

Data about persistent pain after breast cancer treatment (PPBCT) after cosmetic or reconstructive breast surgery is limited and focuses on subpectoral implant placement or intercostal nerve injury. We report one patient who presented with bilateral PPBCT and thoracodorsal neuroma after immediate breast reconstruction with the latissimus dorsi myocutaneous flap (LDMF) and subpectoral tissue expander (TEs). This case demonstrates that thoracodorsal neuroma can be a potential cause of post-reconstruction breast pain.
A 65-year-old woman with a history of right breast cancer presented for evaluation of bilateral chronic breast pain following bilateral skin-sparing mastectomy, right axillary lymph node dissection, and bilateral immediate breast reconstruction with the LDMF and TEs 2 years prior. During the initial operation, the thoracodorsal nerves were not divided surgically and the tissue expanders were placed in the subpectoral and sub-latissimus dorsi plane. She had no chemotherapy or radiotherapy. Postoperatively, she developed significant chest wall pain. Five months later, the TEs were removed and exchanged for silicone breast implants. The pain persisted postoperatively and was attributed to bilateral Baker grade 4 capsular contracture. Three months after implant exchange, she underwent a third surgery where bilateral thoracodorsal nerve main trunk transection, capsulotomy, implant exchange and breast fat grafting were performed. Unfortunately, pain relief only lasted 1.5 months. She was evaluated in a chronic pain clinic and had tried numerous conservative measures without success including bilateral intercostal nerve blocks, supportive bras, topical ketamine, and medications, including gabapentin, celecoxib, diazepam, acetaminophen, oxycodone, and lidocaine 5% patch.
At her initial clinical evaluation with us, the patient described breast pain rated at 8/10 on visual analog scale, and spasms located over the anterior lower pole of her breasts which felt like a constricting belt around her chest. Physical examination revealed active LD muscle contraction and involuntary muscle spasms. This prompted us to offer surgical exploration.
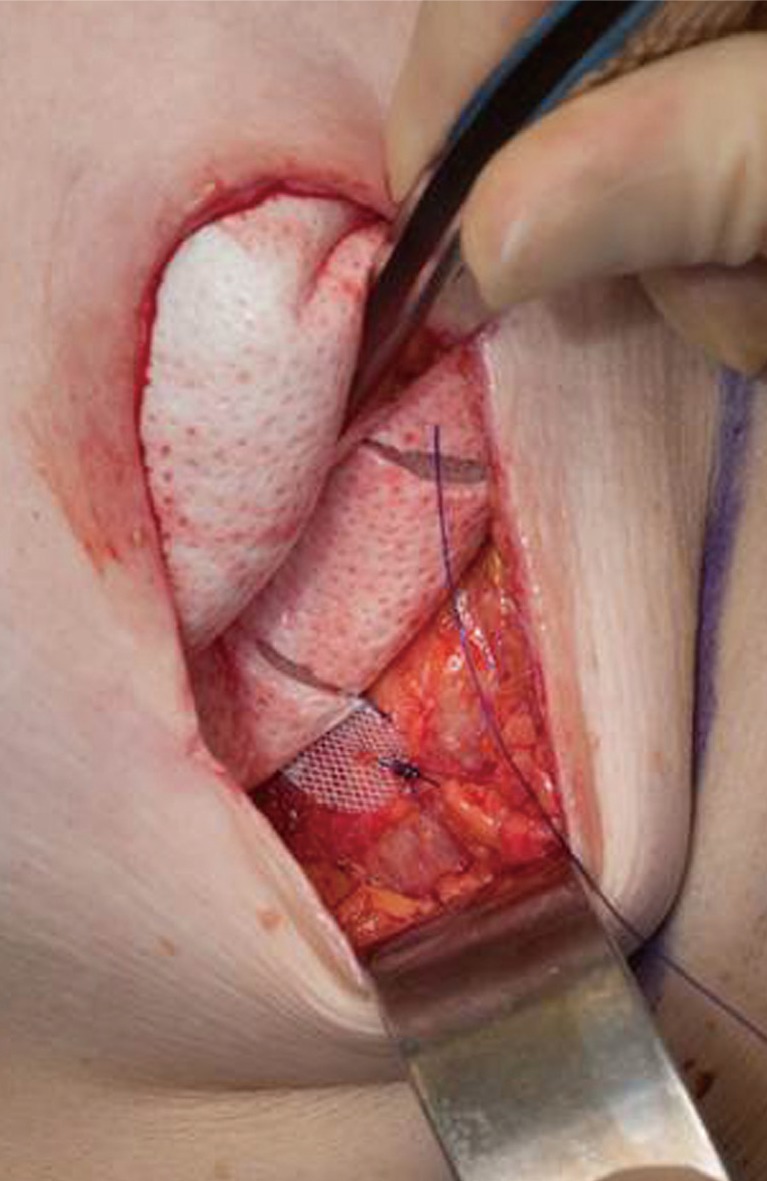
Intraoperatively, bilateral thoracodorsal nerve trunks were found intact, with a visible intraneural mass in both nerves (Fig. 1). The LD muscles were found in the lower pole of both breasts, and were attenuated. Because the patient desired to reduce her breast size in hope of alleviating pain, it was decided to excise the LD myocutaneous flaps by performing a proximal myotomy. A 3 cm segment of thoracodorsal nerve was sent to pathology from each side, and the proximal thoracodorsal nerve stumps were ligated with permanent suture. To minimize the risk of postoperative muscle spasms, the mastectomy defect was recreated, the pectoralis major was repositioned in anatomic position on the chest wall, and TEs were circumferentially wrapped with acellular dermal matrix (Fig. 2) and secured to the chest wall in the subcutaneous plane.
Fig. 1. Bilateral thoracodorsal neuroma: Bilateral thoracodorsal nerves were dissected and isolated. A visible area of enlargement of the proximal thoracodorsal nerve was noticed on both sides, corresponding to the neuroma. (A) Right side. (B) Left side.
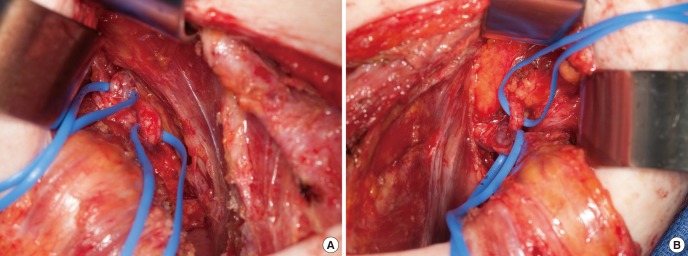
Fig. 2. Tissue expander (TEs) wrapped with acellular dermal matrix: to minimize the risk of postoperative muscle spasms, the mastectomy defect was recreated, the pectoralis major was repositioned in anatomic position on the chest wall, and TEs were circumferentially wrapped with acellular dermal matrix and secured to the chest wall in the subcutaneous plane.
In the early postoperative course, pain was improved bilaterally. Three months later, the patient underwent bilateral removal of TEs and exchange for silicone breast implants. Six months postoperatively, she remained pain free. Histology of bilateral thoracodorsal nerves revealed dense fibrosis consistent with neuroma (Fig. 3).
Fig. 3. Histology of thoracodorsal nerve biopsies: The thoracodorsal nerve biopsies showing haphazardly arranged tangles of variably sized nerve twigs set in a fibrous stroma, characteristic findings of traumatic neuroma. (A) H&E, ×40. (B) H&E, ×100.

PPBCT is a common but poorly understood problem without a clear definition. PPBCT symptoms include altered skin sensations, burning or electric pains, pressure sensations, numbness, aching, and tightening in the breast and axilla.
Development of PPBCT is complex and involves multiple preoperative, intraoperative, and postoperative elements [1]. Cosmetic and reconstructive breast surgery may be associated with persistent breast pain, but relevant research on this topic is rare and focuses on subpectoral implant placement or intercostal nerve injury [2]. Limited data show breast reconstruction with subpectoral implant does not confer increased prevalence of persistent pain [3], but capsule formation, compression of the lateral and medial pectoral nerves and intercostal nerve injury may cause chronic pain [2]. The lateral aspect of the breast is most susceptible to intercostal injury. Nearly 80% of intercostal neuromas were seen in this anatomic location [2].
Our case confirmed the complex and heterogenous presentation of PPBCT. We hypothesize that thoracodorsal neuromas-in-continuity were the initial etiology of pain. This would explain why the pain appeared shortly after the first reconstructive surgery. A neuroma-in-continuity is a neuroma that occurs within an intact nerve resulting from failure of the regenerating nerve growth cone to reach peripheral targets and resulting in a distal portion of the nerve that no longer functions properly [4]. The recurrent pain following the third surgery - where thoracodorsal nerve transection was performed - was most likely caused by the thoracodorsal neuroma and LD muscle reinnervation, which occurred either from incomplete nerve resection or spontaneous neurotization [5]. Mechanical injury during flap dissection or traction could be other possible causes. Meanwhile, capsular contracture, compression of the lateral and medial pectoral nerves under the pectoralis muscle are all additional potential additional causes of pain [2].
Since its first introduction in 1896, use of the LD flap for breast reconstruction has remained popular, but whether and when to cut the thoracodorsal nerve is still controversial. Some authors believe that cutting or saving the nerve does not have an effect on the flap volume or muscle activity in the long run. Thus, both practices seem to be justified [3]. But this case offers new evidence why denervation of thoracodorsal nerve should be performed when harvesting the LD flap: keeping the nerve intact can increase the possibility of voluntary muscle spasm and chronic breast pain. Proximal nerve resection at the axillary apex, with a nerve transection of at least 1 cm, was suggested for a successful denervation [5].
PPBCT has a significant negative effect on quality of life. Non-steroidal anti-inflammatory drugs, benzodiazepines and antidepressants are the most commonly used medications, none of which are very effective. If the pain is caused by the presence of a neuroma, surgical resection can result in complete pain relief. A heightened awareness of the diagnosis and management of neuroma is very important, since this is a treatable cause of pain. When having a consultation about chronic pain after LD breast reconstruction, surgeons should always keep in mind that this is a complex and heterogenous condition for both diagnosis and treatment. Thoracodorsal neuroma should be considered as a possible cause.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 2011;12:725–746. doi: 10.1016/j.jpain.2010.12.005. [DOI] [PubMed] [Google Scholar]
- 2.Ducic I, Seiboth LA, Iorio ML. Chronic postoperative breast pain: danger zones for nerve injuries. Plast Reconstr Surg. 2011;127:41–46. doi: 10.1097/PRS.0b013e3181f9587f. [DOI] [PubMed] [Google Scholar]
- 3.Kaariainen M, Giordano S, Kauhanen S, et al. No need to cut the nerve in LD reconstruction to avoid jumping of the breast: a prospective randomized study. J Plast Reconstr Aesthet Surg. 2014;67:1106–1110. doi: 10.1016/j.bjps.2014.04.029. [DOI] [PubMed] [Google Scholar]
- 4.Mavrogenis AF, Pavlakis K, Stamatoukou A, et al. Current treatment concepts for neuromas-in-continuity. Injury. 2008;39(Suppl 3):S43–S48. doi: 10.1016/j.injury.2008.05.015. [DOI] [PubMed] [Google Scholar]
- 5.Paolini G, Longo B, Laporta R, et al. Permanent latissimus dorsi muscle denervation in breast reconstruction. Ann Plast Surg. 2013;71:639–642. doi: 10.1097/SAP.0b013e31825c0840. [DOI] [PubMed] [Google Scholar]