

Abstract
Thousands of orphaned survivors of the 1994 Rwandan Genocide against the Tutsi were not only exposed to extraordinarily severe forms of violence, but also many of these children took on the responsibility of caring and providing for other child survivors. This study describes the poverty, educational attainment, social support and mental health of orphaned heads of household (OHH) fourteen years after the genocide, and analyzes how violence exposure during the genocide and post-genocide stressors contributed to symptoms of posttraumatic stress disorder (PTSD) and distress. Participants were 61 members of an OHH community organization who were interviewed in 2002 about their genocide experiences and who provided a follow-up assessment of post-genocide risk factors and PTSD and distress symptoms in 2008. Almost all of the OHH in this study reported low social support, high levels of poverty, and high rates of PTSD and distress symptoms. Lower educational attainment predicted PTSD symptoms and partially mediated the association between exposure to genocide violence and PTSD. Distress was predicted by lack of social support and witnessing family members harmed during the genocide. Results suggest that public health and community efforts to improve educational outcomes and to strengthen and expand social support networks may improve mental health outcomes of OHH.
Keywords: Post-genocide stressors, Rwanda, PTSD, distress, orphans
Armed conflicts have devastated entire societies and left millions of children disabled, homeless, orphaned or separated from their parents (The United Nations Children’s Fund, 1996). One such group is child survivors of the 1994 Rwandan Genocide against the Tutsi. During the Rwandan Genocide, hundreds of thousands of people were brutally murdered (Republic of Rwanda, 2014). Survivors of the genocide were exposed to extreme levels of physical and psychological violence including rape, torture, mutilation, and witnessing their family members and loved ones being attacked and murdered. Studies have reported that 94% of people in Rwanda during the genocide experienced at least one genocide event including witnessing the murder of family members, having their property and homes destroyed, and having their lives threatened (Pham, Weinstein, & Longman, 2004). Virtually every child survivor witnessed violence and believed they would die during the genocide (Dyregrov, Gupta, Gjestad, & Mukanoheli, 2000). Many children lost most, if not all, of their family members, and took on the responsibility of caring and providing for other child survivors (Schaal & Elbert, 2006). Indeed, in 2001, seven years after the genocide, it was estimated that 37% of households in Rwanda were headed by children, a higher rate than any country in Sub-Saharan Africa, and possibly the world (The United Nations Children’s Fund, 2003).
Given these experiences, it is not surprising that psychological distress is highly prevalent in survivors of the Rwandan Genocide. Estimates of probable posttraumatic stress disorder (PTSD) diagnoses in orphaned survivors in Rwanda range from 29% to 79% (Dyregrov et al., 2000; Neugebauer et al., 2009; Schaal, Dusingizemungu, Jacob, & Elbert, 2011), with those who were between the ages of 11 and 20 during the genocide being at the highest risk for PTSD (Munyandamutsa, Nkubamugisha, Gex-Fabry, & Eytan, 2012). In addition to PTSD symptoms, a substantial proportion of survivors of the Rwandan Genocide have been found to have distress symptoms, including depression and anxiety (Cohen et al., 2009; Munyandamutsa et al., 2012). Almost half of youth heads of household have been reported to meet the clinical cut-off for depression (Boris et al., 2008).
The range in mental health symptoms reported by orphaned survivors likely can be explained in part by the number and nature of experienced genocide events, with witnessing the attack of a parent being the Rwandan Genocide experience that has been found to be most strongly predictive of PTSD symptoms (Neugebauer et al., 2009; Schaal et al., 2011; Schaal, Weierstall, Dusingizemungu, & Elbert, 2012). However, mental health problems in survivors have not been wholly explained by genocide exposure.
In addition to direct effects, survivors of war may experience indirect effects of exposure to violence on PTSD and depression because violent conflict may disrupt the lives and social support networks that individuals need to survive and cope with stress. Daily stressors, such as poverty and limited access to education and social support, may partially mediate the relation of violence exposure to mental health. War may result in a host of daily stressors, which in turn negatively impact mental health (Fernando, Miller, & Berger, 2010; Miller & Rasmussen, 2010). War can destroy people’s homes, livelihoods, families, and communities, as well as a society’s economy and infrastructure, thereby increasing poverty and isolating people from social services such as clean water, medical care, and education. The social ecological model of child development proposes that disruptions in these aspects of the environment put children at higher risk for poor mental health outcomes including PTSD and depression (Bronfenbrenner, 1979). Thus, living through a genocide may not only result in increased risk for poor mental health directly, but may also result in secondary adversities that may mediate the association between genocide events and psychological difficulties (Bolton, 2001b; Saltzman, Layne, Steinberg, Arslanagic, & Pynoos, 2003).
These secondary adversities and daily stressors may be particularly challenging for children orphaned by the genocide. In convenience samples, researchers have found that many orphans in post-genocide Rwanda felt overwhelmed by daily tasks and the hard labor required to meet their basic needs, and regularly went without food (Boris et al., 2008; Schaal & Elbert, 2006). These studies also found higher rates of PTSD in children living in orphan-headed households than those living in orphanages (Schaal & Elbert, 2006). The researchers posited that the reason for this difference was because those living in the orphanages tended to have better psychosocial environments such as better access to food, shelter, education, and medical services, and less responsibilities and stress than those living in orphan-headed homes (Schaal & Elbert, 2006).
A major secondary adversity in Rwanda, where almost every family lost members during the genocide, may be the decimation of social support networks. The disintegration of social bonds has been hypothesized to be an important factor in hindering psychological adjustment (Scholte et al., 2011). Orphans in Rwanda have been found to have a severe lack of social support, most notably support from an adult (Thurman et al., 2006). This was especially true for orphaned heads of household (OHH), who reported that unlike their younger siblings or housemates, they had no one to turn to for advice or assistance (Ward & Eyber, 2009). Other studies have found that OHH experience a great deal of social isolation and lack of trust (Boris et al., 2008).
Finally, researchers have found that orphans in Rwanda had worse educational outcomes than their non-orphaned peers, independent of the genocide experience (Akresh & De Walque, 2008). Moreover, children who were in Rwanda at the time of the genocide had worse educational outcomes than those who were not (Akresh & De Walque, 2008). Thus, in attempting to access education, orphaned survivors of the genocide shoulder a double burden of experiencing the genocide and being orphans. Lack of access to education that can result from genocide and orphanhood may be a proximal cause of increased psychological difficulties.
While mental health outcomes, specifically traumatic stress and distress symptoms, often co-occur, they may be differentially predicted by genocide exposure and post-genocide risk factors, such as daily stressors. Research on war affected populations has found that genocide exposure primarily predicts PTSD, while daily stressors have been found to predict only depression (Cohen et al., 2009), or both depression and PTSD (Heptinstall, Sethna, & Taylor, 2004; Schweitzer, Melville, Steel, & Lacherez, 2006). Understanding more about the ways that potentially modifiable post-genocide risk factors differentially predict PTSD and distress may offer insight into appropriate avenues for intervention for one or both of these conditions.
This study describes the poverty, educational attainment, social support and mental health of OHH, and analyzes how violence exposure during the genocide and post-genocide risk factors contribute to mental health outcomes 14 years after the Rwandan Genocide. It was hypothesized that violence exposure during the genocide and witnessing family members being attacked would positively predict PTSD and distress symptoms. In addition, the study hypothesized that after accounting for these genocide experiences, poverty would further exacerbate these symptoms, while social support and educational attainment would mitigate them. Post-genocide risk factors that were found to predict PTSD or distress after accounting for genocide experiences were tested to determine whether they partially mediated the association between genocide experiences and PTSD symptoms.
Method
Participants
Participants in this study were 61 OHH members of a Rwandan association of orphaned heads of household who participated in both time points of a longitudinal study conducted in 2002 and 2008 (Ng, Ahishakiye, Miller, & Meyerowitz, In Press). The association is a local nongovernmental organization that advocates for services for members including housing and educational assistance. All of the participants were double-orphans, meaning that both of their parents had died. The mean age of the 61 participants who completed the follow-up assessment was 13.81 (SD=5.31) at the time of the genocide and 34 (55.74%) were men.
Procedure
In 2002, approximately 8 years after the Rwandan Genocide, with training and support from two of the authors, the association collected demographic information and genocide testimonies of 100 association members. The semi-structured interview protocol was designed and approved by the association board and a non-profit umbrella organization of local Rwandan Genocide survivor associations. Interviewers were also association members. Participants were selected by the association board to represent OHH from a wide range of geographical areas and to have roughly equal numbers of males and females. Participants were approached and asked if they wanted to give testimony of their genocide experiences. Interviews were conducted in Kinyarwanda in participants’ homes, in village locations that were selected by the participants, or in the association headquarters in Kigali City. Audiorecordings were translated and transcribed into English by a native Kinyarwanda speaker. Three of the genocide testimonies could not be located and so data on genocide experiences were only available for 97 participants.
In 2008, a follow-up study was conducted to collect data on mental health problems and risk factors from 99 of the original 100 participants (one of the 2002 participants asked to remain anonymous and was therefore not included in the follow-up). All study methods were approved by the association board and the University of Southern California Institutional Review Board. Interviewers sought out participants at their last known village or address. If the original participants could not be located, interviewers asked neighbors or friends for information about their possible whereabouts, and attempted to locate them. Once located, the purpose and procedures of the follow-up study were explained and participants gave informed consent. Sixty-three of the original participants were located and 61 agreed to participate in the follow-up. Of the remaining 36 people who could not be located for the follow-up, information was available about the presumed whereabouts of 12: one had joined the military, two were away at jobs and school in other countries, seven had relocated and could not be found, and two were under psychiatric care. Results of attrition analyses using logistic regression to predict follow-up completion found no significant differences in the completers and non-completers (see Table 1).
Table 1.
Participant Characteristics and Results of Attrition Analyses Predicting Follow-up Completion
| 2002 Variable | Total | Completed Follow-Up | Lost to Follow-Up | OR (SE) | p | |||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||
| N | Estimate | N | Estimate | N | Estimate | |||
| Male; n (%) | 100 | 58 (58.00) | 61 | 34 (55.74) | 39 | 24 (61.54) | .79 (.33) | .57 |
| Age (in years) in 2002; Mean (SD) | 88 | 22.25 (5.06) | 53 | 21.81 (5.31) | 35 | 22.91 (4.64) | .96 (.04) | .32 |
| Genocide Violence Exposure; (Mean, SD) | 97 | 11.05 (4.26) | 58 | 11.43 (4.27) | 39 | 10.49 (4.24) | 1.06 (.05) | .29 |
| Witnessed Family Attacked; n (%) | 97 | 61 (62.89) | 58 | 35 (60.34) | 39 | 26 (66.67) | .76 (.33) | .53 |
| Return to School (n, %) | 92 | 68 (73.91) | 56 | 40 (71.43) | 36 | 28 (77.78) | .71 (.36) | .50 |
For the 2008 follow-up study, interview questions and measures were developed by some of the authors in collaboration with the association board and were selected from existing validated measures. To assist with measuring constructs in culturally appropriate ways, five focus groups that ranged in size from six to 12 OHH were convened from each area of the country to gather information about their day-to-day lives, experiences, and mental health concerns, and to evaluate the face validity of standard measures and assess their cultural appropriateness. After revisions and approval by the association board, measures and interview protocols were forward- and back-translated between English and Kinyarwanda by native Kinyarwanda speakers to ensure accuracy. Six association members were selected as interviewers by the association board, and participated in a week-long training on semi-structured interviewing conducted by some of the authors and the association project director. Interviews, which were conducted in Kinyarwanda, were audio recorded and translated into English by native Kinyarwanda speakers.
English transcripts of the 2002 and 2008 interviews were coded using content analysis (Neuendorf, 2002) by four blinded research assistants to obtain quantitative measurements of genocide events and post-genocide risk factors. In order to code the transcripts efficiently, sequential overlapping coding, also known as a “not fully crossed” coding design, was used (Hallgren, 2012; Neuendorf, 2002). Therefore, every interview was randomly assigned to two coders, with six possible combinations of coders. In cases where discrepancies or missing information remained even after coders independently checked their own coding, items were reviewed and final decisions were made based on a close reading of the interview. Interrater reliability for each pair of coders was calculated using two-way mixed average-measures Intraclass Correlation Coefficients (ICCs). ICC consistency was calculated as absolute agreement for binary items and as consistency for ordinal items. The mean ICC, weighted by the number of transcripts coded by each pair, and range of ICC scores are reported below in the measures section.
Measures
Demographics
Participants’ Gender and Age were obtained from the 2002 interviews.
PTSD Symptoms
PTSD Symptoms were assessed in 2008 using an adapted version of the Impact of Events Scale-Revised (IES-R) (Weiss & Marmar, 1997). The IES-R is a twenty-two item self-report questionnaire that measures PTSD symptoms, scored 0=“Not at all” to 4=“Extremely.” Although the IES-R was not developed for use in Rwanda, it has been used in post-genocide Rwandan samples (Dyregrov et al., 2000). The scale score was calculated as the mean of the items. There was disagreement about the translation of item 17 (I tried to remove it from my memory) and so this item was dropped from the scale, resulting in a 21-item scale with excellent internal reliability (Cronbach’s alpha=.91).
Distress Symptoms
Distress Symptoms were measured in 2008 using a locally-derived Symptom Checklist that was developed for this study using responses from focus groups of OHH to measure different forms of psychological distress in Rwandan OHH, including depression, anxiety, and behavioral problems. The Symptom Checklist is a 26-item scale that asks participants to indicate how intense the severity of a particular symptom was over the past two months. Severity ranged from 0=“Not at all” to 4=“Extremely” and the scale score was the mean. Internal reliability of the scale was excellent (Cronbach’s alpha=.91). The original scale consisted of 36-items, but four items were dropped because of poor translations and two items had very low to no endorsement, and so they were also dropped from the analyses. After determining that the missingness of the Symptom Checklist items for the 39 participants not interviewed at follow-up were missing completely at random (MCAR) by analyzing them using Little’s MCAR analysis in SPSS 19’s Missing Values program (Little’s MCAR Test χ2= 507.12, DF=468, p=.10) (IBM Corp., 2010), scale reduction through reliability analysis was used to improve the internal reliability of the measure. Reliability analysis revealed that four additional items had corrected item-total correlation scores ≤ .20 and were dropped from the scale.
Genocide Violence Exposure
Genocide Violence Exposure was coded from the 2002 genocide testimonies. Codes were developed from the Rwandese Children’s Exposure to War Scenes Measure (Dyregrov et al., 2000), which assesses exposure to events that were common during the Rwandan Genocide. In order to ensure that the codes were comprehensive and specific to OHH in this study, additional items were added that were relevant to the sample (Layne et al., 2010; Netland, 2001, 2005). Example genocide events include reports of having your home destroyed, being attacked, being beaten, being raped, witnessing people being killed, and seeing dead bodies. In total, 41 different genocide experiences were coded 1=reported, and 0=not reported (see Table 2). The sum score of all 41 items was the total score for Genocide Violence Exposure. The weighted mean ICC was .97 and the range was .95 to .99.
Table 2.
Reported Genocide Violence Exposure in 2002 Sample and Comparison between 2008 Follow-Up Completers and Non-Completers
| Genocide Violence Exposure Events | 2002 Sample (n=97) | 2008 Completers (n=58) | 2008 Non-Completers (n=39) | X2 |
|---|---|---|---|---|
|
| ||||
| n (%) | n (%) | n (%) | ||
| Experienced Violence | ||||
| House destroyed or damaged | 92 (94.85) | 55 (94.83) | 37 (94.87) | <.001 |
| Threatened with death | 81 (83.51) | 52 (89.66) | 29 (74.36) | 3.96* |
| Attacked or assaulted | 60 (61.86) | 40 (68.97) | 20 (51.28) | 3.09 |
| Injured | 40 (41.24) | 26 (44.83) | 14 (35.90) | 1.05 |
| Shot at but not hit | 27 (27.84) | 17 (29.31) | 10 (26.32) | .10 |
| Beaten (ex: with sticks, impiri, or ubuhiri) | 24 (24.74) | 13 (22.41) | 11 (28.21) | .42 |
| Shells/grenades/mortars fired at you but weren’t hit | 18 (18.56) | 13 (22.41) | 5 (12.82) | 1.42 |
| Cut (ex: with machete, hoe, or knife) | 9 (9.28) | 4 (6.90) | 5 (12.82) | .92 |
| Shot | 8 (8.25) | 8 (13.79) | 0 (0.00) | 5.86* |
| Raped by one person | 6 (6.19) | 4 (6.90) | 2 (5.13) | .13 |
| Experienced other violencea | 3 (3.09) | 3 (5.17) | 0 (0.00) | 2.12 |
| Had body parts amputated | 3 (3.09) | 2 (3.45) | 1 (2.56) | .07 |
| Raped by more than one person at once | 3 (3.09) | 3 (5.17) | 0 (0.00) | 2.08 |
| Thrown into a pit or latrine | 3 (3.09) | 1 (1.72) | 2 (5.13) | .90 |
| Hit with shells/grenades/mortar fire | 2 (2.06) | 2 (3.45) | 0 (0.00) | 1.40 |
| Drowned (attempted) | 2 (2.06) | 2 (3.45) | 0 (0.00) | 1.40 |
| Held as a sex slave | 2 (2.06) | 1 (1.72) | 1 (2.56) | .08 |
| Forced to kill or attack others | 1 (1.03) | 1 (1.72) | 0 (0.00) | .66 |
| Impaled (ex: with a stick or spear) | 1 (1.03) | 0 (0) | 1 (2.56) | 1.50 |
| Witnessed Violence | ||||
| Someone being killed | 91 (93.81) | 54 (93.10) | 37 (94.87) | .13 |
| Someone being attacked | 85 (87.63) | 51 (87.93) | 34 (87.18) | .12 |
| Dead bodies | 70 (72.16) | 42 (72.41) | 28 (71.79) | .004 |
| Many people killed at once (massacres) | 56 (57.73) | 33 (56.90) | 23 (58.97) | .04 |
| People being cut | 56 (57.73) | 34 (58.62) | 22 (56.41) | .05 |
| People beaten | 37 (38.14) | 22 (37.93) | 15 (38.46) | .003 |
| People being shot | 36 (37.11) | 21 (36.21) | 15 (39.47) | .10 |
| People thrown in pits or latrines | 35 (36.08) | 22 (37.93) | 13 (33.33) | .21 |
| Houses destroyed | 35 (36.08) | 20 (34.48) | 15 (38.46) | .16 |
| People being raped by one person | 29 (29.90) | 16 (27.59) | 13 (33.33) | .37 |
| Babies or children being killed | 24 (24.74) | 16 (27.59) | 8 (20.51) | .63 |
| People being shelled | 21 (21.65) | 15 (25.86) | 6 (15.38) | 1.51 |
| People raped by more than one person | 21 (21.65) | 11 (18.97) | 10 (25.64) | .61 |
| People being impaled | 16 (16.49) | 10 (17.24) | 6 (15.38) | .06 |
| People having body parts amputated | 16 (16.49) | 13 (22.41) | 3 (7.69) | 3.67 |
| Other violence | 14 (14.43) | 10 (17.24) | 4 (10.26) | .92 |
| People held as sex slaves | 13 (13.40) | 7 (12.07) | 6 (15.38) | .22 |
| People being drowned | 9 (9.28) | 5 (8.62) | 4 (10.26) | .07 |
| People screaming for help | 7 (7.22) | 5 (8.62) | 2 (5.13) | .42 |
| People committing suicide | 7 (7.22) | 5 (8.62) | 2 (5.13) | .43 |
| People forced to kill others | 5 (5.15) | 2 (3.45) | 3 (7.69) | .86 |
| People raped with objects | 4 (4.12) | 2 (3.45) | 2 (5.13) | .17 |
| Witnessing Family Being Attacked | 61 (62.89) | 35 (60.34) | 26 (66.67) | .40 |
| Total No. of Genocide Violence Events, Mean (SD) | 11.05 (4.26) | 11.43 (4.27) | 10.49 (4.24) | t=−1.07, p=.287 |
p<.05
Witnessing Family Attacked
Witnessing Family Attacked was coded from the 2002 genocide testimonies. If participants mentioned witnessing their mother, father, or siblings being attacked, they received a score of one, otherwise they received scores of zero. The weighted mean ICC was .93 (range = .78 to 1.00).
Return to School
In the 2002 interview, participants were asked whether they had returned to school after the genocide, and this was coded as a binary (0=No, 1=Yes) variable. The weighted mean ICC was .96 (range = .82 to 1.00).
Educational Attainment
Educational Attainment was coded from participant responses during the 2008 interviews in which they were asked to identify the highest level of education they had attained. Responses were coded into seven ordinal categories ranging from 1=Less than Primary School to 7=Graduate School. If no information was available about educational attainment, it was coded as missing. The weighted mean ICC for Educational Attainment was .97 (range = .93 to 1.00).
Social Support
Social Support was measured in 2008 using the mean of an adapted version of the Medical Outcomes Study Social Support Scale (Sherbourne & Stewart, 1991). The 6-item questionnaire asked participants to rate their perceived social support over the past two months (e.g., “Are there people in your life whom you can trust?”) on scale from 1 (“Not at All”) to 5 (“A Lot”). Cronbach’s alpha was .83.
Poverty
Poverty was measured using the mean of a scale created from variables coded from the 2008 interview that assessed lack of resources. Nine binary (0=No, 1=Yes) items indicated lack of resources, including being unemployed, lacking food, not having water in the home, and not having electricity in the home. Mean weighted ICC of the coded scales was .95 (range = .90 to .97) and the Cronbach’s alpha was .71.
Analyses
To determine whether the follow-up sample of 61 participants differed significantly from the 39 original participants who were not included in the follow-up, logistic, anova, and X2 tests were run in which each of the variables assessed in 2002 predicted participation in the follow-up study. To assess whether the covariates Gender and Age, Genocide Violence Exposure, and post-genocide risk factors predicted PTSD and Distress Symptoms, nested regressions were run in which Gender and Age were entered in model one, Genocide Violence Exposure and Witnessing Family Attacked were added in model two, and Return to School, Educational Attainment, Poverty, and Social Support were entered in model three. Fisher’s r to z transformation was used to compute the average R2 and adjusted R2 values across imputations (Harel, 2009), and Wald tests were used to assess whether including the new set of predictors improved the overall fit of the model.
Mediation analyses were conducted to assess whether significant post-genocide predictors of mental health outcomes mediated the association between Genocide Violence Exposure and mental health. The covariates of Gender and Age were included in the mediation analyses. The significance of the indirect effects was tested using sgmediation with 5,000 bootstrapped samples with case resampling to account for bias in the standard error of the indirect effect. Bootstrapping has been found to provide the most accurate confidence intervals for indirect effects, particularly with small sample sizes (Preacher & Hayes, 2004, 2008). All analyses were conducted using Stata version 12 (StataCorp, 2011). Multiple imputation using 50 imputations was used to impute missing data from the 61 participants.
Results
Genocide violence exposure and witnessing family attacked
Of the 61 participants, genocide exposure data were available for 58 (genocide testimonies were missing for three participants). Results of X2 tests assessing differences in endorsement of each of the Genocide Violence Exposure items between the 58 participants who completed the 2008 interview and the 39 who did not indicated that of the 41 different Genocide Violence Exposure items, endorsement rates differed between the samples for only two, such that participants who completed the 2008 follow-up were more likely to have been threatened with death (X2=3.96, p<.05) and shot (X2=5.86, p=.02). There were no differences between the samples in the total Genocide Violence Exposure Scores (t=1.07, p=.29) or Witnessing Family Attacked (X2=.40, p=.53) (see Table 2).
The 58 participants reported experiencing an average of 11.43 (SD=4.27) of 41 different Genocide Violence Exposure events, and 60.34% of participants witnessed at least one family member being attacked, with 32.76% witnessing their mothers being attacked, 25.86% witnessing their fathers being attacked, and 44.83% witnessing a sibling being attacked. Most of the participants (89.66%) reported that they were threatened with death, 68.97% reported being physically attacked or assaulted, and 44.83% reported being injured during the genocide. In addition, 98.25% of participants reported that they had witnessed people being massacred, killed, or attacked and 72.41% reported seeing dead bodies. Sexual violence was witnessed by 41.38% of participants and experienced by 8.62% of participants (four women and one man) (see Table 2)
PTSD symptoms
PTSD Symptoms were highly prevalent (see Table 3). The mean PTSD Symptoms score was 2.29 out of 4 (SD=.85), with 82% of participants having scores at or above 1.5, which has been found to be the IES-R cut-off with the best diagnostic accuracy for assessing PTSD in Vietnam veterans (Creamer, Bell, & Failla, 2003). For seven of the 21 items, more than 60% of participants responded that they experienced the symptom “A lot/Quite a bit” or “Extremely,” with the most frequently endorsed items being “You didn’t understand how the genocide could have happened” (70.49%; mean=2.97, SD=1.21), “Anything reminds you of the genocide” (73.77%; mean=2.93, SD=1.09), and “Picturing the genocide” (65.57%; mean=2.85, SD=1.38).
Table 3.
Post-Genocide Risk and Resiliency Factors and Mental Health (N=61)
| Binary Items | N | n (%) |
|---|---|---|
| Return to School | 56 | 40 (71.43%) |
| Educational Attainment, Mean (SD) | 48 | 3.50 (1.50) |
| 1 = Less than primary school | 5 (10.42%) | |
| 2 = Completed primary | 6 (12.50%) | |
| 3 = Some secondary | 16 (33.33%) | |
| 4 = Completed secondary school | 8 (16.67%) | |
| 5 = Some university | 8 (16.67%) | |
| 6= Completed university | 4 (8.33%) | |
| 7= Graduate school | 1 (2.08%) | |
| Poverty, Mean (SD) | 61 | .70 (.22) |
| Things you can’t do because you lack the means | 60 | 58 (96.67%) |
| Sometimes lack food | 58 | 55 (94.83%) |
| Mention problems getting food | 61 | 54 (88.52%) |
| No water in your home | 61 | 53 (86.89%) |
| No permanent job | 61 | 49 (80.33%) |
| No electricity in your home | 55 | 34 (61.80%) |
| Typically eating less than two meals a day | 48 | 20 (41.67%) |
| Unemployed | 61 | 28 (45.90%) |
| Being a cultivator/farmer | 61 | 18 (29.51%) |
| Continuous Measures | Possible Range | Actual Range | N | Mean (SD) |
|---|---|---|---|---|
| Social Support | 1 – 5 | 1 – 3.83 | 61 | 2.04 (.56) |
| PTSD Symptoms | 0 – 4 | 0 – 3.90 | 61 | 2.29 (.85) |
| Distress | 0 – 4 | 0.15 – 3.27 | 61 | 1.37 (.79) |
Distress symptoms
Distress Symptoms were also elevated in the follow-up sample (see Table 3), with more than 40% of the sample indicating that they felt “Quite a bit” or “Extremely” on each of the following items: anxious (67.21%; mean=2.77, SD=1.44), sad and depressed (59.01%; mean=2.67, SD=1.36), scared (45.90%; mean=1.95, SD=1.43), lonely (44.26%; mean=1.82, SD=1.62), and isolated (40.99%; mean=1.95, SD=1.70). More than 40% of participants reported that they experienced headaches (47.54%; mean=2.10, SD=1.59) and nightmares (40.98%; mean=1.95, SD=1.47) “Quite a bit” or “Extremely.”
Return to school and educational attainment
By 2002, more than 70% of participants reported that they had returned to school following the genocide and by 2008, 43.75% had completed secondary school, with 27.08% continuing on to higher education (see Table 3).
Poverty
In 2008, almost one-third of participants were cultivators (29.51%) and 45.90% of participants were unemployed with no source of income. Less than 20% of participants had permanent employment (19.67%). Participants reported great difficulty accessing food and water, with 94.83% reporting not having enough food and 41.67% regularly eating fewer than two meals per day. Only 13.11% of participants had a source of water in their homes (see Table 3).
Social support
Social Support was low for almost all participants, with 81.97% of participants rating themselves on average as having “none” or “very few” people in their lives who provide social support (see Table 3).
Prediction of PTSD symptoms
Table 4 provides correlations between all study variables. Results of the nested regressions indicated that PTSD Symptoms were linearly and positively predicted by Genocide Violence Exposure (β =.36, p=.009), but that when post-genocide factors were added to the model, the model fit improved, and Genocide Violence Exposure was no longer a significant predictor of PTSD Symptoms (β=.17, p=.26) (see Table 5). In the final model, Educational Attainment was the only significant predictor of PTSD symptoms (β=−.47, p=.05). The final model accounted for 23% of the variance in PTSD symptoms.
Table 4.
Correlations Between Study Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Male | --- | ||||||||
| 2. Age | .07 | --- | |||||||
| 3. Genocide Violence Exposure | −.17 | −.06 | --- | ||||||
| 4. Witnessing Family Attacked | −.18 | −.32** | .32** | --- | |||||
| 5. Return to School | .13 | −.45*** | .03 | .19 | --- | ||||
| 6. Educational Attainment | .22 | .01 | −.31* | −.11 | .55*** | --- | |||
| 7. Poverty | −.17 | −.31* | .41** | .14 | −.02 | −.55*** | --- | ||
| 8. Social Support | .15 | .04 | −.32* | ,05 | −.07 | .06 | −.30* | --- | |
| 9. PTSD Symptoms | −.15 | .05 | .35** | .10 | −.17 | −.41** | .36** | −.20 | --- |
| 10. Distress Symptoms | −.32* | −.06 | .29* | .27* | −.28* | −.44** | .46*** | −.35** | .73*** |
p<.05,
p<.01,
p<.001
Table 5.
Nested Models Predicting PTSD and Distress Symptoms (N=61)
| Predictor | PTSD Symptoms | Distress Symptoms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |||||||
| β, B (SE) | p | β, B (SE) | p | β, B (SE) | p | β, B (SE) | p | β, B (SE) | p | β, B (SE) | p | |
| Male | −.17, −0.29 (0.22) | .20 | −.15, −0.25 (0.22) | .25 | −.06, −0.11 (0.22) | .62 | −.31, −0.49 (0.20) | .02 | −.27, −0.43 (0.20) | .03 | −.12, −0.19 (0.18) | .29 |
|
| ||||||||||||
| Age | .10, 0.01 (0.02) | .53 | .18, 0.03 (0.02) | .26 | .25, 0.03 (0.03) | .21 | .007, <0.001 (0.02) | .98 | .11, 0.02 (0.02) | .45 | .11, 0.01 (0.02) | .50 |
|
| ||||||||||||
| Genocide Violence Exposure | .36, 0.07 (0.03) | .009 | .17, 0.03 (0.03) | .26 | .23, 0.04 (0.02) | .07 | −.03, −0.01 (0.02) | .80 | ||||
|
| ||||||||||||
| Witnessing Family Attacked | .03, 0.05 (0.24) | .83 | .05, 0.09 (0.23) | .72 | .17, 0.27 (0.22) | .22 | .26, 0.42 (0.19) | .04 | ||||
|
| ||||||||||||
| Return to School | .22, 0.38 (0.35) | .29 | −.12, −0.23 (0.29) | .42 | ||||||||
|
| ||||||||||||
| Educational Attainment | −.47, −0.24 (0.12) | .05 | −.24, −0.11 (0.10) | .25 | ||||||||
|
| ||||||||||||
| Poverty | .08, 0.31 (0.67) | .65 | .24, 0.86 (0.56) | .13 | ||||||||
|
| ||||||||||||
| Social Support | −.10, −0.15 (0.19) | .45 | −.30, −.42 (.16) | .01 | ||||||||
|
| ||||||||||||
| R2 | .04 | .17 | .33 | .10 | .19 | .46 | ||||||
| Adjusted R2 | .01 | .11 | .23 | .07 | .14 | .38 | ||||||
| Wald Test | 4.07 p=.02 | 2.57, p<.05 | 3.15, p=.05 | 5.48, p=.001 | ||||||||
A mediation analysis was conducted to assess whether Educational Attainment mediated the association between Genocide Violence Exposure and PTSD Symptoms (see Figure 1). Gender and Age were included as covariates. Results indicated that Genocide Violence Exposure predicted PTSD Symptoms (Path c; B=0.08, SE=0.02, p=.002). When Educational Attainment was added as a mediator in the model, Genocide Violence Exposure predicted Educational Attainment (Path a; B=−0.15, SE=0.05, p=.005) and Educational Attainment predicted PTSD Symptoms (Path b; B=−0.14, SE=0.06, p=.03). This indirect effect was significant, as the indirect effect estimate’s 95% bias-corrected bootstrapped standard error confidence intervals (CIs) did not contain zero (B=0.02, 95% CIs=0.002–0.05). After including Educational Attainment as a mediator, Genocide Violence Exposure was reduced but still predicted PTSD Symptoms (Path c′; B=0.06, SE=0.02, p=.02). Therefore, Educational Attainment partially mediated the association between Genocide Violence Exposure and PTSD Symptoms.
Figure 1.
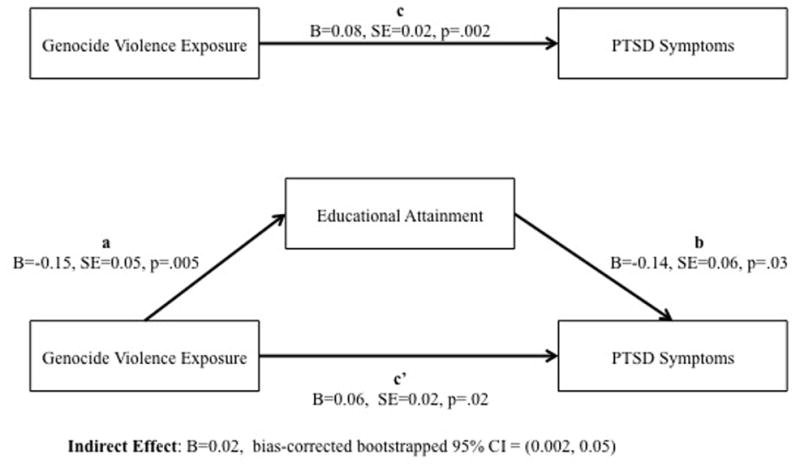
Educational Attainment Mediating the Association Between Genocide Violence Exposure and PTSD Symptoms
Note. Regressions controlled for covariates of Gender and Age. In the mediation model male gender positively predicted Educational Attainment (B=0.99, SE=0.43, p=.02). Gender and Age did not significantly predict any other variables in the models.
While we hypothesized that Educational Attainment would mediate the association between Genocide Violence Exposure and PTSD Symptoms, it is also possible that PTSD Symptoms mediate the association between Genocide Violence Exposure and Educational Attainment. To assess this possibility, follow-up mediation analyses were conducted. Results indicated that the indirect effect was significant (B= −0.05, 95% CI= −0.13 to −0.005), supporting this alternate hypothesis.
Prediction of distress symptoms
Results of the nested regressions indicated that in models one and two, Gender predicted Distress Symptoms (β=−.31, p=.02; β=−.27, p=.03 respectively), such that women reported greater distress than men (see Table 5). However, in the final model, Gender no longer significantly predicted Distress Symptoms (β=−.12, p=.29). Genocide Violence Exposure was trending towards significance in model two (β=.23, p=.07), but when post-genocide factors were added in model three, it was not significant (β=−.03, p=.80), and there was better model fit (Wald Test=5.48, p=.001). In contrast, Witnessing Family Attacked was not significant in model two (β=.17, p=.22), but was significant in model three after the post-genocide risk factors were included (β=.26 p=.04). In addition, Social Support negatively predicted Distress Symptoms (β=−.30, p=.01). No other predictors were significant in model three. The final model accounted for 38% of the variance in distress.
Although Witnessing Family Attacked was not significant until Social Support was added to the model, mediation analyses were conducted to assess whether Social Support was acting as a suppressor of the association between Witnessing Family Attacked and Distress Symptoms. Results of suppression analyses that included Gender and Age as covariates indicated that the indirect effect was not significant, since the 95% bias-corrected bootstrapped CIs contained zero (B=−0.03, 95% CIs= −0.19 to 0.11), so suppression was not present.
Discussion
Fourteen years after the genocide, OHH in this study reported considerable ongoing difficulties, including low social support, high levels of poverty, and high rates of PTSD and distress symptoms. The 60% of participants who reported in 2002 that they witnessed their family members being attacked during the genocide reported more distress in 2008 than participants who did not witness their family members being attacked. Additionally, participants who reported less social support in 2008 reported more distress. Although poverty was clearly a problem for these OHH, it did not directly predict distress or PTSD symptoms.
While exposure to genocide events reported in 2002 had a positive dose-response relationship with PTSD symptoms in 2008, this association was partially mediated by lower educational attainment in 2008. Education emerged as one of the most potentially valuable protective factors following the genocide. Despite the many difficulties facing these survivors, 90% of them managed to complete primary school (6th grade), while 46% completed secondary school (12th grade). Education may be beneficial because it may offer hope and the possibility of a brighter future to OHH. In addition, going to school is one of the primary normative experiences for children, and for OHH who are suddenly thrust into the adult roles of caregiver and breadwinner, education may offer an opportunity for success in a developmentally appropriate everyday role, as well as providing access to concerned adults. Indeed, education certainly appears to be extremely important to many of the OHH in this sample, who on average achieved higher educational levels than similarly aged youth in Rwanda (Akresh & De Walque, 2008).
The difference in education between Rwandan youth overall and the OHH in this sample may stem in part from the fact that the OHH in this sample were members of a grassroots community organization dedicated to assisting OHH, and may therefore have had better access to education than other youth in Rwanda. Moreover, qualitative interviews revealed that many participants received educational assistance from the Rwandan government’s National Assistance Fund for Survivors of Genocide (Fond d’Assistance pour les Rescapes du Genocide: FARG). It seems that the assistance it provided may have been essential to helping the OHH with pursuing their educational goals, and in turn, that educational attainment may have resulted in lower PTSD symptoms years later. Programs that help orphaned survivors of war access education by providing transportation, uniform fees, school materials, and assistance with applying to and paying for higher education may reduce PTSD symptoms.
While many OHH in this study succeeded in gaining education, almost none reported having substantial social support. Despite this limited range, social support was still a highly significant predictor of distress. Social support as measured in this study refers to the perception of having someone to turn to when things bother you, when you are sick, and when you need advice or help making decisions, and having someone around whom you trust, feel close too, and who understands your feelings. OHH who have even one person in their lives who provides this support may indeed be much better off than those who report having none. For war-affected populations, efforts to strengthen and expand social support networks, such as promoting community groups of others with shared experiences, developing mentoring networks, and continuing efforts to reconnect fragmented families may also decrease distress. The goals of social support interventions may not need to be lofty, because the results suggest that even a small change may be beneficial. Indeed, there is some evidence that distress decreases in Rwandans receiving interventions designed to improve social cohesion and bonding (Brown et al., 2009; Scholte et al., 2011).
While the findings are consistent with studies which have found that psychological distress in war-affected populations is often more associated with daily stressors than with war exposures (Miller, Omidian, Rasmussen, Yaqubi, & Daudzai, 2008; Miller & Rasmussen, 2010), post-genocide risk factors and mental health symptoms were both assessed in 2008, and therefore directionality cannot be inferred. Results of the follow-up mediation analyses found that PTSD symptoms may also mediate the association between genocide violence exposure and educational attainment. While further research is needed on the directionality of the association of these variables, the results of this study support the association between PTSD symptoms and education and between distress and social support.
For many war survivors, public health interventions that improve social support and education may significantly reduce distress and PTSD symptoms, but for some survivors, particularly those who have witnessed their family members and loved ones being harmed, interventions for mood and anxiety disorders may also be beneficial. In addition to increased understanding of the efficacy of interventions for depression and anxiety, research is needed on the effectiveness of existing local community-based approaches to addressing risk factors and mental health needs. Not only may these approaches be more culturally-relevant for war survivors, but they may also be more sustainable than imported interventions.
Limitations and strengths
This study has a number of limitations. The findings may not be generalizable to other OHH in Rwanda because the participants were members of an orphan organization, were selected by the organization leadership and, thus, were not a random sample of OHH. Additionally, the fact that all participants in this study had given genocide testimony may have had an impact on the mental health outcomes reported here, as studies have found that providing narrative accounts of traumatic experiences can reduce PTSD symptoms (Bisson & Andrew, 2009). Therefore results must be interpreted with caution. The study has a small sample size, which may mean the analyses are underpowered. Although coding of the genocide testimonies was reported in a more naturalistic and personal way than a checklist approach, genocide experiences were reported retrospectively with little prompting, and may not be complete. While the process for translating assessment instruments involved having measures reviewed and approved by OHH in focus groups and by board members, and having the measures forward and back translated by native Kinyarwanda speakers and approved by a different set of OHH, the measures did not undergo formal pre-testing and cognitive interviewing as suggested by the World Health Organization (World Health Organization, 2014). Finally, educational attainment was used as a continuous variable, and while using ordinal variables coded into five or more categories as continuous variables has been supported in the literature (Beauducel & Herzberg, 2006; DiStefano, 2002; Rhemtulla, Brosseau-Liard, & Savalei, 2012), it is possible that this created some bias in the parameter estimates.
Despite these limitations, this study also has a number of strengths. The use of two time points allowed for prediction of risk and outcome variables from reported genocide exposure and a long separation between the reporting of distressing information about the genocide and the collection of information on mental health. Additionally, the study not only used a standardized measure with strong established psychometric properties (IES-R), but also a measure developed locally for this population (Symptom Checklist), to assess mental health symptoms, thereby increasing the likelihood of cultural relevance and appropriateness of the assessments (Bolton, 2001a; Jayawickreme, Jayawickreme, Atanasov, Goonasekera, & Foa, 2012). Finally, this study was conducted with the full collaboration and participation of an association of OHH, which helped increase the cultural relevance and sensitivity of the study and ensured that the questions being asked were meeting the specific needs of their membership.
Conclusion
These results provide support for the hypothesis that education and social support may play important roles in mental health of genocide survivors, and may even contribute more to PTSD and distress symptoms than war exposures. While experiences that occurred during the genocide cannot be altered, these post-genocide factors may be targets of change for interventions and may be used to identify individuals at higher risk of poor mental health outcomes. Results suggest that public health and community efforts to improve educational outcomes and strengthen and expand social support networks may improve mental health outcomes of OHH. In addition, secondary and tertiary interventions such as depression and anxiety interventions may be beneficial for a subset of OHH who have witnessed harm to family members. Taken together, these findings highlight possible directions for post-genocide psychosocial and public health intervention programs to improve the mental health of OHH in Rwanda. The resilience shown by these young survivors in obtaining education and raising their families even after facing horrifying genocidal experiences suggests that such interventions may be valuable and welcomed.
Acknowledgments
We wish to thank the Rwandan Association des Orphelins Chefs de Ménages, for their commitment to unifying, strengthening, and bringing hope to children orphaned by the 1994 Rwandan Genocide against the Tutsi. This project was funded by grants from the Rosenzweig-Coopersmith Foundation and the Office of the Provost at the University of Southern California to Dr. Meyerowitz. Dr. Ng’s time was partially supported by the National Institute of Mental Health (#s 5T32MH093310 and 5R34MH084679).
References
- Akresh R, De Walque D. World Bank Policy Research Working Paper. 2008. Armed conflict and schooling: Evidence from the 1994 Rwandan genocide; p. 4606. [Google Scholar]
- Beauducel A, Herzberg PY. On the performance of maximum likelihood versus means and variance adjusted weighted least squares estimation in CFA. Structural Equation Modeling. 2006;13:186–203. doi: 10.1207/s15328007sem1302_2. [DOI] [Google Scholar]
- Bolton P. Cross-cultural validity and reliability testing of a standard psychiatric assessment instrument without a gold standard. Journal of Nervous and Mental Disease. 2001a;189:238–242. doi: 10.1097/00005053-200104000-00005. [DOI] [PubMed] [Google Scholar]
- Bolton P. Local perceptions of the mental health effects of the Rwandan genocide. Journal of Nervous and Mental Disease. 2001b;189:243–248. doi: 10.1097/00005053-200104000-00006. [DOI] [PubMed] [Google Scholar]
- Boris NW, Brown LA, Thurman TR, Rice JC, Snider LM, Ntaganira J, Nyirazinyoye LN. Depressive symptoms in youth heads of household in Rwanda: correlates and implications for intervention. Archives of Pediatrics and Adolescent Medicine. 2008;162:836–843. doi: 10.1001/archpedi.162.9.836. [DOI] [PubMed] [Google Scholar]
- Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, MA: The Harvard University Press; 1979. [Google Scholar]
- Brown L, Thurman TR, Rice J, Boris NW, Ntaganira J, Nyirazinyoye L, Snider L. Impact of a mentoring program on psychosocial wellbeing of youth in Rwanda: Results of a quasi-experimental study. Vulnerable Children and Youth Studies. 2009;4:288–299. doi: 10.1080/17450120903193915. [DOI] [Google Scholar]
- Cohen MH, Fabri M, Cai X, Shi Q, Hoover DR, Binagwaho A, Anastos K. Prevalence and predictors of posttraumatic stress disorder and depression in HIV-infected and at-risk Rwandan women. Journal of Women’s Health. 2009;18:1783–1791. doi: 10.1089/jwh.2009.1367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creamer M, Bell R, Failla S. Psychometric properties of the Impact of Event Scale - Revised. Behaviour Research and Therapy. 2003;41:1489–1496. doi: 10.1016/j.brat.2003.07.010. [DOI] [PubMed] [Google Scholar]
- DiStefano C. The impact of categorization with confirmatory factor analysis. Structural Equation Modeling. 2002;9:327–346. doi: 10.1207/S15328007SEM0903_2. [DOI] [Google Scholar]
- Dyregrov A, Gupta L, Gjestad R, Mukanoheli E. Trauma exposure and psychological reactions to genocide among Rwandan children. Journal of Traumatic Stress. 2000;13:3–21. doi: 10.1023/A:1007759112499. [DOI] [PubMed] [Google Scholar]
- Fernando G, Miller K, Berger D. Growing pains: The impact of disaster-related and daily stressors on the mental health and psychosocial functioning of youth in Sri Lanka. Child Development. 2010;81:1192–1210. doi: 10.1111/j.1467-8624.2010.01462.x. [DOI] [PubMed] [Google Scholar]
- Hallgren KA. Computing inter-rater reliability for observational data: An overview and tutorial. Tutorials in quantitative methods for psychology. 2012;8:23. doi: 10.20982/tqmp.08.1.p023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harel O. The estimation of R 2 and adjusted R 2 in incomplete data sets using multiple imputation. Journal of Applied Statistics. 2009;36:1109–1118. doi: 10.1080/02664760802553000. [DOI] [Google Scholar]
- Heptinstall E, Sethna V, Taylor E. PTSD and depression in refugee children. European Child and Adolescent Psychiatry. 2004;13:373–380. doi: 10.1007/s00787-004-0422-y. [DOI] [PubMed] [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp; 2010. [Google Scholar]
- Jayawickreme N, Jayawickreme E, Atanasov P, Goonasekera MA, Foa EB. Are culturally specific measures of trauma-related anxiety and depression needed? The case of Sri Lanka. Psychological Assessment. 2012;24:791–800. doi: 10.1037/a0027564. [DOI] [PubMed] [Google Scholar]
- Layne CM, Olsen JA, Baker A, Legerski JP, Isakson B, Pašalić A. Unpacking trauma exposure risk factors and differential pathways of influence: Predicting post-war mental distress in Bosnian adolescents. Child Development. 2010;81:1053–1076. doi: 10.1111/j.1467-8624.2010.01454.x. [DOI] [PubMed] [Google Scholar]
- Miller KE, Omidian P, Rasmussen A, Yaqubi A, Daudzai H. Daily stressors, war experiences, and mental health in Afghanistan. Transcultural Psychiatry. 2008;45:611–638. doi: 10.1177/1363461508100785. [DOI] [PubMed] [Google Scholar]
- Miller KE, Rasmussen A. War exposure, daily stressors, and mental health in conflict and post-conflict settings: bridging the divide between trauma-focused and psychosocial frameworks. Social Science and Medicine. 2010;70:7–16. doi: 10.1016/j.socscimed.2009.09.029. [DOI] [PubMed] [Google Scholar]
- Munyandamutsa N, Nkubamugisha PM, Gex-Fabry M, Eytan A. Mental and physical health in Rwanda 14 years after the genocide. Social Psychiatry and Psychiatric Epidemiology. 2012;47:1753–1761. doi: 10.1007/s00127-012-0494-9. [DOI] [PubMed] [Google Scholar]
- Netland M. Assessment of exposure to political violence and other potentially traumatizing events. A critical review. Journal of Traumatic Stress. 2001;14:311–326. doi: 10.1023/A:1011164901867. [DOI] [PubMed] [Google Scholar]
- Netland M. Event-list construction and treatment of exposure data in research on political violence. Journal of Traumatic Stress. 2005;18:507–517. doi: 10.1002/jts.20059. [DOI] [PubMed] [Google Scholar]
- Neuendorf KA. The content analysis guidebook. Thousand Oaks, CA: Sage Publications; 2002. [Google Scholar]
- Neugebauer R, Fisher PW, Turner JB, Yamabe S, Sarsfield JA, Stehling-Ariza T. Post-traumatic stress reactions among Rwandan children and adolescents in the early aftermath of genocide. International Journal of Epidemiology. 2009;38:1033–1045. doi: 10.1093/ije/dyn375. [DOI] [PubMed] [Google Scholar]
- Ng LC, Ahishakiye N, Miller DE, Meyerowitz BE. Psychological Trauma: Theory, Research, Practice and Policy. Narrative Characteristics of Genocide Testimonies Predict Posttraumatic Stress Disorder Symptoms Years Later. (In Press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pham PN, Weinstein HM, Longman T. Trauma and PTSD symptoms in Rwanda: implications for attitudes toward justice and reconciliation. JAMA. 2004;292:602–612. doi: 10.1001/jama.292.5.602. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers. 2004;36:717–731. doi: 10.3758/BF03206553. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/BRM.40.3.879. [DOI] [PubMed] [Google Scholar]
- Republic of Rwanda. History. 2014 Retrieved January 13, 2015, from http://www.gov.rw/home/history/
- Rhemtulla M, Brosseau-Liard PE, Savalei V. When can categorical variables be treated as continuous? A comparison of robust continuous and categorical SEM estimation methods under suboptimal conditions. Psychological Methods. 2012;17:354. doi: 10.1037/a0029315. [DOI] [PubMed] [Google Scholar]
- Saltzman WR, Layne CM, Steinberg AM, Arslanagic B, Pynoos RS. Developing a culturally and ecologically sound intervention program for youth exposed to war and terrorism. Child and Adolescent Psychiatric Clinics of North America. 2003;12:319–342. doi: 10.1016/s1056-4993(02)00099-8. [DOI] [PubMed] [Google Scholar]
- Schaal S, Dusingizemungu J-P, Jacob N, Elbert T. Rates of trauma spectrum disorders and risks of posttraumatic stress disorder in a sample of orphaned and widowed genocide survivors. European journal of psychotraumatology. 2011;2 doi: 10.3402/ejpt.v2i0.6343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaal S, Elbert T. Ten years after the genocide: trauma confrontation and posttraumatic stress in Rwandan adolescents. Journal of Traumatic Stress. 2006;19:95–105. doi: 10.1002/jts.20104. [DOI] [PubMed] [Google Scholar]
- Schaal S, Weierstall R, Dusingizemungu JP, Elbert T. Mental health 15 years after the killings in Rwanda: Imprisoned perpetrators of the genocide against the Tutsi versus a community sample of survivors. Journal of Traumatic Stress. 2012;25:446–453. doi: 10.1002/jts.21728. [DOI] [PubMed] [Google Scholar]
- Scholte WF, Verduin F, Kamperman AM, Rutayisire T, Zwinderman AH, Stronks K. The effect on mental health of a large scale psychosocial intervention for survivors of mass violence: a quasi-experimental study in Rwanda. PloS One. 2011;6:e21819. doi: 10.1371/journal.pone.0021819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schweitzer R, Melville F, Steel Z, Lacherez P. Trauma, post-migration living difficulties, and social support as predictors of psychological adjustment in resettled Sudanese refugees. Australian and New Zealand Journal of Psychiatry. 2006;40:179–188. doi: 10.1080/j.1440-1614.2006.01766.x. [DOI] [PubMed] [Google Scholar]
- Sherbourne CD, Stewart AL. The MOS social support survey. Social Science and Medicine. 1991;32:705–714. doi: 10.1016/0277-9536(91)90150-B. [DOI] [PubMed] [Google Scholar]
- StataCorp. Stata Statistical Software: Release 12 (Version 12) College Station, TX: StataCorp LP; 2011. [Google Scholar]
- The United Nations Children’s Fund. The State of the World’s Children 1996. New York: United Nations Children’s Fund; 1996. [Google Scholar]
- The United Nations Children’s Fund. Africa’s Orphaned Generations. New York: United Nations Children’s Fund; 2003. [Google Scholar]
- Thurman TR, Snider L, Boris N, Kalisa E, Nkunda Mugarira E, Ntaganira J, Brown L. Psychosocial support and marginalization of youth-headed households in Rwanda. AIDS Care. 2006;18:220–229. doi: 10.1080/09540120500456656. [DOI] [PubMed] [Google Scholar]
- Ward LM, Eyber C. Resiliency of children in child-headed households in Rwanda: implications for community based psychosocial interventions. Intervention. 2009;7:17–33. doi: 10.1097/WTF.0b013e32832ad3ac. [DOI] [Google Scholar]
- Weiss D, Marmar C. The Impact of Event Scale-Revised. In: Keane T, editor. Assessing psychological trauma and PTSD. New York: Guilford; 1997. pp. 399–411. [Google Scholar]
- World Health Organization. Process of translation and adaptation of instruments. 2014 Retrieved August 26, 2014, 2014, from http://www.who.int/substance_abuse/research_tools/translation/en/