterogeneous neoplasm of 4 cm in size in the left paravesical area that was retrieved laparoscopically. Abdominal CT and clinical suspicion are helpful for diagnosis. Laparoscopy may be used to confirm the diagnosis and to remove the retained surgical gauze, and considered as an alternative therapy for some selected patients.
Keywords: Gossypiboma, herniorrhaphy, laparoscopy
INTRODUCTION
Retained surgical sponge, also called gossypiboma or textiloma, or instrument is a serious iatrogenic complication that may occur after almost any surgical and even nonsurgical procedures including abdominal, urological, gynecological and obstetrical, endoscopic procedure, and orthopedic surgeries. A surgical sponge constitutes the most frequently encountered object because of its common usage, size, and amorphous structure.[1] Laparotomy has been known as the most common procedure associated with retained surgical sponge.[1] Herein, we present an unusual case of paravesical gossypiboma treated via the laparoscopic approach.
CASE REPORT
A 45-year-old man presented with painless gross hematuria for 2 days. There was no previous history of dysuria. The patient had undergone a left inguinal herniorrhaphy 8 years earlier and an operative scar of 4 cm in length was left. The abdomen was soft and flat. Laboratory findings were all within the normal range. Abdominal radiography and echography revealed no radiopaque lesion in the urological organs. Further evaluation with CT scan demonstrated a well-defined encapsulated mass with heterogeneous density located at the left paravesical area [Figure 1]. A diagnosis of soft tissue neoplasm was made.
Figure 1.
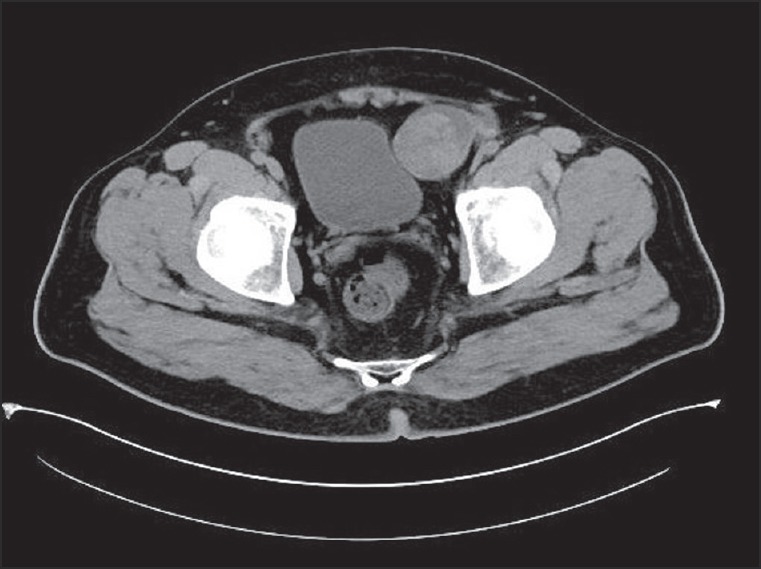
Abdominal CT showing a round, heterogeneous and low dense mass with a thin, hyperdense capsule at the left paravesical area
Under general anesthesia, the patient was operated on via laparoscopic approach in supine position. After creation of a pneumoperitoneum, a 10-mm periumbilical port and two 5-mm ports in the left and right lower quadrants were made. On inspecting the pelvic cavity, a golf ball-sized tumor arising from the preperitoneal space lateral to the left side of the urinary bladder was found [Figure 2a]. Following sharp dissection on the tumor capsule, a piece of surgical gauze with odorless seropurulent fluid was disclosed [Figure 2b]. The gauze was removed by expanding the wound in the peritoneal part of the mass [Figures 2c and d]. After evacuation of the cavity of the mass, a rubber catheter was placed as a drain. The patient got an uneventful recovery and was discharged on the third postoperative day.
Figure 2.
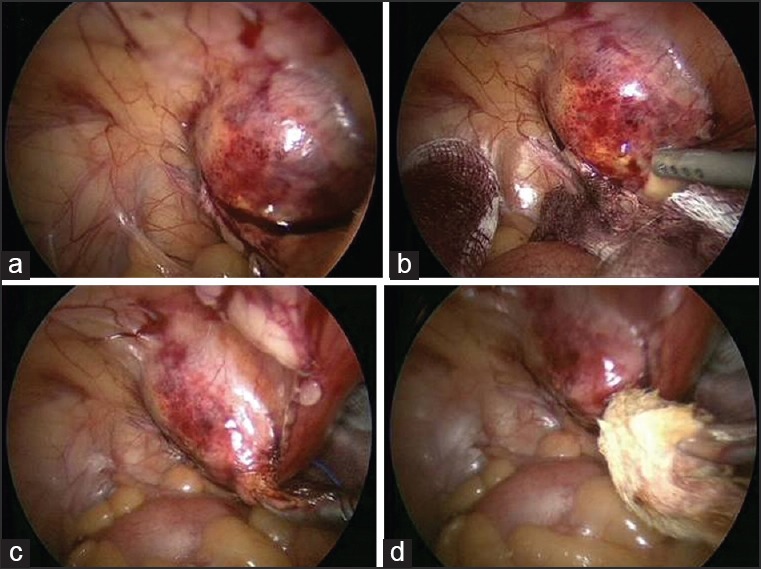
Laparoscopy showing a paravesical tumor lateral to the left side of the urinary bladder. (a) Following sharp dissection on the tumor capsule, yellowish seropurulent fluid being drained outside the tumor. (b) A surgical gauze being removed from the tumor. (c and d)
DISCUSSION
The incidence of retained surgical foreigner bodies varied from 1 in 8801 to 1 in 18,760 inpatient operations at acute care hospitals in USA.[1] The recorded incidence of gossypiboma may be just the tip of the iceberg, possibly due to a reluctance to report occurrences leading to legal implications. Rarely, a retained surgical sponge following an inguinal herniorrhaphy is mentioned in the literature.[2] Several factors including an emergency operation, an unexpected change in procedure, long duration operations, hurried sponge counts, inexperienced staff, inadequate number of staff, change in operating room staff, patients’ unstable condition, and obesity of patients, have been reported to increase the risk for leaving sponge and instruments.[1,3] Identification and removal of a sponge may become more difficult or complicated in the situations of intraoperative bleeding, prolonged case fatigue, and operation in deep anatomical regions.
Most patients with gossypiboma present nonspecific manifestations varying from mild discomfort and pain to fever and bowel obstruction, depending on the location of the sponge and the progress of inflammatory reaction.[2,3] However, several patients were found to be asymptomatic and incidentally discovered[1,2,3] as in this case. It has been reported that 50% of gossypiboma are discovered as late as 5 years or more after surgery.[4] The diagnosis of gossypiboma is usually aided by imaging studies and clinical suspicion, in which a gossypiboma may present curved or banded radio-opaque lines on plain radiograph. CT may manifest a cystic lesion with internal spongiform appearance with mottled shadows as bubbles, thin hyperdense capsule, concentric layering, or mottled mural calcifications.[2,3] Nevertheless, the condition is frequently misdiagnosed and often unnecessary radical surgical procedures are performed because it is not anticipated.[3]
Exploratory laparotomy for removal of the intraabdominal foreign body, percutaneous extraction for intraperitoneal retained foreign bodies and endoscopic retrieval for an intragastric gossypiboma has been successfully described.[2,3,5] Recently it has been claimed that laparoscopy may provide simultaneous diagnostic and therapeutic benefit for the treatment of retained surgical pad, gauze, and instruments.[2,3] The current recommendations suggest that the laparoscopic approach could be attempted in recent, small inflammatory pseudotumors, with obvious encapsulation and no complications.[3] Our experience also indicates that laparoscopy is a feasible and beneficial surgical alternative for the management of a paravesical gossypiboma. Proper team interaction between the surgeon and nurses can definitely eliminate this medicolegal problem.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003;348:229–35. doi: 10.1056/NEJMsa021721. [DOI] [PubMed] [Google Scholar]
- 2.Lauwers PR, Van Hee RH. Intraperitoneal gossypibomas: The need to count sponges. World J Surg. 2000;24:521–7. doi: 10.1007/s002689910084. [DOI] [PubMed] [Google Scholar]
- 3.Târcoveanu E, Dimofte G, Georgescu S, Vasilescu A, Lupaşcu C, Bradea C, et al. Laparoscopic retrieval of gossypibomas - short series and review of literature. Acta Chir Belg. 2011;111:366–9. doi: 10.1080/00015458.2011.11680774. [DOI] [PubMed] [Google Scholar]
- 4.Rappaport W, Haynes K. The retained surgical sponge following intra-abdominal surgery: A continuing problem. Arch Surg. 1990;125:405–7. doi: 10.1001/archsurg.1990.01410150127025. [DOI] [PubMed] [Google Scholar]
- 5.Erdil A, Kilciler G, Ates Y, Tuzun A, Gulsen M, Karaeren N, et al. Transgastric migration of retained intraabdominal surgical sponge: Gossypiboma in the bulbus. Intern Med. 2008;47:613–5. doi: 10.2169/internalmedicine.47.0391. [DOI] [PubMed] [Google Scholar]