

Abstract
Objectives
Incarceration has been linked to increased risk of sexually transmitted infections (STIs). We conducted a census tract-level ecologic analysis to explore the relationship between neighbourhood incarceration rates and chlamydia incidence among adolescent girls and young women under age 25 in San Francisco in 2010 to focus public health efforts in neighbourhoods at risk.
Methods
Female chlamydia cases under age 25 that were reported to the San Francisco Department of Public Health in 2010 were geocoded to census tract and chlamydia incidence was calculated. Addresses of incarcerated individuals were geocoded, and census tract-specific incarceration rates were estimated. American Community Survey data from 2005–2009 provided tract-specific survey estimates of demographic and socioeconomic characteristics of communities to allow for evaluation of potential census tract-level confounders. A Poisson mixed model was used to assess the relationship of census tract-level incarceration rate with chlamydia case rate.
Results
Accounting for spatial dependence in neighbouring regions, there was a positive association between incarceration rates and chlamydia incidence in young women under age 25 in San Francisco, and this association decreased as poverty increased, after controlling for other risk factors in the model.
Conclusions
This ecologic analysis supports the neighbourhood role of incarceration in the risk of chlamydia among young women. These results have important implications for directing limited public health resources to local areas at risk in order to geographically focus prevention interventions and provide improved access to STI services in specific neighbourhoods with high incarceration rates.
Keywords: Chlamydia, Sexually Transmitted Infections, Epidemiology, Adolescents, Women, Incarceration
INTRODUCTION
In the United States, African-American adolescents and young adults bear a disproportionate burden of sexually transmitted infections (STIs).(1–3) This unequal distribution of morbidity is reflected in San Francisco, where in 2010, the reported chlamydia incidence among adolescents under age 21 was 1990.7 per 100,000 population, nearly four times the adult rate. Furthermore, chlamydia rates among African-Americans under age 21 were over 10 times higher than rates among white adolescents. (4) As shown in prior studies, STI morbidity is not randomly distributed geographically (5) and these patterns are seen locally; San Francisco’s southern and central regions, which are historically largely African-American, have consistently demonstrated the highest STI incidence among adolescents in the city. (4)
Largely, research has been focused on individual-level behavioural factors contributing to STI risk, such as condom use, number of sexual partners, and substance use. However, these individual-level factors do not account for the substantial differences in disease burden among diverse age and racial groups. (2) Research efforts have begun to shift toward risk factors within the broader context of sexual network and structural determinants of health. The determinants underlying the disproportionate burden of disease among African-American youth are complex and likely include the underlying high disease prevalence in the community, poverty, low male:female sex ratio, and high rates of incarceration in this population. (6, 7) Multiple studies have identified the strong link between incarceration and increased STI risk among individuals, (8, 9) and between incarceration and increased sexual risk behaviours, including concurrency and multiple sexual partners. (8, 10, 11) Young African-American women with a male sexual partner recently released from jail have been found to have increased risk of acquiring chlamydia. (12) However, the relationship between individual STI risk, individual sexual behaviour, and history of incarceration may not fully describe how community STI prevalence is influenced by census tract-level incarceration rates.
Our study objective was to explore the ecologic association between census tract-level incarceration and chlamydia incidence among female adolescents and young adults in San Francisco, while accounting for spatial dependence in neighbouring census tracts as well as other measures of correlated social disadvantage. Spatial dependence was included in the model to account for geographic clustering of STIs, and to allow for an evaluation of the relationship between incarceration and chlamydia independent of spatial correlation. We hypothesized that incarceration rates after adjusting for other methods of disadvantage, including interaction effects related to selected demographic factors, would be associated with increased chlamydia incidence.
METHODS
Chlamydia
All chlamydia cases diagnosed in San Francisco residents are reportable to the San Francisco Department of Public Health (DPH) per Article 17 of the California Public Health Code; case reports include patient age, gender, gender of sex partners, and residential address. Chlamydia counts for women under age 25 diagnosed in 2010 in San Francisco were obtained from the DPH STI surveillance system and geocoded with MapMarker Plus 14.2 (Pitney Bowes Software Inc. Troy, NY). Chi-square tests were performed to evaluate for potential differences between cases that could be geocoded and those that could not with regard to patient race and age. Once geocoded, aggregated case counts per census tract for chlamydia in females under age 25 were calculated. Population data for each census tract were obtained from the United States 2010 census. (13) Census tract-specific chlamydia incidence among women under age 25 was calculated.
Census Tract-Level Measures
The unit of analysis was the census tract (n=178). Several census tract boundaries changed between 2000 and 2010; however, this analysis was conducted using the 2000 census tract boundaries, given that most of the morbidity and neighbourhood-level data were available within these 2000 census tract boundaries. Updated population counts using 2010 census data were used to populate tracts per the 2000 census tract boundaries. Two census tracts had boundaries change by one or two census block groups between 2000 and 2010; for each of these census tracts, the 2010 population count for the census tract which most closely approximated the year 2000 census tract boundary was used. Sensitivity analyses were conducted with and without these two census tracts and results did not change significantly, thus we included them in our analysis. Five census tracts with fewer than 20 female residents ages 10–24 were excluded from the analysis.
The San Francisco Sheriff’s Department provided the available residential addresses of all individuals in jail custody on four days representing each quarter in 2010 (March 30, June 30, September 30, and December 30, 2010). The date and time of initial processing into jail were provided to allow for identification of duplicates. Initially, 6,256 addresses were received. There were 1,152 (18.4%) addresses located outside San Francisco; these were excluded from the analysis. An additional 1,479 (23.6%) entries that had the same address, date, and time were excluded, as they likely represented the same individual in jail over the course of those four dates. There were 3,625 (57.9%) addresses with a distinct date and time per address. Of these, 3,385 (54.1% of all addresses received and 93.4% of addresses with a unique date and time) were geocoded to San Francisco census tracts. The census tract-specific incarceration count was then divided by the total population per tract, creating a proxy for incarceration rates based on available data from those four dates in 2010. For confidentiality reasons, we did not obtain any information about the incarcerated individuals other than address, and thus we were unable to evaluate for bias due to potential differences between individuals with addresses that were geocoded and those that were not.
The U.S. Census Bureau American Community Survey (ACS) from 2005–2009 was used to estimate the following census tract-level measures: proportion of residents who are African-American, proportion of residents with income below poverty level in the past 12 months, proportion of housing units which are vacant, proportion of households that received food stamps/Supplemental Nutrition Assistance Programme in the past 12 months, and proportion of households with a female head of household. The proportion of households with a female head of household was used as a proxy for sex ratio in census tracts.
Statistical Analysis
Pearson correlation was obtained among the variables to examine the crude associations. A generalized linear mixed model (GLMM) with chlamydia count as Poisson response and population data from the 2010 census as offset was used to evaluate the association between census tract-level incarceration rates and chlamydia incidence. The model included the interaction between incarceration rates and poverty adjusting for potential confounders as covariates, and included spatial random effects on census tract levels to account for spatial correlation among contiguous census tracts. In addition, the model allowed for independent variations on census tract level by including an independent random effect to account for any over-dispersion. This model is also as known as the Besag-York-Mollie (BYM) model, (14) which accounts for spatial correlation with aggregated count data. The BYM model is computationally efficient and results in a smooth risk surface and prediction variance that changes mainly as a function of the predicted risk. Accounting for spatial correlation helps to better estimate the standard error of the covariates and therefore reduce the false discovery rate. The analysis was done using Integrated Nested Laplace Approximation (INLA)(15) via Bayesian inference. All analyses were conducted using R (www.r-project.org). Only de-identified aggregated surveillance case report and incarceration data were used for public health programme planning and improvement purposes, and thus this study was considered exempt from human subjects considerations in accordance with the Code of Federal Regulations, Title 45.
RESULTS
In San Francisco, there were 1,298 chlamydia cases in women under age 25 reported to DPH in 2010. The reported chlamydia incidence in women under age 25 was 2,097 cases per 100,000. Among these women, there were 1,085 chlamydia cases geocoded to 152 of 178 census tracts. There were 213 chlamydia cases (16.4%) with missing addresses that could not be geocoded. There were no differences by race between those cases that could be geocoded and those that could not (p-value=0.413). However, cases aged 20–24 years were less likely to be geocoded to a valid address than those 19 and younger (p-value <0.0005). The distributions of incarceration and the other census tract-level factors are described in Table 1, and maps of the chlamydia incidence and incarceration rate estimate in San Francisco by census tract are shown in Figures 1 and 2.
Table 1.
Distributions of incarceration and census tract-level factors in San Francisco census tracts (n=178) in 2010.
| Per census tract | Median | 25th percentile |
75th percentile |
Range |
|---|---|---|---|---|
| Incarceration rate estimate (per 100,000)1 | 191.9 | 93.7 | 418.0 | 0–4282.7 |
| % Income below federal poverty line | 9.1 | 5.9 | 14.9 | 0–41.1 |
| % African-American | 2.6 | 0.8 | 8.4 | 0–72.9 |
| % Female head of household | 6.6 | 3.7 | 12.3 | 0–43.9 |
| % Vacant housing units | 8.1 | 5.0 | 11.6 | 0–37.3 |
| % Households receiving food stamps | 1.6 | 0.4 | 4.0 | 0–32.4 |
Incarceration rate estimates were based on data from four discrete dates (March 30, June 30, September 30, and December 30, 2010). This analysis of incarceration rate estimates was performed for public health evaluation and improvement purposes, and is not an official estimate for the City of San Francisco for 2010.
Figure 1. Clamydia incidence rate among females under age 25 by census tract for San Francisco, 2010.
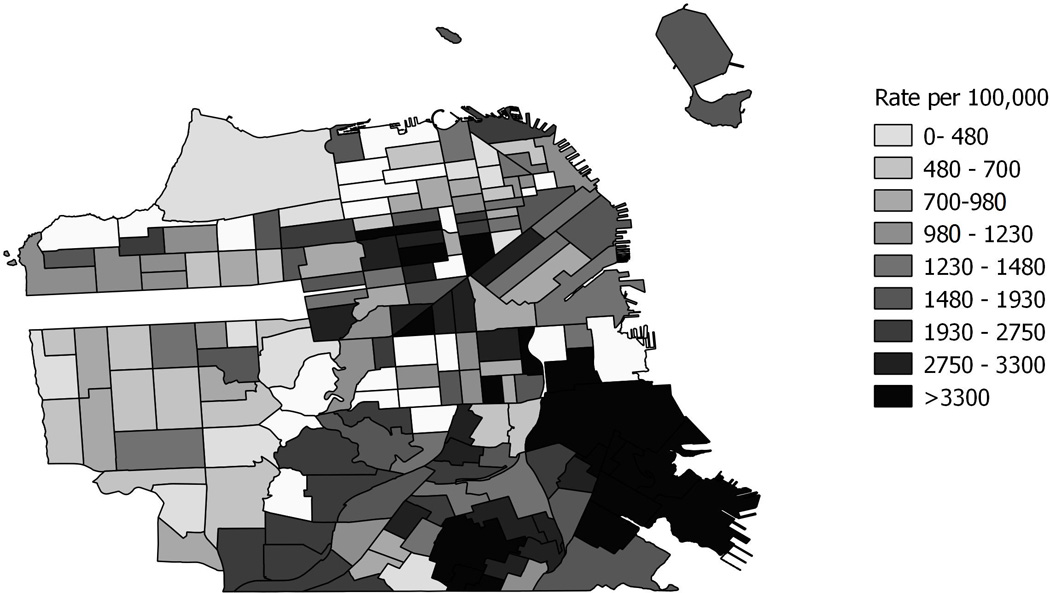
Figure 2. Incarceration rate estimate by census tract for San Francisco, 20101.
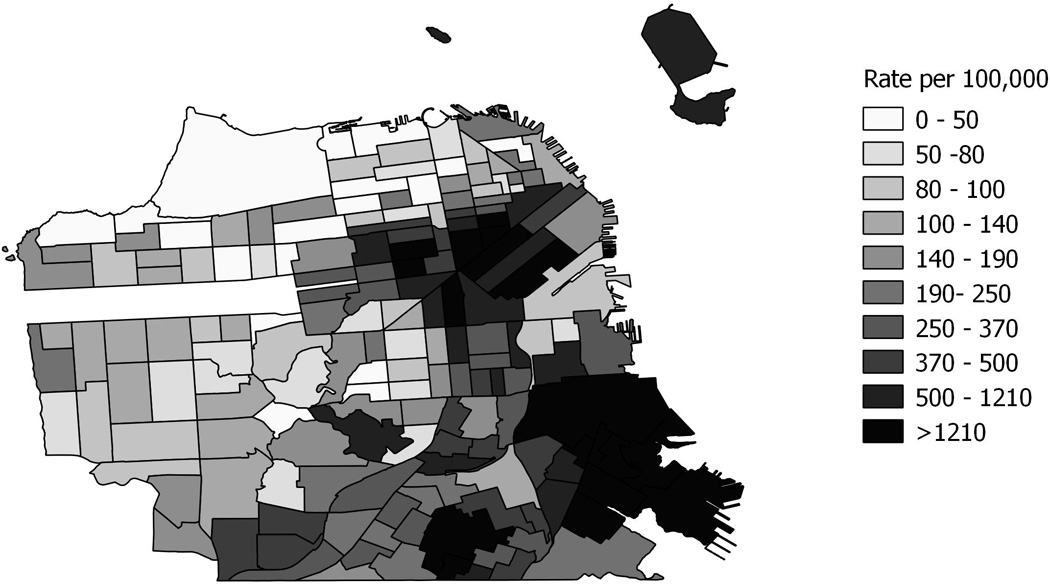
1. Incarceration rate estimates were based on data from four discrete dates (March 30, June 30, September 30, and December 30, 2010). This analysis of incarceration rate estimates was performed for public health evaluation and improvement purposes, and is not an official estimate for the city of San Francisco for 2010.
The correlation of incarceration and the other census-tract level factors were examined. The highest unadjusted correlations were between incarceration rate and proportion African-American (r=0.759), incarceration rate and proportion of households receiving food stamps (r=0.755), and proportion African-American and proportion of households receiving food stamps (r=0.682). The correlation between incarceration rate and proportion below the federal poverty line was 0.411, and the correlation between incarceration rate and chlamydia incidence was 0.586.
Results from the Poisson mixed model are presented in Table 2. The proportion of African-American residents, households with a female head of household, and population with income below poverty level were tested for possible interaction, and poverty was a significant effect modifier for the relationship between incarceration and chlamydia. Considering a baseline in which census tracts were modeled to have no population with income below poverty level, for every 1% increase in the incarceration rate in a census tract, the census tract-level chlamydia incidence is expected to increase by 149% (95% confidence interval 76%–243%) on average among young women under age 25 in San Francisco in 2010, after controlling for the proportion of African-American residents, households with a female head of household, vacant housing units, and households that received food stamps. For every 1% increase in the census tract-level proportion of the population with income below poverty level, this association decreased by 1.8% (95% confidence interval 0.8%–2.9%). When census tracts were modeled to have no incarceration, for every 1% increase in the population with income below poverty level in a census tract, the census tract-level chlamydia incidence increased by 1.8% (95% confidence interval 0.1%–3.6%) on average among women under age 25 in San Francisco, after adjustment for other risk factors in the model. In addition, the proportion of residents who are African-American and the proportion of households with a female head of household in a census tract were also positively associated with chlamydia risk, and the proportion of housing units which are vacant in a census tract was inversely associated with chlamydia risk, on average among young women in San Francisco, adjusting for other risk factors in the model.
Table 2.
Results of Poisson mixed model evaluating association between neighbourhood incarceration and chlamydia counts among adolescent girls and young women under age 25 in San Francisco in 2010.2
| Chlamydia Incidence | ||
|---|---|---|
| Census Tract-Level Covariate | Relative Risk |
95% confidence interval |
| Incarceration rate estimate (per 100,000)3 | 2.489 | 1.764–3.429 |
| % Income below federal poverty line4 | 1.018 | 1.001–1.036 |
| Incarceration rate : poverty interaction term | 0.982 | 0.971–0.992 |
| % African-American | 1.013 | 1.000–1.025 |
| % Female head of household | 1.021 | 1.005–1.039 |
| % Vacant housing units | 0.962 | 0.943–0.981 |
| % Households receiving food stamps | 0.996 | 0.967–1.025 |
Relative risks significant at an alpha=0.05 are bolded.
When modeling no poverty in census tract.
When modeling no incarceration in census tract.
There was a very small amount of variation for both spatial structured random effects 0.25 (95% confidence interval 0.12–0.58) and non-structured random effects 0.00054 (95% confidence interval 0.0001–0.009).
DISCUSSION
In this ecologic analysis, we found that census tract-level incarceration rate estimates were positively associated with increased chlamydia risk among females under age 25 in San Francisco in 2010, after adjusting for spatial dependence. Further, the proportion of the population with income below poverty level was found to be an effect modifier for the relationship between incarceration and chlamydia, and was independently associated with chlamydia risk when census tracts were modeled to have no incarceration. These findings highlight the potential importance of considering not only individual risk behaviours but also area-level factors as interventions are developed to help reduce chlamydia among adolescents and young women.
Our findings are consistent with the established literature linking incarceration with increased STI risk. In 2005, significant correlations were found between county-level incarceration rates and chlamydia and gonorrhoea rates in North Carolina, (16) and a subsequent analysis in Durham County, North Carolina identified an association between census tract incarceration rates and gonorrhoea rates. (17) An ecologic study in Chicago neighbourhoods employed homicide rates as a proxy for incarceration rates, and identified an association with STI rates. (18) Thomas et al has posited several potential mechanisms for the association between incarceration in communities and STIs. First, recently released individuals could bring infection (acquired prior to incarceration and never treated, or acquired while incarcerated) back to the community upon release, resulting in increased STI rates. (16) Next, the effect of incarcerating large numbers of men changes the male:female sex ratio, such that men become more of a commodity, thus shifting power dynamics of sexual relationships and leading women into riskier sexual partnerships. (6, 16,19, 20) Supporting this theory, Green et al found that lower county-level male:female sex ratios were associated with increased risky sexual behaviours among African-American individuals on probation and parole.(21) And last, social disorganization contributes to increased prevalence of infection in neighbourhoods; incarceration is itself a “social force” that leads to disruption of communities. Neighbourhoods experiencing the prolonged absence of many residents while incarcerated or the re-entry of the recently released may be fundamentally different from other communities and lacking in collective efficacy or social capital. (16, 18)
Poverty was found to be an effect modifier for the relationship between incarceration and chlamydia. Although the association between incarceration and chlamydia in a community was large in the model relative to the other covariates, the association decreased as poverty increased in a census tract. This highlights both the independent role of incarceration in chlamydia risk and the cumulative role of multiple structural determinants affecting health outcomes. While significant, high levels of neighbourhood incarceration alone do not explain the disproportionate burden of disease borne by young African-American women in San Francisco. Previous studies have found that after adjusting for sexual behaviour and socioeconomic factors, young African-Americans continue to have greater risk of STIs than teenagers of other races. (22, 23) High background prevalence of disease increases the likelihood of any sexual encounter resulting in infection. (6) In addition, sexual network dynamics have been proposed as a mechanism for increased rates of bacterial STIs in African-American populations, with a comparatively increased number of sexual contacts between individuals with high risk and low risk sexual behaviours in sexual networks, leading to spread of infections throughout networks. (24) Incarceration, poverty, skewed sex ratios, high background prevalence of disease, and other unmeasured network factors all likely contribute to elevated chlamydia rates in these populations.
In an unexpected finding, the proportion of housing units which are vacant in a census tract was inversely associated with chlamydia risk among women under 25. This result counters the theory that vacant households contribute to neighbourhood social disorder and thus would be associated with an increase rather than a decrease in STI rates. One study in Baltimore showed that people living in core gonorrhoea transmission areas lived closer to their sexual partners than individuals from lower gonorrhoea prevalence regions. (25) The reason for our finding is unknown, but similarly it is possible that in San Francisco the population in neighbourhoods with more vacant housing units is less dense, and thus there are fewer people in close proximity and sharing sexual networks.
There are inherent limitations in an ecologic approach in that area-level characteristics cannot be reliably projected onto individuals within the communities examined (the ecologic fallacy). Geocoding to census tracts to estimate neighbourhood incarceration rates was a strength of this analysis, as historically these data have been difficult to obtain, limiting the ability to study the contribution of community incarceration to neighbourhood STI rates. In addition, this analysis accounted for spatial dependence in neighbouring regions, resulting in more accurate estimates of standard error and therefore reduced possibility of making a false discovery.
Additionally, there were data issues that might have impacted the magnitude of the association that we found. We were unable to geocode all cases of chlamydia in San Francisco or all of the addresses of incarcerated individuals. In comparisons of women with chlamydia that could and could not be geocoded there were no differences by race, however women ages 20–24 were less likely to be geocoded than those 19 and younger. We did not have individual-level data available to evaluate for differences among incarcerated individuals, however we have no reason to believe that the lack of data was related to any of the measures examined. The incarceration rates used were estimates based on available residential addresses of all inmates in San Francisco jails on four dates throughout 2010; we were unable to obtain addresses of all incarcerated individuals in San Francisco for the year. By using the addresses of incarcerated individuals on four dates representing each of the four quarters in 2010, we attempted to obtain as representative a sample of the incarcerated population as possible given the resource constraints on obtaining additional data. Also, the ACS provides data on estimates of community characteristics and not actual counts, and these estimates reflected the five years prior to 2010. Last, there is significant variation throughout the world in incarceration practices; the United States has more individuals in prison than any other country. (7) Given the range in incarceration practices worldwide, there may be differences in the relationship between incarceration and STI risk that limit the international generalizability of these results.
Collecting and analyzing incarceration information with STI incidence at a local level may be one way to inform the development of data-guided programmatic efforts to decrease community STI morbidity. As one example of a possible linked STI prevention intervention, observational and modeling studies have suggested that jail-based chlamydia screening might lead to a decrease in community prevalence. (26, 27) Following release, STI screening could be incorporated into probation services for individuals returning to their communities. In addition, health departments could focus the provision of STI services in neighbourhoods with high incarceration rates.
In conclusion, this ecologic analysis supports the community-level role of incarceration in the risk of chlamydia among adolescent girls and young women. More broadly, our findings suggest the importance of multipronged upstream efforts that go beyond the individual to network and community levels to create public health interventions focusing on neighbourhoods with young women at risk. These results have important implications for directing limited public health resources to local regions in order to provide more effective prevention interventions and access to STI services in specific neighbourhoods, rather than across broader geographic regions. In addition, this study identifies neighbourhoods with higher risk where STI prevention and control programmes may be supported by collaboration between local public health departments and correctional partners.
Key messages.
Census tract-level incarceration rates were associated with higher chlamydia incidence among young women in San Francisco, and this association decreased as poverty increased.
Geocoding chlamydia case and incarcerated individual data to census tracts enabled more specific spatial information for assessment of this association.
STI prevention and control measures at the local level may be implemented more effectively by using incarceration data as an additional measure to guide geographically-targeted interventions.
Collaboration between local public health departments and correctional partners in neighbourhoods at risk may result in more effective STI prevention programmes.
Acknowledgments
Funding This work has been supported in part by the US Public Health Service T32 Grant (AI007641-10) and by Comprehensive STD Prevention Projects (1H25PS001354-01) Centers for Disease Control and Prevention.
Footnotes
Competing Interests All co-authors have reviewed and approved this work and have no conflicts of interest. Dr. Susan S. Philip has grants supported by Roche, Cepheid, Abbott Diagnostics, SeraCare Life Sciences, Melinta Therapeutics, and receives royalties from McGraw Hill Textbooks.
Contributors JE Stoltey led data collection, consulted regarding data analysis and interpretation of results, and led the writing. Y Li performed the analysis and interpretation of the data. KT Bernstein conceived the study, supervised the data analysis and interpretation, and assisted with writing and reviewing the manuscript. SS Philip conceived the study, provided critical review of the manuscript, and supervised the study.
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be published in STI and any other BMJPGL products and sub-licences such use and exploit all subsidiary rights, as set out in our licence http://group.bmj.com/products/journals/instructions-for-authors/licence-forms.
REFERENCES
- 1.Miller WC, Ford CA, Morris M, Handcock MS, Schmitz JL, Hobbs MM, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004 May 12;291(18):2229–2236. doi: 10.1001/jama.291.18.2229. [DOI] [PubMed] [Google Scholar]
- 2.Newman LM, Berman SM. Epidemiology of STD disparities in African American communities. Sex Transm Dis. 2008 Dec;35(12 Suppl):S4–S12. doi: 10.1097/OLQ.0b013e31818eb90e. [DOI] [PubMed] [Google Scholar]
- 3.Centers for Disease Control and Prevention | National Center for HIV/AIDS Viral Hepatitis STD and TB Prevention | Division of STD Prevention. Atlanta: 2010. [cited 2012 February 6, 2012]. STD Trends in the United States: 2010 National Data for Gonorrhea, Chlamydia, and Syphilis. [updated November 22, 2010]; Available from: http://www.cdc.gov/std/stats10/tables/trends-table.htm. [Google Scholar]
- 4.STD Control Section. San Francisco, California: San Francisco Department of Public Health; 2011. Sep, San Francisco Sexually Transmitted Disease Annual Summary, 2010. 2011. [Google Scholar]
- 5.Sullivan AB, Gesink DC, Brown P, Zhou L, Kaufman JS, Fitch M, et al. Are neighborhood sociocultural factors influencing the spatial pattern of gonorrhea in North Carolina? Ann Epidemiol. 2011 Apr;21(4):245–252. doi: 10.1016/j.annepidem.2010.11.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aral SO, Adimora AA, Fenton KA. Understanding and responding to disparities in HIV and other sexually transmitted infections in African Americans. Lancet. 2008 Jul 26;372(9635):337–340. doi: 10.1016/S0140-6736(08)61118-6. [DOI] [PubMed] [Google Scholar]
- 7.Walmsley R. World Prison Population List. 10th edition. London: International Centre for Prison Studies; 2013. [cited 2014 October, 1, 2014]. [updated November 21, 2013;]; Available from: http://www.prisonstudies.org/sites/prisonstudies.org/files/resources/downloads/wppl_10.pdf. [Google Scholar]
- 8.Rogers SM, Khan MR, Tan S, Turner CF, Miller WC, Erbelding E. Incarceration, high-risk sexual partnerships and sexually transmitted infections in an urban population. Sex Transm Infect. 2012 Feb;88(1):63–68. doi: 10.1136/sextrans-2011-050280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Joesoef MR, Kahn RH, Weinstock HS. Sexually transmitted diseases in incarcerated adolescents. Curr Opin Infect Dis. 2006 Feb;19(1):44–48. doi: 10.1097/01.qco.0000199020.58075.1a. [DOI] [PubMed] [Google Scholar]
- 10.Epstein H, Morris M. Concurrent partnerships and HIV: an inconvenient truth. J Int AIDS Soc. 2011;14:13. doi: 10.1186/1758-2652-14-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Khan MR, Behrend L, Adimora AA, Weir SS, Tisdale C, Wohl DA. Dissolution of primary intimate relationships during incarceration and associations with post-release STI/HIV risk behavior in a Southeastern city. Sex Transm Dis. 2011 Jan;38(1):43–47. doi: 10.1097/OLQ.0b013e3181e969d0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Swartzendruber A, Brown JL, Sales JM, Murray CC, DiClemente RJ. Sexually transmitted infections, sexual risk behavior, and intimate partner violence among African American adolescent females with a male sex partner recently released from incarceration. J Adolesc Health. 2012 Aug;51(2):156–163. doi: 10.1016/j.jadohealth.2011.11.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bureau of the Census | U.S. Department of Commerce. Census 2010 Summary File 1, Table P12. California: 2010. [Google Scholar]
- 14.Besag J, York J, Mollié A. Bayesian image restoration, with two applications in spatial statistics. Annals of the Institute of Statistical Mathematics. 1991;43(1):1–20. [Google Scholar]
- 15.Rue H, Martino S, Chopin N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations (with discussion) Journal of the Royal Statistical Society, Series B. 2009;71:319–392. [Google Scholar]
- 16.Thomas JC, Sampson LA. High rates of incarceration as a social force associated with community rates of sexually transmitted infection. J Infect Dis. 2005 Feb 1;191(Suppl 1):S55–S60. doi: 10.1086/425278. [DOI] [PubMed] [Google Scholar]
- 17.Thomas JC, Levandowski BA, Isler MR, Torrone E, Wilson G. Incarceration and sexually transmitted infections: a neighborhood perspective. J Urban Health. 2008 Jan;85(1):90–99. doi: 10.1007/s11524-007-9231-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thomas JC, Torrone EA, Browning CR. Neighborhood factors affecting rates of sexually transmitted diseases in Chicago. J Urban Health. 2010 Jan;87(1):102–112. doi: 10.1007/s11524-009-9410-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Thomas JC, Torrone E. Incarceration as forced migration: effects on selected community health outcomes. Am J Public Health. 2006 Oct;96(10):1762–1765. doi: 10.2105/AJPH.2005.081760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pouget ER, Kershaw TS, Niccolai LM, Ickovics JR, Blankenship KM. Associations of sex ratios and male incarceration rates with multiple opposite-sex partners: potential social determinants of HIV/STI transmission. Public Health Rep. 2010 Jul-Aug;125(Suppl 4):70–80. doi: 10.1177/00333549101250S411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Green TC, Pouget ER, Harrington M, Taxman FS, Rhodes AG, O'Connell D, et al. Limiting options: sex ratios, incarceration rates, and sexual risk behavior among people on probation and parole. Sex Transm Dis. 2012 Jun;39(6):424–430. doi: 10.1097/OLQ.0b013e318254c81a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ellen JM, Aral SO, Madger LS. Do differences in sexual behaviors account for the racial/ethnic differences in adolescents' self-reported history of a sexually transmitted disease? Sex Transm Dis. 1998 Mar;25(3):125–129. doi: 10.1097/00007435-199803000-00002. [DOI] [PubMed] [Google Scholar]
- 23.Hallfors DD, Iritani BJ, Miller WC, Bauer DJ. Sexual and drug behavior patterns and HIV and STD racial disparities: the need for new directions. Am J Public Health. 2007 Jan;97(1):125–132. doi: 10.2105/AJPH.2005.075747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Laumann EO, Youm Y. Racial/ethnic group differences in the prevalence of sexually transmitted diseases in the United States: a network explanation. Sex Transm Dis. 1999 May;26(5):250–261. doi: 10.1097/00007435-199905000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Zenilman JM, Ellish N, Fresia A, Glass G. The geography of sexual partnerships in Baltimore: applications of core theory dynamics using a geographic information system. Sex Transm Dis. 1999 Feb;26(2):75–81. doi: 10.1097/00007435-199902000-00002. [DOI] [PubMed] [Google Scholar]
- 26.Barry PM, Kent CK, Scott KC, Goldenson J, Klausner JD. Is jail screening associated with a decrease in Chlamydia positivity among females seeking health services at community clinics?-San francisco, 1997–2004. Sex Transm Dis. 2009 Feb;36(2 Suppl):S22–S28. doi: 10.1097/OLQ.0b013e31815ed7c8. [DOI] [PubMed] [Google Scholar]
- 27.Owusu-Edusei K, Jr, Gift TL, Chesson HW, Kent CK. Investigating the potential public health benefit of jail-based screening and treatment programs for chlamydia. Am J Epidemiol. 2013 Mar 1;177(5):463–473. doi: 10.1093/aje/kws240. [DOI] [PubMed] [Google Scholar]