
Fig. 2.
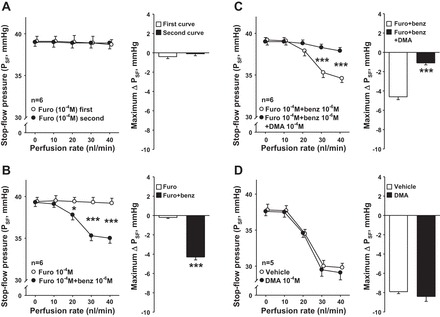
A: time control experiments with furosemide treatment. Left: in the presence of the NKCC2 blocker furosemide, PSF remained unchanged in a reproducible manner while increasing the perfusion rates 2 consecutive times in the late proximal tubule (○, first curve; ●, second curve). Right: maximum PSF responses in the first and second curves. B: effect of inhibiting TGF and connecting tubuloglomerular feedback (CTGF) simultaneously on a TGF-like response. Left: in the presence of furosemide (○), adding epithelial Na channel (ENaC) blocker benzamil (benz; ●) caused PSF to decrease in response to increasing the nephron perfusion, suggesting that when NKCC2 and CTGF are both blocked there is an additional constrictor phenomenon initiated in the nephron. Right: maximum PSF responses in the furosemide and furosemide+benzamil curves. *P < 0.05, ***P < 0.001. C: effect of Na/H exchanger (NHE) inhibition on PSF in the absence of TGF and CTGF. Left: in the presence of furosemide and benzamil (○), adding NHE blocker dimethylamiloride (DMA; ●) prevented the decrease in PSF in response to increasing the nephron perfusion, suggesting that when TGF and CTGF are blocked, NHE can induce a TGF-like response. Right: maximum PSF responses in the furosemide+benzamil and furosemide+benzamil+DMA curves. ***P < 0.001. D: effect of NHE blocker DMA on PSF. Left: increasing the perfusion rates in the late proximal tubule decreased PSF (○, vehicle). Addition of NHE blocker DMA (●) did not affect the PSF response induced by increasing the perfusion rates. Right: maximum PSF responses in vehicle and DMA curves.