

Abstract
Many variants of the long head of the biceps tendon exist but their appearance has not been documented with ultrasonography (US). We describe a case of variant LHB anatomy that was visualized by magnetic resonance imaging and confirmed with US. Additionally, US was useful to exclude instability of the LHBT. To the best of our knowledge, this variant appearance of the LHBT has not been previously described with US. Considering that shoulder US is routinely performed clinically, knowledge of the appearance of variant LHBT anatomy may be useful.
Electronic supplementary material
The online version of this article (doi:10.1007/s40477-014-0125-2) contains supplementary material, which is available to authorized users.
Riassunto
Esistono molte varianti del tendine del capo lungo del bicipite, ma il loro aspetto non è stato documentato con ecografia (US). Descriviamo un caso di variante anatomica del LHBT visualizzata con risonanza magnetica e confermata con gli US. Inoltre, gli US sono stati utili per escludere l’instabilità del LHBT. Per quanto a nostra conoscenza, questa variante del LHBT non è stata descritta in precedenza con gli US. Considerando che l’ecografia della spalla viene eseguita di routine nella pratica clinica, la conoscenza della variante anatomica del LHBT può essere utile.
Electronic supplementary material
The online version of this article (doi:10.1007/s40477-014-0125-2) contains supplementary material, which is available to authorized users.
Introduction
Many variants of the long head of the biceps tendon (LHBT) exist however the ultrasonographic (US) appearance of these variants is to the best of our knowledge not described. We present a case of a variant LHBT in a patient with multiple shoulder pathologies. This variant tendon is clearly depicted with both US and magnetic resonance imaging (MRI). US was useful over MRI to exclude instability of the LHBT. Considering the pervasiveness of shoulder US in clinical practise, knowledge of the US appearance of variant LHBT may be useful.
Case report
A 56 year old female presented with a chief complaint of chronic, right anterior shoulder pain. A direct MR arthrogram obtained 1 month prior at an outside institution demonstrated acromioclavicular arthritis, partial tearing of the rotator cuff, and tears of both the anterior and posterior labrum. Additionally, the LHBT was separated into three distinct tendon bundles in the region of the intertubercular sulcus (Fig. 1a). At the proximal labral attachment and distal myotendinous junction, the LHBT was one discrete tendon. Sequential axial scanning confirmed the presence of these multiple tendons and excluded the possibility of thickened or variant superior glenohumeral or coracohumeral ligaments. Although this was considered to be an anatomical variant, the stability of the LHBT was a clinical concern. US of the right shoulder was therefore performed for dynamic assessment of the LHBT, acromioclavicular joint, and rotator cuff. During US examination, the presence of multiple tendon bundles of the LHBT was confirmed (Fig. 1b). The LHBT remained stable in the intertubercular sulcus with resisted elbow flexion (Online resource 1). Incidentally, in addition to being arthritic, the acromioclavicular joint was also hypermobile with stress manoeuvres. Rotator cuff pathology was confirmed and there was subacromial impingement with glenohumeral abduction.
Fig. 1.
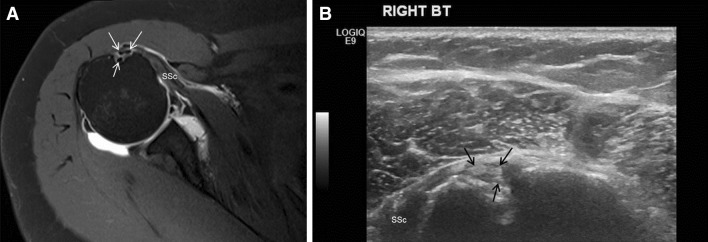
a Axial T1-weighted fat suppressed direct MR arthrogram of the right shoulder demonstrates variant long head biceps tendon anatomy consisting of three tendons within the region of the intertubercular sulcus (white arrows). For reference, the subscapularis muscle (SSc) is seen medially attaching to the lesser tubercle. b Short axis US examination of the shoulder demonstrates the same variant long head biceps tendon anatomy (black arrows) in the intertubercular sulcus. The subscapularis muscle (SSc) is again seen medially
Discussion
In this current case, both MRI and US were able to resolve the patient’s variant LHBT. In addition, US was useful as a dynamic examination to exclude LHBT instability. Considering the increasing role of US in imaging evaluation of the shoulder, understanding of variant anatomy is crucial. To the best of our knowledge, this variant appearance of the LHBT has not been previously described in the ultrasound literature. Variant intra- and extra-articular anatomy of the LHBT is well described in the literature. In one study variant intra-articular LHBT anatomy was present in 1.91 % of a retrospective review of 2,976 shoulder arthroscopies [1]. A separate review of 671 shoulder arthroscopies showed a higher prevalence of intra-articular LHBT variant anatomy of 7.4 % [2]. Classification systems for variant intra-articular LHBT anatomy have been proposed [1]. Another cadaveric study using MRI described the origin of an accessory biceps head from the intertubercular sulcus with incorporation distally into the biceps muscle belly [3]. This reported appearance is similar to the current case, except in our case three distinct tendon bundles were visualised within the region of the intertubercular sulcus. Furthermore, results from our imaging demonstrated the incorporation of the tendon distally prior to the myotendinous junction, rather than discrete supernumerary heads. The LHBT may also originate from the rotator cuff, have an extra-articular origin, or be congenitally absent [4–6]. Clinically, there is an association between variant intra-articular LHBT anatomy and other shoulder pathologies, especially labral tears [1, 2]. US has been shown to be both sensitive and specific in the detection of LHBT full thickness tears and subluxation and dislocation [7]. However, US appears to be insensitive in the detection of partial thickness LHBT tears when compared to arthroscopy [7]. Providing that anisotropy is accounted for during examination, this case report suggests that clinicians should feel confident in diagnosing variant LHBT anatomy with US. Additionally, US was useful in this case to exclude instability of the variant LHBT.
Electronic Supplementary Material
Supplementary material 1 Online resource 1: Dynamic evaluation of the LHBT: Notice how the overlying deltoid muscle contracts with resisted elbow and arm flexion. The variant LHBT remains stable in the intertubercular sulcus (WMV 931 kb)
Conflict of interest
The authors declare they have no conflicts of interest to disclose.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). All patients provided written informed consent to enrolment in the study and to the inclusion in this article of information that could potentially lead to their identification.
Human and animal studies
The study was conducted in accordance with all institutional and national guidelines for the care and use of laboratory animals.
References
- 1.Dierickx C, Ceccarelli E, Conti M, Vanlommel J, Castagna A. Variations of the intra-articular portion of the long head of the biceps tendon: a classification of embryologically explained variations. J Should Elb Surg Am Should Elb Surg. 2009;18(4):556–565. doi: 10.1016/j.jse.2009.03.006. [DOI] [PubMed] [Google Scholar]
- 2.Kanatli U, Ozturk BY, Esen E, Bolukbasi S. Intra-articular variations of the long head of the biceps tendon. Knee Surg Sports Traumatol Arthrosc Off J Esska. 2011;19(9):1576–1581. doi: 10.1007/s00167-010-1384-x. [DOI] [PubMed] [Google Scholar]
- 3.Gheno R, Zoner CS, Buck FM, Nico MA, Haghighi P, Trudell DJ, Resnick D. Accessory head of biceps brachii muscle: anatomy, histology, and MRI in cadavers. AJR Am J Roentgenol. 2010;194(1):W80–W83. doi: 10.2214/AJR.09.3158. [DOI] [PubMed] [Google Scholar]
- 4.Kim KC, Rhee KJ, Shin HD. A long head of the biceps tendon confluent with the intra-articular rotator cuff: arthroscopic and MR arthrographic findings. Arch Orthop Trauma Surg. 2009;129(3):311–314. doi: 10.1007/s00402-007-0559-5. [DOI] [PubMed] [Google Scholar]
- 5.Audenaert EA, Barbaix EJ, Van Hoonacker P, Berghs BM. Extraarticular variants of the long head of the biceps brachii: a reminder of embryology. J Should Elb Surg Am Should Elb Surg. 2008;17(1 Suppl):114S–117S. doi: 10.1016/j.jse.2007.06.014. [DOI] [PubMed] [Google Scholar]
- 6.Koplas MC, Winalski CS, Ulmer WH, Jr, Recht M. Bilateral congenital absence of the long head of the biceps tendon. Skeletal Radiol. 2009;38(7):715–719. doi: 10.1007/s00256-009-0688-8. [DOI] [PubMed] [Google Scholar]
- 7.Armstrong A, Teefey SA, Wu T, Clark AM, Middleton WD, Yamaguchi K, Galatz LM. The efficacy of ultrasound in the diagnosis of long head of the biceps tendon pathology. J should elb surg Am Should Elb Surg. 2006;15(1):7–11. doi: 10.1016/j.jse.2005.04.008. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material 1 Online resource 1: Dynamic evaluation of the LHBT: Notice how the overlying deltoid muscle contracts with resisted elbow and arm flexion. The variant LHBT remains stable in the intertubercular sulcus (WMV 931 kb)