

Abstract
Parent training (PT) is well understood as an evidence-based treatment for typically developing children with disruptive behavior. Within the field of autism spectrum disorder (ASD), the term parent training has been used to describe a wide range of interventions including care coordination, psychoeducation, treatments for language or social development, as well as programs designed to address maladaptive behaviors. As a result, the meaning of “parent training” in ASD is profoundly uncertain. This paper describes the need to delineate the variants of PT in ASD and offers a coherent taxonomy. Uniform characterization of PT programs can facilitate communication with families, professionals, administrators and third-party payers. Moreover, it may also serve as a framework for comparing and contrasting PT programs. In support of the taxonomy, a purposive sampling of the literature is presented to illustrate the range of parent training interventions in ASD.
Keywords: autism spectrum disorder, parent training, parent-mediated intervention, Psychoeducation, care coordination
In child mental health services, the term “parent training” is synonymous with parent-focused, evidence-based treatment for typically developing children with disruptive behavior. The efficacy of parent training in treating disruptive behaviors in children from preschool to adolescence is supported by decades of research (Dretzke, et al., 2009; Michelson, Davenport, Dretzke, Barlow, & Day, 2013) and clinicians can choose from one of several well-established, structured programs, including Webster Stratton’s Incredible Years (www.incredibleyears.com), Kazdin’s Parent Training (Kazdin, 2005), Barkley’s Defiant Children (Barkley, 2013), and Eyberg’s Parent-Child Interaction Therapy (McNeil & Hembree-Kigin, 2011).
In contrast, within the field of autism spectrum disorder (ASD), the term “parent training” is attached to a variety of treatments that may or may not share common features. This ambiguous application of the term “parent training” may be due to the complexity of ASD and the multiple targets of intervention including skill deficits in communication, socialization, imitation, play and adaptive skills as well as disruptive behavior. Thus, although the term “parent training” is a clear and succinct label for describing an empirically supported treatment for typically developing children with disruptive behavior, the use of this term within the ASD field calls for clarification.
The broad application of parent training in ASD is readily illustrated by a literature search. The terms: “parent training” and “autism” identify articles where authors use labels such as “parent training” (Aman et al., 2009; Bearss et al., 2013b; Beaudoin, Sebire & Couture, 2014; Coolican, Smith, & Bryson, 2010; Drew et al., 2002; Ingersoll & Dvortcsak, 2006; Matson, Mahan, & Matson, 2009; Oosterling et al., 2010; Solomon, Necheles, Ferch, & Bruckman, 2007), “parent education” (Schultz, Schmidt & Stichter, 2011; Stahmer & Gist, 2001; Steiner, et al., 2012; Symon, 2001), “parent-implemented” (Ingersoll & Gergans, 2007; McConachie & Diggle, 2007; Nunes & Hanline, 2007; Reagon & Higbee, 2009; Tarbox, Schiff, & Najdowski, 2010), “parent-mediated” (Diggle, McConachie, & Randle, 2003; Green et al., 2020; Ingersoll & Wainer, 2013; Oono, Honey, & McConahie, 2013; Schertz & Odom, 2007; Siller, Hutman, & Sigman, 2013), and “caregiver-mediated” (Kasari et al., 2010; Kasari et al., 2014). These programs represent a stunning range of intervention formats and treatment targets, including language skills, social skills, psychoeducation, and treatment of disruptive behaviors.
Given this broad application of the label “parent training” in ASD, it is not surprising that clinicians (even those well-versed in ASD) offer differing definitions. This dilemma of confusion around the labeling is not just an academic issue – it has clinical implications for how to discuss treatments with families. Moreover, in the absence of clarity about what is meant by “parent training,” communication about the rationale and content of parent training with clinic administrators, funding agencies, insurance companies, and policy makers is likely to result in confusion or misunderstanding. Thus, given the ambiguities of terminology used to describe parenting programs in ASD, clarification is overdue. To this end, this paper offers a taxonomy for parent training programs for children with ASD (see Figure 1).
Figure 1.
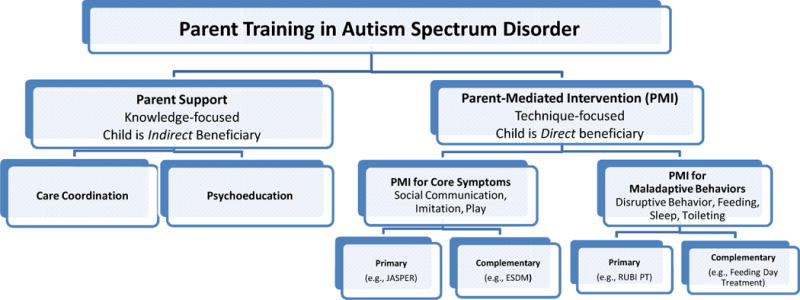
Taxonomy of Parent Training in Autism Spectrum Disorder
Parent Training – Characterizing the Label
An initial way to distinguish parent training programs is to take note of whether the program is designed to provide parental support and promote knowledge gains around the child’s ASD diagnosis versus a program that is designed to actively engage the parent in promoting skill acquisition or behavior change in the child. Figure 1 proposes two broad categories to reflect these differences in programs that invoke the label parent training: Parent Support and Parent Mediated-Intervention (PMI). This initial classification schema is then broadened to include programs within four main categories: Care Coordination, Psychoeducation, Parent-Mediated Interventions for Core Symptoms, and Parent-Mediated Interventions for Maladaptive Behaviors, which will be further described below. Each of the interventions shown in Figure 1 has a tradition and a history. Moreover, these interventions have varying levels of research support from case reports, through rigorous single-subject design and, rarely, randomized controlled trials with structured interventions.
Interventions that involve some form of parent training can be further characterized by considering the program’s format, intensity, location, duration, and target age (Beauodoin, Sebire, & Couture, 2014; Oono, Honey & McConachie, 2013; Schultz, Schmide & Stichter, 2011; Steiner et al., 2012). Format refers to how information is presented to the parent. Self-guided material is available on line or in self-help books. Alternatively, therapist-guided programs may be offered in groups or one-to-one. The most common and most complex format involves therapist-guided parental coaching during parent-child interactions (Schultz et al., 2011). Parent training programs may also range from low to high intensity. Low intensity programs may include brief consultation with a care coordinator or bi-monthly meetings with a therapist. Other more intensive programs may include 60 to 90 minute weekly outpatient or in-home sessions (Bearss, Johnson, Handen, Smith & Scahill, 2013; Hardan et al., 2014; Kasari et al., 2014). High intensity programs may involve multiple sessions a week or day treatment (Dawson et al., 2010; Sharp et al, 2009; Wong & Kwan, 2010). In their review of parenting programs for children with ASD, Schultz and colleagues (2011) reported the intensity of treatments ranging from 1–25 hours a week. Location is where the intervention takes place and may include clinic, school, home-based services or in recent years online presentation or delivery via telehealth (Wacker et al., 2013). Duration involves the length of time the parent participates in the treatment. In Oono, Honey, and McConachie’s review (2013) of parent training programs for young children with ASD, duration of services ranged from one week (Neftd, 2010) to two years (Dawson et al., 2010). Finally, programs may focus on specific target age groups (e.g., preschoolers, adolescents). We will present a purposive sampling of the literature to illustrate the range of characteristics in parent training interventions in ASD as well as a summary of available empirical support across the four main categories. For more comprehensive reviews of available PT programs see (Beaudoin, Sebire & Couture, 2014; Oono, Honey & McConachie, 2013; Schultz, Schmidt & Stichter, 2011).
Parent Support
Parent Support encompasses programs intended to provide indirect benefit to the child by supporting the parent as caregiver and increasing parental knowledge about ASD. Parent Support can be categorized as Care Coordination and Psychoeducation.
Care Coordination
The Agency for Healthcare Research and Quality (AHRQ) defines care coordination as: “the deliberate organization of patient care activities between two or more participants involved in a patient’s care to facilitate the appropriate delivery of health care services” (AHRQ, 2014). Given the complex medical and educational requirements of children with ASD, care coordination is an essential element in overall clinical management. Indeed, children with ASD use more health care resources than the general pediatric population (Gurney, McPheeters, & Davis, 2006; Liptak, Stuart, Auinger, 2006). Parental effort required to coordinate multiple services is substantial, which prompts many parents to reduce working hours or to stop working in order to meet service demands (Kogan et al., 2008). For example, in a sample of 2088 families from the 2005–2006 National Survey of Children with Special Health Care Needs, 25% of families reported spending 10 or more hours per week coordinating the child’s care (Kogan et al.). This burden of care could be reduced if access to appropriate services and better integration of available services were available (Parellada et al., 2013).
The goal of care coordination is to connect families to services and to bridge gaps along a care pathway. This often involves assisting parents to navigate the complicated array of medical, behavioral, alternative, educational and medical treatments. Care coordination tends to be a brief and time-limited consultation delivered by a social worker or case manager. State and local agencies may also provide care coordination services. For example, in Pennsylvania, families can register their child with the Office of Developmental Programs to obtain services from a support coordinator who will serve as an advocate and develop an Individual Support Plan (Lubetsky, Handen, Lubetsky, & McGonigle, 2014).
Although there are accepted recommendations for educational and medical services for children with ASD (e.g., National Research Council, 2001; National Standards Report, 2009), empirical support for current models of “care coordination” in ASD is sparse. A major barrier to rigorous testing of care coordination models is the wide range of regional differences in available services. In addition, the services indicated for children with ASD across the range of severity and age, pose a challenge for care coordination. As in many areas in ASD, one size does not fit all.
One model of care coordination for individuals with ASD and their families has been described by Parellada and colleagues (2013). The program, Comprehensive Medical Care for Autism Spectrum Disorders (AMITEA), developed in Spain, aims to provide centralized care for medical, developmental and behavioral problems in individuals with ASD. In this model, the care coordinator facilitates care by organizing appointments for the families, accompanying the family to appointments, and keeping relevant practitioners abreast of the individual’s needs (Parellada et al., 2013).
The program described by Parellada and colleagues is consistent with the concept of the medical home model articulated by the American Academy of Pediatrics (AAP, 2002; Hyman & Johnson, 2012). Medical homes are intended to provide coordinated, accessible, continuous, culturally competent care that includes screening, education, referrals, and follow up for children with ASD (Lubetsky et al, 2014; AAP, 2002; Murphy & Carbone, 2011). Available research findings suggest that care coordination under the rubric of the medical home results in improved health status for children with ASD (Homer et al., 2008) and that participation in a medical home may also reduce costs of medical care (Kogan et al., 2008).
Psychoeducation
Among the most frequently expressed unmet need by parents of children with ASD at the point of the child’s diagnosis is access to quality information about ASD (Hamilton, 2008; Whitaker, 2002). By providing parents with up-to-date information about ASD, effective psychoeducational programs can help parents adjust expectations for the child’s future and advocate for appropriate services. For example, psychoeducation can help parents prepare for the challenges in the development of an Individualized Education Plan (IEP). Parents of newly diagnosed children need guidance about interventions with empirical support, interventions without solid evidence that are promising, as well as interventions that are unfounded and unsafe. Psychoeducation also can also be beneficial as new challenges unfold throughout the child’s lifetime, such as the onset of puberty or transition to independent living.
There are many self-guided psychoeducational resources available to parents, such as Volkmar and Weisner’s (2009) book “A Practical Guide to Autism: What Every Parent, Family Member, and Teacher Needs to Know,” or web-based resources such as the Autism Speaks 100 Day Kit (http://www.autismspeaks.org/family-services/tool-kits/100-day-kit). Informal psychoeducation also occurs as a part of regular clinical practice (e.g., within the primary care or mental health setting). A structured psychoeducational program is likely to be more intensive than care coordination in the number of visits, and can be delivered by case managers, social workers, psychiatric nurse practitioners or psychologists. Structured psychoeducational programs are generally short-term in duration (i.e., 6–12 sessions) and can be conducted in group or individual formats. Group programs have the added value of promoting mutual support and opportunities to share personal experience with other parents (Daley, Singhal, Weisner, Barua & Brezis, 2013; Farmer & Reupert, 2013).
Common outcomes for psychoeducational programs in ASD include increased parental knowledge, enhanced competence in advocating for the child, decreased parental stress and a reduced sense of isolation (Daley et al., 2013; Farmer & Reupert, 2013; Smith, Greenberg & Mailick, 2012; Tonge et al., 2006). Psychoeducation also may include a few sessions on behavioral management strategies or techniques to enhance communication. Given the brief coverage of these topics within a broader psychoeducation program (Farmer & Reupert, 2013; Smith, Greenberg & Mailick, 2012), these few sessions may increase parental knowledge on behavioral techniques, but are unlikely to provide adequate guidance on management of moderate or greater behavioral problems.
Psychoeducation programs are well-established in other psychiatric conditions, such as schizophrenia and bipolar disorder (Colom et al., 2003; Klaus & Fristad, 2005; McFarlane, Dixon, Lukens, & Lucksted, 2003; Miklowitz, et al., 2003). In comparison, research on psychoeducation in ASD is limited. To date, a few pilot studies have examined psychoeducation as a stand-alone intervention for ASD (Daley et al., 2013; Farmer & Reupert, 2013; Smith, Greenberg, & Mailick, 2012) or as a ‘control’ condition (Bearss et al, in preparation; Hardan et al., 2014; Tonge et al., 2006; 2014).
Smith, Greenberg & Mailick (2012) describe a structured parent psychoeducational program, entitled Transitioning Together, in their pilot study of parents of 10 adolescents with ASD. The 10-session program included two individual family sessions focused on goal-setting for the adolescent. These sessions were followed by eight multifamily group sessions that covered a range of topics including the developmental course of ASD, negotiation of service systems, exploration of behavioral management strategies, advocacy, parental well-being, and long-term planning for the adolescent. The study provided encouraging results on parental understanding of the child’s disability and service system as well as improvements in the parent-child relationship (Smith, Greenberg & Mailick, 2012).
Parent-Mediated Interventions
Parent-mediated interventions are technique-focused where the parent is the agent of change and the child is the direct beneficiary of treatment. As shown in Figure 1, parent-mediated interventions may focus on the treatment of core features of ASD or maladaptive behaviors. These broad categories (core features or maladaptive behaviors) involve the parent as the ‘mediator’ of intervention.
Programs that fall within Parent-Mediated Interventions may be further divided into primary or complementary interventions. This distinction is based upon whether the parent is the primary change agent or a team member in a therapist-led intervention. Specifically, primary programs actively engage the parent from the outset in order for the parent to facilitate the child’s acquisition of specific skills (e.g., joint attention; Kasari et al., 2014) or the reduction of the child’s maladaptive behaviors (Bearss et al, 2013a). In complementary programs, treatment primarily or initially involves the child working with a therapist. Parental coaching is used to promote application of techniques from therapist to parent (e.g., Early Start Denver Model; Dawson et al., 2010) or from clinic into the home and community (e.g., Marcus Autism Center Feeding Program; Sharp et al., 2009). Although this distinction is useful for classifying interventions, hybrid programs have emerged in which interventions initially designed as complementary have expanded to include primary programs (e.g., ESDM, Rogers et al., 2012).
Parent-Mediated Intervention (PMI) for Core Symptoms
PMI’s related to core symptoms include treatments that focus on teaching parents how to promote social interaction, communication, imitation and play skills. Although there are self-guided PMI resources for parents (e.g., Teaching social communication to children with autism: A manual for parents (Ingersoll and Dvortcsak (2010); More than words: A parent’s guide to building interaction and language skills for children with autism spectrum disorder or social communication difficulties (Sussman, 2012), most PMI programs for core symptoms involve therapist coaching of the parent-child dyad (Oono, Honey, & McConachie, 2013; Schultz et al., 2011). PMIs can be delivered in the home and community settings. These locations may be preferred because interactions and skill acquisition occur in a naturalistic setting (Carter, 2011; Dawson, 2010; Drew, 2002; Roberts, 2011; Siller et al., 2013; Smith, Groen & Wynn, 2000). Most programs run two to three hours per session, but the frequency ranges widely from twice daily to monthly (Oono, Honey, & McConachie, 2013). Duration varies as well. Although many structured PMIs targeting core symptoms are over one year in length (Casenhiser, Shanker & Stieben, 2013; Dawson et al., 2010; Drew et al., 2002; Green et al, 2010; Roberts et al., 2011), a handful of programs teach skills to parents within one to two weeks (Nefdt et al., 2010; Wong & Kwan, 2010). PMIs can be delivered by a variety of professionals including special educators, speech pathologists, psychologists and Board Certified Behavior Analysts.
Currently, most parenting interventions in ASD focus on core features, such as socialization and communication or imitation skills (Carter et al., 2011; Drew et al., 2002; Green et al., 2010; Hardan et al., 2014; Ingersoll & Gergans, 2007; Kasari et al., 2010, 2014; Oosterling et al., 2010; Rogers et al., 2012). For example, in Schultz, Schmit & Stichter’s (2011) review, nearly half of the 30 parent training studies identified focused on communication as the primary target for intervention. In Beaudoin and colleagues (2014) review on parenting interventions for toddlers with ASD, communication was a main goal in all 15 included studies. Finally, in the Cochrane review on PMIs for young children with ASD, over 75% of the identified studies targeted core symptoms of ASD (Oono, Honey, & McConachie, 2013). This is also, undoubtedly the most advanced area of research, with a growing number of well-designed randomized clinical trials (RCTs). For example, the Cochrane review identified 13 RCTs targeting core symptoms of ASD (Oono, Honey, & McConachie, 2013), with sample sizes ranging from 17 (Wong & Kwan, 2010) to 152 (Green et al., 2010).
Primary PMI for core symptoms
The intervention developed by Kasari and colleagues (2014) targeting social communication skills in disadvantaged preschoolers (2 to 5 years) is an example of a primary PMI for core symptoms of ASD. The intervention, delivered in the home, includes two 1-hour sessions per week for 12 weeks. Using a structured intervention called Joint Attention Symbolic Play Engagement and Regulation (JASPER), therapists coached parents on how to cultivate engagement with the child during play and ‘every day activities’ (e.g., chores, grooming). The active coaching aims to promote joint attention, play skills, and language. In a parallel group design, 112 children were randomly assigned to this individual caregiver-mediated intervention or a small group caregiver education program (children were not present; Kasari et al., 2014). While children in both groups exhibited improved joint engagement and initiation of joint attention after 12 weeks of treatment, greater improvements were noted in the caregiver-mediated group, with gains maintained over time (3 months post-treatment; Kasari et al.).
Complementary PMI for core symptoms
The Early Start Denver Model (ESDM) is an example of a Complementary PMI for core features of ASD (Dawson et al., 2010). This comprehensive, primarily child-focused intervention for children age 12 to 48 months involves therapist-led treatment 20 hours per week (e.g., 4 hours per day, 5 days/week) for two years in the home. The treatment also includes twice monthly parent consultation during which the principles and specific techniques of ESDM are taught to parents. Parents are then encouraged to apply ESDM strategies during everyday activities such as feeding, bath time, and play. ESDM integrates developmental and relationship-based approaches with techniques from applied behavior analysis (ABA) to promote interpersonal exchange and shared engagement with real-life activities in the child. It also promotes parental sensitivity to the child’s cues and verbal and nonverbal communication. In a study of 48 children, age 18 to 30 months, subjects were randomized to either ESDM or treatment as usual (community-based intervention) for two years. In the ESDM group, therapists averaged 15 hours of direct care per week and parents reported spending an average of 16 hours per week using ESDM strategies. By contrast, the treatment as usual group reported an average of 18 hours per week of services (9 hours of individual therapy, 9 hours of group intervention). After the first year of treatment, there were minimal differences between groups. After two years of treatment, however, the ESDM group showed significant improvements on measures of communication compared to the treatment as usual group. The differences between the gains in the ESDM group were accentuated by the lower scores on standardized measures of IQ and functional communication in the treatment as usual group (Dawson et al.)
Parent-Mediated Intervention for Maladaptive Behavior
In addition to core features of ASD, clinically significant disruptive behavior problems are common and may include tantrums, aggression, noncompliance with routine demands, self-injury, property destruction and hyperactivity (Hartley, Sikora, & McCoy, 2008; Kaat & Lecavalier, 2013) as well as more focal concerns such as food refusal (Sharp et al, 2013), sleep disturbance (Hoffman, Sweeney, Gilliam, & Lopez-Wagner, 2006; Johnson, et al., 2014;), toileting problems (Maskey, Warnell, Parr, Couteur, & McConachie, 2013; Simonoff et al., 2008) and elopement (Anderson, et al., 2012). These maladaptive behaviors may interfere with a child’s response to educational intervention, lead to further isolation from peers, and increase caregiver stress due to disruptions in daily activities (Brereton, Tonge, & Einfeld, 2006; Hartley, Sikora, & McCoy, 2008; Herring et al., 2006; Simonoff et al., 2008; Symon, 2005; Tonge et al, 2006). Children with ASD with disruptive behavior who actively resist acquiring new skills or performing already acquired skills will likely fall behind in adaptive functioning. Indeed, on measures of adaptive functioning, children with ASD are often a full standard deviation below their assessed cognitive ability (Kanne et al., 2011; Perry, Flanagan, Dunn Geier & Freeman, 2009). This connection between disruptive behavior and impaired adaptive functioning provides a compelling rationale for PMIs designed to reduce the child’s behavioral problems and improve daily living skills.
Self-guided resources such as No More Meltdowns (Baker, 2008); Understanding Why Problem Behaviors Occur (Frea, Koegel, & Koegel, 1994); Toilet Training in Children with Severe Handicaps (Dunlap, Koegel, & Koegel, 1984) are available for clinicians and parents. As principles of applied behavior analysis (ABA) are commonly used in the treatment of disruptive behavior and focal problems in children with ASD, programs tend to be highly individualized, time-limited, and target problem-specific, with varying degrees of parental involvement (Odom, Boyd, Hall, & Hume, 2010; Odom et al., 2003). ABA emphasizes live observation, determining a functional relationship via experimental control, careful manipulation of environmental stimuli, and in-vivo treatment (Odom et al., 2003). As a result, while many programs involve therapist-child or parent-dyad coaching by the therapist, the intensity and duration of programs vary. These targeted interventions, such as feeding intervention, are delivered most commonly by behaviorally trained therapists (Sharp, Burrell, & Jaquess, 2013).
Until recently, most studies on training parents to reduce disruptive behavior have used single-subject designs (Anderson & McMillan, 2001; Ducharme & Drain, 2004; Moes & Frea, 2002; Wahler, Vigilante, & Strand, 2004). These studies offer proof of concept for specific PMI techniques for children with ASD and maladaptive behavior. However, the individualized approach and lack of a structured manual hinder replication (Smith et al., 2007). In addition, study samples were often inadequately characterized making generalization difficult. More recently, a handful of open prospective case series (Bearss et al., 2013a; Brookman-Frazee, Drahota & Stadnick, 2012; RUPP, 2007; Wacker et al., 2013) and quasi-experimental trials (Tonge et al., 2014) using a structured manual have been published. Two randomized clinical trials (RCTs) (Sofronoff, Leslie, & Brown, 2004; Whittingham, Sofronoff, Sheffield, & Sanders, 2009) have been published to date. Sofronoff, Leslie & Brown (2004) compared a one-day workshop (n=18) and 6-session individual parent training program (n=18) to waitlist control (n=15) in children with Aspergers age 6 to 12. Whittingham and colleagues (2009) randomized children with ASD (age 2 to 9) to the Stepping Stones Triple P parent training program (n=29) or a wait-list control (n=30). Both studies showed significant reductions of parent-reported child behavior problems for the parent training programs compared to waitlist, with the Sofronoff study (2004) exhibiting superiority of the individual format when compared to workshops (Sofronoff et al.). Behavioral improvements were maintained at the 3-month (Sofronoff et al.) and 6-month (Whittingham et al., 2009) follow-up. The Cochrane review (2013) of programs for children six and under otherwise determined that no study conclusively identified a significant reduction in maladaptive behavior in favor of the parent training intervention group.
Primary PMI for disruptive behavior
The Research Units in Pediatric Psychopharmacology (RUPP) Autism Network parent training program (Aman, et al., 2009; Bearss et al., 2013a; Bearss et al, 2013b; Johnson et al, 2007; RUPP, 2007; Scahill et al., 2012;) illustrates a Primary PMI program for the reduction in disruptive behavior and improvement in adaptive skills in young children with ASD. The program consists of 11 core and up to two optional focal-problem sessions (e.g., toileting or sleep problems) as well as two telephone booster calls and two home visits delivered over the course of six months. The intervention is based on the principles and techniques of applied behavior analysis. In this model, disruptive, noncompliant, and aggressive behaviors serve a function for the child. The function may be access to a tangible item (certain food or preferred toy), attention, escape from a demand or self-stimulatory in nature. The key to changing a behavior is first to identify the function and then modify the situations that precede and the consequences that follow the behavior. Because therapists set out to teach parents how to modify the child’s behavior, parents are the change agents. The program targets daily activities such as getting dressed, getting ready for bed or managing trips to the grocery store that are often daily struggles for families of children with ASD.
The RUPP consortium developed the manual and evaluated the feasibility of the manual in an open prospective study (Johnson et al., 2007; RUPP, 2007). The demonstration of acceptability by parents and the clear evidence that the manual could be delivered reliably by therapists at different sites was followed by a large scale randomized trial of risperidone only versus risperidone plus parent training in 124 school-age children with ASD accompanied by serious behavioral problems (Aman et al, 2009; Scahill et al., 2012). Bearss et al. (2013a) subsequently modified the RUPP manual as a stand-alone treatment for younger children between the ages of 3 and 6 years. With funding from the National Institute of Mental Health (NIMH), the multisite consortium has completed a randomized trial of this parent training program compared to parent psychoeducation in 180 preschool-age children with ASD plus disruptive behavior (Bearss et al., manuscript in preparation).
Complementary PMI for disruptive behavior
The intensive day treatment feeding program at the Marcus Autism Center is a model of a complementary PMI for maladaptive behavior in the form of extreme food refusal and food selectivity in children with ASD (Sharp, Jaquess, Morton, & Miles, 2009). The intervention involves four, 45-minute meals presented each day, five days a week for eight weeks. An individual treatment protocol is developed for each child using common behavioral intervention components such as stimulus fading (e.g., gradual increase of bite size), escape extinction (no longer allowing disruptive behaviors to serve as an escape from meal demand) and positive reinforcement (Sharp et al., 2009). While caregivers are involved in the selection of foods in the treatment and they observe the intervention, the therapist implements all aspects of the individualized treatment protocol until the child’s short-term feeding goals are met. Once these goals are met, the therapist conducts in-vivo parent-child coaching to promote reliable application of the interventions developed and implemented by the therapist. Once trained, parents implement the intervention in the home. Sharp and colleagues (2009) conducted a retrospective chart review of 13 children with ASD ages 2 to 7 who participated in the feeding day program. Length of treatment ranged from 29 to 46 days with preliminary results supporting the utility of the program in decreasing food refusal and expanding the variety of foods consumed (Sharp et al., 2009). Additionally, gains in appropriate mealtime behaviors continued once caregivers transitioned into the role of primary feeder and were maintained more than one year after discharge (Sharp et al., 2009).
Discussion
Parent training for typically developing children with disruptive behavior is a well-established, evidence-based intervention. The challenges parents face in raising a child with ASD has sparked interest in the application of parent training in this population and as a result, a variety of programs are emerging as effective, with the advantage that they can be administered in various service settings (clinics, primary care, schools, home). They also are emerging against a backdrop of increased recognition that traditional forms of intervention (intensive, school-based) are costly (Solomon, Necheles, Ferch, & Bruckman, 2007) and there is a shortage of trained professionals available to implement the interventions (Brookman-Frazee, Drahota, Stadnick & Palinkas, 2012). Thus, parent training programs can be cost-effective and are needed, especially in areas where specialized services are not otherwise available.
As a product of the wide ranging needs of children with ASD, the term ‘parent training’ and its variants has been applied to programs ranging from care coordination and psychoeducation about ASD to parent-mediated interventions for core symptoms and common co-occurring behavioral problems. In addition, ‘parent training’ may involve the parent as primary agent of change or as an adjunctive component in an intensive child-focused therapy program. Using selective examples, Table 1 illustrates the complexity and range of formats, intensity, location, duration and target age groups found in parent training programs in ASD across the four categories.
Table 1.
Characteristics of Parent Training Programs
| Intervention | Focus | Parent Role | Format & Intensity | Location | Duration | Age |
|---|---|---|---|---|---|---|
|
AMITEA Parallada et al, 2013 |
Parent Support: Care Coordination | — | Continuous coordinated care facilitated by a case manager assigned to the patient | Clinic | Ongoing | Any age |
|
Understanding Autism and Understanding My Child with Autism Farmer and Reupert, 2013 |
Parent Support: Psychoeducation | — | 6 Weekly two-hour sessions in a group format | Clinic | 6 weeks | 66% 2–6 years 34% > 6 years |
|
Transitioning Together Smith, Greenberg, & Mailick, 2014 |
Parent Support: Psychoeducation | — | 10 Weekly 90-minute Sessions: 2 Therapist-Parent sessions 8 Therapist-Parent Group sessions |
Clinic | 10 weeks | 14 – 17 years |
|
Joint Attention Symbolic Play Engagement and Regulation (JASPER) Kasari et al., 2010 |
PMI: Core | Primary | 24 45-minute Sessions 3×/week: 8 Therapist-Parent sessions 16 Parent-child dyad coaching sessions |
Clinic | 8 weeks | 21 – 36 months |
|
Hanen’s More than Words Carter, et al., 2011 |
PMI: Core | Primary | 14 Weekly Sessions: 11 Therapist-Parent Group session 3 Parent-child dyad coaching sessions |
Home and clinic | 14 weeks | 15 – 24 months |
|
Preschool Autism Communication Trial (PACT) Green et al., 2010 |
PMI: Core | Primary | Months 1–6: 18 2-hour bi-weekly Parent-child dyad coaching Months 7–12: 18 2-hour monthly Parent-child dyad coaching |
Clinic | 12 months | 2 – 4 years |
|
P-Early Start Denver Model Rogers et al., 2012 |
PMI: Core | Primary | 1 hour/week of Therapist-Parent Instruction and Parent-child dyad coaching sessions | Clinic | 12 weeks | 12 – 24 months |
|
Early Start Denver Model Dawson et al., 2010 |
PMI: Core | Complementary | 20 hours/week Therapist-child instruction Semi-monthly Therapist-Parent sessions |
Home | 2 years | 18 – 30 months |
|
Pivotal Response Treatment Smith et al., 2010 |
PMI: Core | Complementary | Cohort 1: 15 hours/week therapist-child sessions for 12 months; 1 week of parent training in group workshop with in-vivo parent-child dyad coaching Cohort 2: 15 hours/week for 6 months, 10 hours/week for 3 months, 5 hours/week for 3 months of therapist-child sessions; 1 week of parent training in the home with parent-child dyad in-vivo coaching |
Home/school | 12 months | 2 – 6 years |
|
Preschoolers with Autism Tonge et al., 2014 |
PMI: Core | Primary | 10 90-minute Therapist-Parent group sessions 10 60-minute Therapist-Parent sessions |
Clinic | 20 weeks | 2.5 – 5 years |
|
RUBI Parent Training Bearss et al., 2013a |
PMI: Maladaptive | Primary | Up to 13 weekly 60–90 parent sessions; minute therapist-2 home visits; 2 phone sessions | Clinic/home/phone | 6 months | 3 – 6 years |
|
Marcus Autism Center Feeding Day Treatment Program Sharp et al., 2009 |
PMI: Maladaptive | Complementary | 4 sessions/day for 39 days of Therapist–led sessions. Parent-child dyad coaching introduced to generalize skills learned via therapist-child intervention |
Clinic | 8 weeks | 2–7 years |
Not surprisingly, the multiple applications of the term ‘parent training’ for children with ASD has promulgated confusion among professionals, parents, administrators and third-party payers on the meaning of the term. To address this problem, we propose a taxonomy with two broad categories –parent support programs and parent mediated interventions – to delineate parent training programs. These broad categories can be further divided into care coordination, psychoeducation (under parent support programs) and parent-meditated interventions for core symptoms or for maladaptive behaviors. This taxonomy reflects the diversity of parent support programs and parent mediated interventions for children with ASD and it also provides a basis for uniform characterization of programs. This allows placement of a given intervention into the broader treatment landscape. Moving forward, this taxonomy may also guide labeling of specific types of similar programs within the taxonomy. For example, within “PMI for core symptoms”, Naturalistic Developmental Behavioral Intervention (NDBI) is an emerging label that is being used to characterize a cluster of early interventions (e.g., JASPER, ESDM, Pivotal Response Treatment (PRT) that address deficits in communication and cognition at early developmental stages.
Outside of breeding familiarity via brand names (e.g., NDBI, JASPER, ESDM, PRT), the diverse nature of programs involving parents requires the field to avoid the use of concise labels as they may not provide enough information about program content. This, in turn, places the onus on researchers and clinicians to describe the format, focus, and content of any one program and to facilitate communication amongst professionals. In practical terms, this implies that saying a program is a “PMI” is insufficient, as a distinction needs to be made, for example, between a “PMI for communication” versus a “PMI for imitation skills.” Although this expanded description may seem unnecessary or burdensome, it may be especially useful to insurance companies, policy-makers, and clinic administrators who are not familiar with the similarities and differences across various programs but nevertheless play an important role in determining program viability. Moreover, parents, who are the primary consumer of these services, are often inundated with information and may be overwhelmed by treatment choices. Clear descriptions will help parents decipher treatment options.
Additional Considerations
The proposed delineation of parent support programs and parent-mediated interventions implies that the resulting four categories are mutually exclusive. When sorting through available evidence, classification of an intervention into one of the four categories is justified and useful for discussion. In clinical settings, however, the demarcation may not be so firm and there may be overlap across the four areas. In some settings, clinicians provide a combination of supportive and skill-based treatments by necessity. Alternatively, there may be programs that are designed primarily to address core symptoms or behavioral issues in children with ASD but may include, as part of the program, sessions on psychoeducation.
Future Directions
Parent-mediated interventions for core symptoms of ASD have been an area of active research. In the recent Cochrane review (Oono, Honey, & McConachie, 2013), improvement in proximal outcomes such as shared attention between parent and child, as well as distal improvements in child language skills and reduction in core features of ASD were noted. Improvements in child social initiations, adaptive skills, maladaptive behaviors, and parent stress, however, were inconclusive. Of the 19 RCTs reviewed, only one study (Green et al, 2010) was deemed adequately powered (Oono, Honey & McConachie, 2013). Thus, although there is a growing body of evidence for PMI focused on core features of ASD, additional research is needed to test existing and new models. In addition, models of care coordination and psychoeducation across the age range also require further development within the field of ASD. As the body of research on PT interventions for ASD continues to develop, the proposed taxonomy may require revision and expansion to incorporate newer programs that gain empirical support. The taxonomy can serve as a guide in the refinement of existing programs and development of new ones in areas for which they are needed.
As the empirical foundation for parent support programs and PMIs expand, there will be concomitant need for dissemination (spreading the word about the evidence-based intervention) and implementation (deliberate steps to incorporate evidence-based treatments into real world settings). Training demands for empirically-supported interventions for children with ASD vary with the complexity of the treatment. For example, parent training for disruptive behavior in young children with ASD is likely to require less training than the JASPER model. Due to the complexity of some interventions, implementation may be selective to centers that have the capacity to adopt more specialized treatments. Finally, expansion of the autism spectrum diagnosis and improved methods of assessment have contributed to an increase in the prevalence of ASD (Elsabbagh et al., 2012). The term ‘autism spectrum’ implies that the affected have a range of treatment needs. Some children may need intensive language intervention; others may need less intensive intervention to transmit effective tools to deal with maladaptive behavior. The challenge for the field is to build the evidence base in order to match the child with the empirically-supported intervention.
Acknowledgments
This publication was made possible by the following grants: the National Institute of Mental Health NIMH R01 MH081148 (principal investigator: L Scahill); Healthcare Innovation Program/Atlanta Clinical & Translational Research Seed Grant Program. This publication was also made possible by a Clinical and Translational Scholar Award (CTSA) Grant Number UL1 RR024139 and 5KL2RR024138 (principal investigator: K Bearss) from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH.
Footnotes
Disclosure of Potential Conflicts of Interest
Dr. Scahill serves as a consultant for Neuren, Coronado, Roche, MedAdvante, and Shire. Dr. Bearss, Burrell and Stewart have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. No writing assistance was utilized in the production of this manuscript.
Contributor Information
Karen Bearss, Marcus Autism Center, Children’s Healthcare of Atlanta and Emory University School of Medicine 1920 Briarcliff Road, NE, Atlanta, GA 30329.
T. Lindsey Burrell, Marcus Autism Center, Children’s Healthcare of Atlanta and Emory University School of Medicine 1920 Briarcliff Road, NE, Atlanta, GA 30329.
Lindsay M. Stewart, Emory University School of Medicine Department of Psychiatry and Behavioral Sciences, 12 Executive Park Dr. NE, Atlanta, GA 30329.
Lawrence Scahill, Marcus Autism Center, Children’s Healthcare of Atlanta and Emory University School of Medicine 1920 Briarcliff Road, NE, Atlanta, GA 30329.
References
- Aman MG, McDougle CJ, Scahill L, Handen B, Arnold LE, Johnson C, Wagner A. Medication and parent training in children with pervasive developmental disorders and serious behavior problems: Results from a randomized clinical trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2009;48:1143–1154. doi: 10.1097/CHI.0b013e3181bfd669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson C, Law JK, Daniels A, Rice C, Mandell DS, Hagopian L, Law PA. Occurrence and family impact of elopement in children with autism spectrum disorders. Pediatrics. 2012;130(5):870–877. doi: 10.1542/peds,2012-0762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson CM, McMillan K. Parental use of escape extinction and differential reinforcement to treat food selectivity. Journal of Applied Behavior Analysis. 2001;34(4):511–515. doi: 10.1901/jaba.2001.34-511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Academy of Pediatrics. The medical home: Medical home initiatives for children with special needs project advisory committee. Pediatrics. 2002;110(1):184–186. [Google Scholar]
- Agency for Healthcare Research and Quality. Care Coordination Measures Atlas Update. Rockville, MD: 2014. Chapter 2. What is Care Coordination? http://www.ahrq.gov/professionals/prevention-chronic-care/improve/coordination/atlas2014/chapter2.html. [Google Scholar]
- Baker J. No more meltdowns: Positive strategies for managing and preventing out-of-control behaviors. Arlington, TX: Future Horizons Inc; 2008. [Google Scholar]
- Barkley R. Defiant children: A clinician’s manual for assessment and parent training. 3. New York, NY: Guilford; 2013. [Google Scholar]
- Bearss K, Johnson C, Handen B, Smith T, Scahill L. A pilot study of parent training in young children with autism spectrum disorders and disruptive behavior. Journal of Autism and Developmental Disorders. 2013a;43:829–840. doi: 10.1007/s10803-012-1624-7. [DOI] [PubMed] [Google Scholar]
- Bearss K, Lecavalier L, Minshawi N, Johnson C, Smith T, Handen B, Scahill L. Toward an exportable parent training program for disruptive behaviors in autism spectrum disorders. Neuropsychiatry. 2013b;3:169–180. doi: 10.2217/npy.13.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beaudoin AJ, Sébire G, Couture M. Parent Training interventions for toddlers with Autism Spectrum Disorder. Autism Research and Treatment. 2014 doi: 10.1155/2014/839890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brereton AV, Tonge BJ, Einfeld SL. Psychopathology in children and adolescents with autism compared to young people with intellectual disability. Journal of Autism and Developmental Disorders. 2006;7:863–870. doi: 10.1007/s10803-006-0125-y. (2006) [DOI] [PubMed] [Google Scholar]
- Brookman-Frazee L, Drahota A, Stadnick N. Training community mental health therapists to deliver a package of evidence-based practice strategies for school-age children with autism spectrum disorders: A pilot study. Journal of Autism and Developmental Disorders. 2012;42:1651–1661. doi: 10.1007/s10803-011-1406-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brookman-Frazee L, Drahota A, Stadnick N, Palinkas LA. Therapist perspectives on community mental health services for children with autism spectrum disorders. Administration and Policy in Mental Health and Mental Health Services Research. 2012;39:365–373. doi: 10.1007/s10488-011-0355-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter AS, Messinger DS, Stone WL, Celimli S, Nahmias AS, Yoder P. A randomised controlled trial of Hanen’s “MoreThan Words” in toddlers with early autism symptoms. Journal of Child Psychology and Psychiatry. 2011;52(7):741–52. doi: 10.1111/j.1469-7610.2011.02395.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casenhiser DM, Shanker SG, Stieben J. Learning through interaction in children with autism: Preliminary data from a social-communication-based intervention. Autism. 2013;17(2):220–241. doi: 10.1177/1362361311422052. [DOI] [PubMed] [Google Scholar]
- Colom F, Vieta E, Martinez-Aran A, Reinares M, Goikolea JM, Benabarre A, Corominas J. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remissions. Archives of General Psychiatry. 2003;60:402–407. doi: 10.1001/archpsyc.60.4.402. [DOI] [PubMed] [Google Scholar]
- Coolican J, Smith IM, Bryson SE. Brief parent training in pivotal response treatment for preschoolers with autism parent training in PRT. Journal of Child Psychology & Psychiatry. 2010;51:1321–1330. doi: 10.1111/j.1269.7610.2010.02326.x. [DOI] [PubMed] [Google Scholar]
- Daley TC, Singhal N, Weisner T, Barua M, Brezis RS. Evaluation of an Acceptance and Empowerment Parent Training Model: Evidence from an Intervention in India. Paper presented as a part of an Integrated Educational Session on Parent Training and Parent Mediated Intervention in Diverse Contexts at the International Meeting for Autism Research; San Sebastian, Spain. 2013. [Google Scholar]
- Dawson G, Rogers S, Munson J, Smith M, Winter J, Greenson J, Varlet J. Randomized, controlled trial of an intervention for toddlers with autism: The early start Denver model. Pediatrics. 2010;125:17–23. doi: 10.1542/peds.2009-0958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diggle T, McConachie HR, Randle VRL. Parent-mediated early intervention for young children with autism spectrum disorder. (Issue 1. Art. No.: CD003496).Cochrane Database of Systematic Reviews. 2003 doi: 10.1002/14651858.CD003496. [DOI] [PubMed] [Google Scholar]
- Drew A, Baird G, Baron-Cohen S, Cox A, Slonims V, Wheelwright S, Charman T. A pilot randomized control trial of a parent training intervention for pre-school children with autism. European Child & Adolescent Psychiatry. 2002;11(6):266–272. doi: 10.1007/s00787-002-0299-6. [DOI] [PubMed] [Google Scholar]
- Dretzke J, Davenport C, Frew E, Barlow J, Stewart-Brown S, Bayliss S, Hyde C. The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomized control trials. Child and Adolescent Psychiatry and Mental Health. 2009;3(7) doi: 10.1186/1753-2000-3-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ducharme JM, Drain TL. Errorless academic compliance training: Improving generalized cooperation with parental requests in children with autism. Journal of the American Academy of Child and Adolescent Psychiatry. 2004;43:163–171. doi: 10.1097/00004583-200402000-00011. [DOI] [PubMed] [Google Scholar]
- Dunlap G, Koegel R, Koegel L. Toilet training for children with severe handicaps: A field manual for coordinating training procedures across multiple community settings. Santa Barbara: University of California, Santa Barbara; 1984. [Google Scholar]
- Elsabbagh M, Divan G, Koh Y, Kim Y, Kauchali S, Marcín C, Fombonne E. Global Prevalence of Autism and Other Pervasive Developmental Disorders. Autism Research. 2012;5:160–179. doi: 10.1002/aur.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farmer J, Reupert A. Understanding autism and understanding my child with autism: An evaluation of a group parent education program in rural Australia. Australian Journal of Rural Health. 2013;21(1):20–27. doi: 10.1111/ajr.12004. [DOI] [PubMed] [Google Scholar]
- Frea WD, Koegel LK, Koegel RL. Understanding why problem behaviors occur: A guide for assisting parents in assessing causes of behavior and designing treatment plans. Santa Barbara: University of California, Santa Barbara; 1994. [Google Scholar]
- Green J, Charman T, MCConachie H, Aldred C, Slonims V, Howlin P, Pickles A. Parent-mediated communication-focused treatment in children with autism (PACT): randomized controlled trial. The Lancet. 2010;375:19–25. doi: 10.1016/S0140-6736(10)60587-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurney J, McPheeters M, Davis M. Parental report of health conditions and health care use among children with and without autism. Archives of Pediatric and Adolescent Medicine. 2006;160:825–830. doi: 10.1001/archpedi.160.8.825. [DOI] [PubMed] [Google Scholar]
- Hamilton LM. Facing autism: Giving parents reasons for hope and guidance for help. Random House; Digital, Inc: 2008. [Google Scholar]
- Hardan AY, Gengoux GW, Berquist KL, Libove RA, Ardel CM, Phillips J, Minjarez MB. A randomized controlled trial of Pivotal Response Treatment Group for parents of children with autism. Journal of Child Psychology and Psychiatry. 2014 doi: 10.1111/jcpp.12354. [DOI] [PubMed] [Google Scholar]
- Hartley SL, Sikora DM, McCoy R. Prevalence and risk factors of maladaptive behaviour in young children with autistic disorder. Journal of Intellectual Disabilities Research. 2008;52:819–829. doi: 10.1111/j.1365-2788.2008.01065.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herring S, Gray K, Taffe J, Tonge B, Sweeney D, Einfeld S. Behaviour and emotional problems in toddlers with pervasive developmental disorders and developmental delay: Associations with parental mental health and family functioning. Journal of Intellectual Disability Research. 2006;50(12):874–882. doi: 10.1111/j.1365-2788.2006.00904.x. [DOI] [PubMed] [Google Scholar]
- Hoffman CD, Sweeney DP, Gilliam JE, Lopez-Wagner MC. Sleep problems in children with autism and in typically developing children. Focus on Autism and Other Developmental Disabilities. 2006;21:146–152. [Google Scholar]
- Homer CJ, Klatka K, Romm D, Kuhlthau K, Bloom S, Newacheck P, Perrin JM. A review of the evidence for the medical home for children with special health care needs. Pediatrics. 2008;122(4):e922–37. doi: 10.1542/peds.2007-3762. [DOI] [PubMed] [Google Scholar]
- Hyman SL, Johnson JK. Autism and pediatric practice: Toward a medical home. Journal of Autism and Developmental Disorders. 2012;42(6):1156–1164. doi: 10.1007/s10803-012-1474-3. [DOI] [PubMed] [Google Scholar]
- Ingersoll B, Dvortcsak A. Teaching social communication to children with autism: A manual for parents. New York: The Guilford Press; 2010. [Google Scholar]
- Ingersoll B, Dvortcsak A. Including parent training in the early childhood special education curriculum for children with autism spectrum disorders. Journal of Positive Behavior Interventions. 2006;8(2):79–87. doi: 10.1177/10983007060080020601. [DOI] [Google Scholar]
- Ingersoll B, Gergans S. The effect of a parent-implemented naturalistic imitation intervention on spontaneous imitation skills in young children with autism. Research in Developmental Disabilities. 2007;28:163–175. doi: 10.1016/j.ridd.2006.02.004. [DOI] [PubMed] [Google Scholar]
- Ingersoll B, Wainer A. Initial efficacy of Project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorder. 2013;43:2943–295. doi: 10.1007/s10803-013-1840-9. [DOI] [PubMed] [Google Scholar]
- Johnson CR, Handen BL, Butter E, Wagner A, Mulick J, Sukhodolsky DG, Smith T. Development of a parent training program for children with pervasive developmental disorders. Behavioral Interventions. 2007;22:201–221. [Google Scholar]
- Johnson CR, Turner K, Stewart PA, Schmidt B, Shui A, Macklin E, Hyman SL. Relationships between feeding problems, behavioral characteristics and nutritional quality in children with ASD. Journal of Autism and Developmental Disorders. 2014;44:2175–2184. doi: 10.1007/s10803-014-2095-9. [DOI] [PubMed] [Google Scholar]
- Kaat A, Lecavalier L. Disruptive behavior disorders in children and adolescents with autism spectrum disorders: A review of the prevalence, presentation, and treatment. Research in Autism Spectrum Disorders. 2013;7(12):1579–1594. [Google Scholar]
- Kanne SM, Gerber AJ, Quirmbach LM, Sparrow SS, Cicchetti DV, Saulnier CA. The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. Journal of Autism and Developmental Disorders. 2011;41:1007–1018. doi: 10.1007/s10803-010-1126-4. [DOI] [PubMed] [Google Scholar]
- Kasari C, Gulsrud AC, Wong C, Kwon S, Locke J. Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders. 2010;40:1045–1056. doi: 10.1007/s10803-010-0955-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Lawton K, Shih W, Barker TV, Landa R, Lord C, Senturk D. Caregiver-mediated intervention for low-resourced preschoolers with autism: An RCT. Pediatrics. 2014 doi: 10.1542/peds.2013-3229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kazdin AE. Parent Management Training: Treatment for Oppositional, Aggressive, and Antisocial Behavior in Children and Adolescents. New York: Oxford University Press; 2005. [Google Scholar]
- Klaus N, Fristad MA. Family psychoeducation: An adjunctive intervention for children with bipolar disorder. Directions in Psychiatry. 2005;25(3):217–230. doi: 10.1016/s0006-3223(03)00186-0. [DOI] [PubMed] [Google Scholar]
- Kogan M, Strickland B, Blumberg S, Singh G, Perrin J, van Dyck P. A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States. Pediatrics. 2008;122(6) doi: 10.1542/peds.2008-1057. [DOI] [PubMed] [Google Scholar]
- Liptak GS, Stuart T, Auinger P. Health care utilization and expenditures for children with autism: Data from U.S. national samples. Journal of Autism and Developmental Disorders. 2006;36(7):871–879. doi: 10.1007/s10803-006-0119-9. [DOI] [PubMed] [Google Scholar]
- Lubetsky MJ, Handen BL, Lubetsky M, McGonigle JJ. Systems of care for individuals with autism spectrum disorder and serious behavioral disturbance through the lifespan. Child and Adolescent Psychiatric Clinics of North America. 2014;23:97–110. doi: 10.1016/j.chc.2013.08.004. [DOI] [PubMed] [Google Scholar]
- Maskey M, Warnell F, Parr JR, Couteur AL, McConachie H. Emotional and behavioural problems in children with autism spectrum disorder. Journal of Autism and Developmental Disorders. 2013;48:851–859. doi: 10.1007/s10803-012-1622-9. [DOI] [PubMed] [Google Scholar]
- Matson ML, Mahan S, Matson JL. Parent training: A review of methods for children with autism spectrum disorders. Research in Autism Spectrum Disorders. 2009;3(40):868–875. doi: 10.10106/j.ras.2009.02.003. [DOI] [Google Scholar]
- McConachie H, Diggle T. Parent implemented early intervention for young children with autism spectrum disorder: A systematic review. Journal of Evaluation in Clinical Practice. 2007;13:120–129. doi: 10.1111/j.1365-2753.2006.00674.x. [DOI] [PubMed] [Google Scholar]
- McFarlane WR, Dixon L, Lukens E, Lucksted A. Family psychoeducation and schizophrenia: A review of the literature. Journal of Marital & Family Therapy. 2003;29:223–245. doi: 10.1111/j.1752-0606.2003.tb01202.x. [DOI] [PubMed] [Google Scholar]
- McNeil CB, Hembree-Kigin TL. Parent-Child Interaction Therapy. Second. New York: Springer; 2011. [Google Scholar]
- Michelson D, Davenport C, Dretzke J, Barlow J, Day C. Do evidence-based interventions work when tested in the “real world?”. A systematic review and meta-analysis of parent management training for the treatment of child disruptive behavior. Clinical Child and Family Psychology Review. 2013;16:18–34. doi: 10.1007/s10567-013-0128-0. [DOI] [PubMed] [Google Scholar]
- Miklowitz DJ, George E, Richards J, Simoneau TL, Suddath RL. A randomized study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder. Archives of General Psychiatry. 2003;60(9):904–912. doi: 10.1001/archpsyc.60.9.904. [DOI] [PubMed] [Google Scholar]
- Moes DR, Frea WD. Contextualized behavioral support in early intervention for children with autism and their families. Journal of Autism and Developmental Disorders. 2002;32(6):519–531. doi: 10.1023/a:1021298729297. [DOI] [PubMed] [Google Scholar]
- Murphy N, Carbone P. COCWD. Parent-provider-community partnerships: Optimizing outcomes for children with disabilities. Pediatrics. 2011;128(4):795–802. doi: 10.1542/peds.2011-1467. [DOI] [PubMed] [Google Scholar]
- National Research Council. Educating children with autism. Washington, DC: National Academy Press, Division of Behavioral and Social Sciences and Education, Committee on Educational Interventions for Children with Autism; 2001. [Google Scholar]
- National Standards Report. The national standards project—Addressing the need for evidence-based practice guidelines for autism spectrum disorders. Randolph: National Autism Center; 2009. [Google Scholar]
- Nefdt N, Koegel R, Singer G, Gerber M. The use of a selfdirected learning program to provide introductory training in pivotal response treatment to parents of children with autism. Journal of Positive Behavior Interventions. 2010;12(1):23–32. [Google Scholar]
- Nunes D, Hanline MF. Enhancing the alternative and augmentative communication use of a child with Autism through a parent-implemented naturalistic intervention. International Journal of Disability, Development, & Education. 2007;54(2):177–197. [Google Scholar]
- Odom SL, Boyd BA, Hall LJ, Hume K. Evaluation of comprehensive treatment models for individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2010;40:425–436. doi: 10.1007/s10803-009-0825-1. [DOI] [PubMed] [Google Scholar]
- Odom SL, Brown WH, Frey T, Karasu N, Smith-Carter L, Strain P. Evidence-based practices for young children with autism: Evidence from single-subject research design. Focus on Autism and Other Developmental Disabilities. 2003;18:176–181. doi: 10.1177/10883576030180030401. [DOI] [Google Scholar]
- Oono IP, Honey EJ, McConachie H. Parent-mediated early intervention for young children with autism spectrum disorders. Cochrane Database of Systematic Reviews. 2013;4 doi: 10.1002/14651858.CD009774.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oosterling I, Visser J, Swinkels S, Rommelse N, Donders R, Woudenberg T, Buitelaar J. Randomised controlled trial of the focus parent training for toddlers with autism: 1-yearoutcome. Journal of Autism and Developmental Disorders. 2010;40(12):1447–1158. doi: 10.1007/s10803-010-1004-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parellada M, Boada L, Moreno C, Llorente C, Romo J, Muela C, Arango C. Specialty care programme for autism spectrum disorders in an urban population: A case-management model for health care delivery in an ASD population. European Psychiatry. 2013;28:102–109. doi: 10.1016/j.eurpsy.2011.06.004. [DOI] [PubMed] [Google Scholar]
- Perry A, Flanagan HE, Dunn Geier J, Freeman NL. Brief report: the Vineland Adaptive Behavior Scales in young children with autism spectrum disorders at different cognitive levels. Journal of Autism and Developmental Disorders. 2009;39:1066–1078. doi: 10.1007/s10803-009-0783-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reagon KA, Higbee TS. Parent-implemented script fading to promote play-based verbal initiations in children with Autism. Journal of Applied Behavior Analysis. 2009;42(3):659–664. doi: 10.1901/jaba.2009.42-659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Research Units on Pediatric Psychopharmacology (RUPP) Autism Network. Parent training for children with pervasive developmental disorders: A Multi-site feasibility trial. Behavioral Interventions. 2007;22:179–199. [Google Scholar]
- Roberts J, Williams K, Carter M, Evans D, Parmenter T, Silove N, Warren A. A randomized controlled trial of two early intervention programs for young children with autism: Centre-based with parent program and home-based. Research in AutismSpectrum Disorders. 2011;5(4):1553–1566. [Google Scholar]
- Rogers SJ, Estes A, Lord C, Vismara L, Winter J, Fitzpatrick A, Dawson G. Effects of a brief Early Start Denver Model (ESDM) – Based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry. 2012;51(10):1052–1065. doi: 10.1016/j.jaac.2012.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scahill L, McDougle CJ, Aman MG, Johnson C, Handen B, Bearss K, Vitiello B. Effects of risperidone and parent training on adaptive functioning in children with pervasive developmental disorders and serious behavioral problems. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;51(2):136–146. doi: 10.1016/j.jaac.2011.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schertz HH, Odom SL. Promoting joint attention in toddlers with autism: A parent-mediated developmental model. Journal of Autism & Developmental Disorders. 2007;37:1562–1575. doi: 10.1007/s10803-006-0290-z. [DOI] [PubMed] [Google Scholar]
- Schultz TR, Schmidt CT, Sticher JP. A review of parent education programs for parents of children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities. 2011;26(2):96–104. doi: 10.1177/1088357610397346. [DOI] [Google Scholar]
- Sharp WG, Berry RC, McCracken C, Nuhu NN, Marvel E, Saulnier CA, Jaquess DL. Feeding problems and nutrient intake in children with autism spectrum disorders: A meta-analysis and comprehensive review of the literature. Journal of Autism and Developmental Disorders. 2013;43:2159–217. doi: 10.1007/s10803-013-1771-5. [DOI] [PubMed] [Google Scholar]
- Sharp WG, Burrell TL, Jaquess DJ. The autism meal plan: A parent-training curriculum to manage eating aversions and low intake among children with autism. Autism. 2013;18(6):712–722. doi: 10.1177/1362361313489190. [DOI] [PubMed] [Google Scholar]
- Sharp WG, Jaquess DL, Morton JF, Miles AG. A retrospective chart review of dietary diversity and feeding behavior of children with autism spectrum disorder before and after admission to a day-treatment program. Focus on Autism and Other Developmental Disabilities. 2009;1:1–13. doi: 10.1177/1088357609349245. [DOI] [Google Scholar]
- Siller M, Hutman T, Sigman M. A parent-mediated intervention to increase responsive parental behaviors and child communication in children with ASD: A randomized clinical trial. Journal of Autism & Developmental Disorders. 2013;43(3):540–555. doi: 10.1007/s10803-012-1584-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry. 2008;47(8):921–929. doi: 10.1097/CHI.0b013e318179964f. [DOI] [PubMed] [Google Scholar]
- Smith IM, Koegel RL, Koegel LK, Openden DA, Fossum KL, Bryson SE. Effectiveness of a novel community-based early intervention model for children with autistic spectrum disorder. American Journal of Intellectual and Developmental Disabilities. 2010;115(6):504–523. doi: 10.1352/1944-7558-115.6.504. [DOI] [PubMed] [Google Scholar]
- Smith LE, Greenberg JS, Mailick MR. The family context of autism spectrum disorders: Influence on the behavioral phenotype and quality of life. Child and Adolescent Psychiatric Clinics of North America. 2014;23(1):143–155. doi: 10.1016/j.chc.2013.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith T, Groen AD, Wynn JW. Randomized Trial of Intensive Early Intervention for Children with Pervasive Developmental Disorder. American Journal of Mental Retardation. 2000;105(4):269–285. doi: 10.1352/0895-8017(2000)105<0269:RTOIEI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Sofronoff K, Leslie A, Brown W. Parent management training and Asperger syndrome: a randomized controlled trial to evaluate a parent based intervention. Autism. 2004;8(3):301–17. doi: 10.1177/1362361304045215. [DOI] [PubMed] [Google Scholar]
- Smith T, Scahill L, Dawson G, Guthrie D, Lord C, Odom S, Wagner A. Designing research studies on psychosocial interventions in autism. Journal of Autism and Developmental Disorders. 2007;37:354–366. doi: 10.1007/s10803-006-0173-3. [DOI] [PubMed] [Google Scholar]
- Solomon R, Necheles J, Ferch C, Bruckman D. Pilot study of a parent training program for young children with autism: The PLAY project consultation program. Autism. 2007;11(3):204–224. doi: 10.1177/1362361307076842. [DOI] [PubMed] [Google Scholar]
- Stahmer AC, Gist K. The effects of an accelerated parent education program on technique mastery and child outcome. Journal of Positive Behavior Interventions. 2001;3:75–82. [Google Scholar]
- Steiner A, Koegel L, Koegel R, Ence W. Issues and theoretical constructs regarding parent education for autism spectrum disorders. Journal of Autism and Developmental Disorders. 2012;42:1218–1227. doi: 10.1007/s10803-011-1194-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sussman F. More than words: A parent’s guide to building interaction and language skills for children with autism spectrum disorder or social communication difficulties. Toronto: The Hanen Centre; 2012. [Google Scholar]
- Symon JB. Parent education for autism: Issues in providing services at a distance. Journal of Positive Behavior Interventions. 2001;3(3):160–174. doi: 10.1177/109830070100300304. [DOI] [Google Scholar]
- Symon JB. Expanding interventions for children with autism: Parents as trainers. Journal of Positive Behavior Interventions. 2005;7(3):159–173. [Google Scholar]
- Tarbox J, Schiff A, Najdowski AC. Parent-implemented procedural modification of escape extinction in the treatment of food selectivity in a young child with Autism. Education & Treatment of Children. 2010;33(2):223–234. [Google Scholar]
- Tonge B, Brereton A, Kiomall M, Mackinnon A, King N, Rinehart N. Effects on parental mental health of an education and skills training program for parents of young children with autism: a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2006;45(5):561–569. doi: 10.1097/01.chi.0000205701.48324.26. [DOI] [PubMed] [Google Scholar]
- Tonge B, Brereton A, Kiomall M, Mackinnon A, Rinehart NJ. A randomized group comparison controlled trial of ‘preschoolers with autism’: A parent education and skills training intervention for young children with autistic disorder. The International Journal of Research & Practice. 2014;18(2):166–177. doi: 10.1177/1362361312458186. [DOI] [PubMed] [Google Scholar]
- Volkmar FR, Wiesner LA. A Practical Guide to Autism: What Every Parent, Family Member, and Teacher Needs to Know. Hoboken, NJ: John Wiley & Sons, Inc; 2009. [Google Scholar]
- Wacker DP, Lee JF, Padilla Dalmau YC, Kopelman TG, Lindgren SD, Kuhle J, Waldron DB. Conducting Functional Communication Training via telehealth to reduce the problem behavior of young children with autism. Journal of Developmental and Physical Disabilities. 2013;25(1):35–48. doi: 10.1007/s10882-012-9314-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wahler RG, Vigilante VA, Strand PS. Generalization of child’s oppositional behavior across home and school. Journal of Applied Behavior Analysis. 2004;37(1):43–51. doi: 10.1901/jaba.2004.37-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitaker P. Supporting families of preschool children with autism: What parents want and what helps. Autism. 2002;6:411–426. doi: 10.1177/1362361302006004007. [DOI] [PubMed] [Google Scholar]
- Whittingham K, Sofronoff K, Sheffield J, Sanders MR. Stepping Stones Triple P: an RCT of a parenting program with parents of a child diagnosed with an autism spectrum disorder. Journal of Abnormal Child Psychology. 2009;37(4):469–80. doi: 10.1007/s10802-008-9285-x. [DOI] [PubMed] [Google Scholar]
- Wong VCN, Kwan QK. Randomized controlled trial for early intervention for autism: a pilot study of the Autism 1-2-3 Project. Journal of Autism and Developmental Disorders. 2010;40(6):677–88. doi: 10.1007/s10803-009-0916-z. [DOI] [PubMed] [Google Scholar]