

Abstract
Calcium alginate has been proved to favor the skin ulcer healing and collagen synthesis was a critical factor for the wound closure. The present study was to elucidate the mechanism of calcium alginate on the diabetes skin ulceration. Calcium alginate dressing was applied daily on the full-thickness exercising wound created on the back of diabetic rat model as Alg-group (n=6), and the vaseline dressing was used as control (n=6). Rats were respectively sacrificed and the wound tissues were removed and used for the evaluation of various biochemical analysis contained collagen (type I and III) by Western blotting and hydroxyproline level changes by ELISA assay at 3 d, 7 d and 14 d after wounding. The expression of skin collagen I in Alg-group was enhanced from day 3 (0.66±0.25 vs. 0.42±0.09, P<0.05) to day 14 (1.09±0.14 vs. 0.78±0.16, P<0.05). However, no significant difference of collagen III expression was found between two groups during wound healing (P>0.05). And the ratio of collagen I/III in Alg-group was greater than that of Vas-group at day 7 (1.07±0.31 vs. 0.77±0.11, P<0.05) and 14 (1.18±0.30 vs. 0.83±0.14, P<0.05). The hydroxyproline level in skin homogenate of Alg-group was higher than that of Vas-group from day 3 (30.29±0.92 ng/ml vs. 27.52±0.83 ng/ml, P<0.05) to day 14 (89.58±4.97 ng/ml vs. 79.30±4.42 ng/ml, P<0.05). Calcium alginate accelerates the process of wound healing through improving type I collagen synthesis and increasing ratio of collagen I/III in diabetic rats.
Keywords: Calcium alginate, diabetic wound, collagen type I/III
Introduction
The prevalence of diabetes has increased enormous world-wide; its complications became serious threats for public health [1,2]. One of these most severe complications is the delaying and refractory foot ulcerations [3,4]. The normal wound healing process involves consecutive interactions of many different cell types. Inflammation, proliferation, angiogenesis, epithelialization, matrix remodeling, and scar maturation are the consequence of several basic processes [5]. This complex sequence starts from the moment of injury and continues for different periods, and the time period depending on the health status of the injured individual and the extent of the wound area [6]. The reduction of extracellular matrix, cell and growth factor of tissue related to normal wound-repair process will be a vital contributing factor to the poor healing of diabetic wound [3].
Collagen fiber is the main component of the extracellular matrix of tissues and is the most abundant protein in skin tissue, and optimum deposition of collagen type I and III with their proper ratio is essential during connective tissue formation and to prevent scarring [7]. Collagen I is responsible for higher tensile strength, while collagen III is mainly found in early wound healing stages [8], and they keep a particular ratio in healthy skin [9]. The distribution of collagen fiber and their optimum ratio are critical to maintain required crosslinked density and mechanical toughness during the wound healing process [10]. Thus, the increase and stabilization of collagen fiber are of great impact on the healing of diabetic wound.
Since 1980s, numerous wound healing dressings constituted with natural polymers such as alginate, chitosan, have been developed to promote the diabetic wound healing [11,12]. Alginate, a natural herbal polymer, was a family of linear copolymer that contains two uronic acids, β-(1-4)-linked D-mannuronic acid (M) and α-(1-4)-linked L-guluronic acid (G) [13]. Divalent cations, such as Ca2+, can interact with alginate polymer chains to form a gel structure. These structures are composed by each divalention interacting with two contiguous G-residues, or with two G-residues in an opposing chain [14]. Calcium alginate is used in the fabrication of wound dressings due to its excellent water-absorbing quality, biodegradation, biocompatibility and outstanding film forming properties [15]. However, to our knowledge, little is known about the alteration of collagen and the ratio of its different type in the diabetic wound during the calcium alginate dressing therapy, particularly the changes of ratio of collagen I and III. Therefore, the aim of the present study was to clarify whether the protective effect of calcium alginate on the diabetic ulcer has some connection with the change of collagen type I and III in diabetic rats.
Materials and methods
Materials
Calcium alginate dressing was supplied by Shangdong Yinuo Biotechnology Co., Ltd, Shandong, China, and the alginate extracted from Laminaria hyperborean. Vaseline dressing was purchased from Sigma-Aldrich USA The supplied dressings were cut to suitable sizes and sterilized by gamma irradiation before dressing change. The mouse fibroblast cell line (L929) was purchased from the Cellular Biology Institute of the Chinese Academy of Sciences, Shanghai, China.
Cytotoxicity of calcium alginate
The cytotoxicity assay was performed as described by Adetutu et al [16]. The ascending concentrations of the extracted liquid of the materials were prepared in serial dilutions ranging from 0 to 12.0 mg/ml (0, 6.0, 12.0 mg/ml). Mouse fibroblast cells (L929) were plated individually in 96-well plates with 400 μl of DMEM above the previously sterilized (UV light for 30 min) biomaterials. 40 μl of 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) solution (5 mg/ml) was added to each well after 0, 12, 24 and 48 h incubation. The plates were further incubated at 37°C for 1 h in an incubator containing 5% CO2. 300 μl of acidic isopropanol (0.04 N HCl in isopropanol) was added after this period. Quantification was processed using an ELISA automatic microplate reader (SLT, Austria) with a reference wavelength of 450 nm. Each sample was examined in thrice.
Establishment of diabetic wound and treatment with calcium alginate dressing
Thirty-six healthy male Sprague-Dawley rats, 8 weeks old and weighting 220 g to 250 g, were purchased from the Animal Breeding Center in Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University (Shanghai, China). They were given a single i.p injection of 55 mg/kg STZ dissolved in sodium citrate buffer (pH 4.5) to establish the diabetes model. Blood glucose collected from rat tail-vein was monitored using Blood Glucose monitor (LifeScan Inc. Milpitas, CA) 3 days later. STZ-treated rats with blood glucose levels exceeded 16.7 mM were considered diabetic. This study was carried out on the basis of the criteria outlined in the “Guide for the Care and Use of Laboratory Animals”, Institute of Laboratory Animal Resources, National Research Council. The full-thickness exercise wound was prepared in these rats at 1 month after the onset of diabetes. The animals were randomly divided into two groups (Alg group and Vas group) with 18 rats each, then each group was assigned into three subgroups based on their sacrificed time (named 3, 7 and 14 day group, n=6 each group). They were etherized for anesthesia, the dorsal surface of the rat was hair removed by electrical hair cutter. Then a 20 mm×20 mm full-thickness wound was created by excising the dermis and epidermis. Calcium alginate dressings were applied to cover the wound beds as Alg-group, wound treated with vaseline dressing alone (Vas-group) as control. The wound dressings were changed every day, the wound size was record daily, and wound lesion appearance was collected by photographing at a close and fixed distance at day 0, 3, 7 and 14, wound closure rate was calculated using the following formula: Wound closure rate (%)=[Wound area (day 0-day t)/Wound area day 0]×100%. Rats were respectively sacrificed at day 3, 7 and 14, a half of skin tissue within wound area or 10 mm beside the wound were collected and stored in refrigerator at -80°C for future assay, and the other half wound skin was prepared in 10% neutral buffered formalin for histopathological observation.
Histopathological analysis
For histopathogical analysis, the moiety of the skin tissue samples prepared in 10% neutral buffered formalin was embedded in paraffin, and was cut into 3 μm thickness slices for histopathological examination through hematoxylin/eosin (H&E) staining. For collagen formation by Masson’s trichrome staining, the tissue sections were deparaffinized and redehydrated and then stained followed the instruction of Masson’s Trichrome Staining kit. The stained sections were observed with a Nikon YS100 microscope with a DXM 1200F digital camera (Nikon, Japan). And the Image-pro Plus 6.0 software was used to test the collagen density with the pathological section.
Western blotting for type I and III collagen expression
The skin tissue of wound area for type I and III collagen were assayed by Western blot [17]. The skin tissue representing an equal quantity of type I and III collagen were resolved by 8% SDS-PAGE under non-reducing conditions and transformed to nitrocellulose membranes. Five percent non-fat milk solution in Tris-buffered with 0.1% Tween (TTBS) was used to block the membranes for 1 hour at room temperature. Then they were incubated with a mouse antibody to rodent type I or III collagen (1:10,000 dilution, Abcam Inc., Cambridge, MA) in the same buffer overnight at 4°C. Following this, the membranes were washed with TTBS and the Phototope-HRP western detection kit (Cell Signaling Technologies, Inc., Danvers, MA) was used to detect bound antibody. Signal intensity was quantified by image analyzer (Image J). And the ratio of collagen I to collagen III was calculated using the following formula: ratio of collagen I to collagen III=expression levels of collagen I/collagen III×100%.
ELISA assay for hydroxyproline concentrations
Enzyme-linked immunosorbent assay (ELISA) was used to evaluate hydroxyproline level. In brief, the new skin and granulation tissue of wound area or 10 mm beside the wound at day 3, 7, and 14 was pulverized in chilled lysis buffer containing 100 mM Tris-HCl, 0.05 mM EDTA with the help of ice-cold pestle and mortar and a pinch of glass wool. They were transferred to 1.5 ml microcentrifuge tubes and centrifuged for 10 min after the tissue were thoroughly pulverized into a homogenous mixture, then a supernatant protein lysate was collected and ELISA was conducted according to the manufacturer’s instructions.
Statistical analysis
The results are expressed as means ± S.D. Statistically significant difference of cytotoxicity and wound closure area were determined using two-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison tests, the expression of collagen levels and the ratio of collagen I/III were compared with paired or unpaired student t test using the SPSS 17.0 software. Difference was considered to be statistically significant if P<0.05.
Results
Calcium alginate exhibits no cytotoxicity
In this study, mouse fibroblast cells (L929) grew well in the extracted liquid of materials for 48 h (Figure 1). As the cells viability in the all groups (the concentrations of extracted liquid of material were 6.0 and 12.0 mg/ml) were identical to those (without material) in controls (P>0.05).
Figure 1.
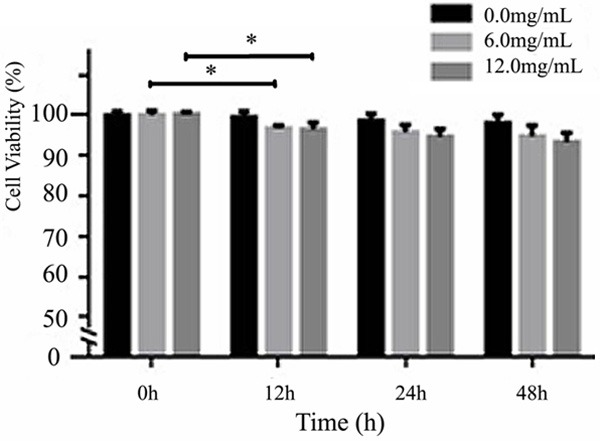
Cytotoxicity effects of calcium alginate. The cell viability in the all groups (the concentrations of extracted liquid of material were 6.0 and 12.0 mg/ml) were identical to those (without material) in controls (P>0.05), there was a significant difference in the cell viability between 0 h and 12 h in the groups which the concentrations were 6.0 and 12.0 mg/ml (P<0.05). *P<0.05 when compared with the different periods in the same group.
Calcium alginate accelerated wound closure rate
Figure 2A showed representative photographs of wounds covered with alginate or vaseline spot at days 0, 3, 5, 7 and 14 after wounding. Wound size in all groups was calculated from post-surgery on days 0, 2, 4, 6, 8, 10, 12 and 14. And the wound closure rate in the Alg-group was dramatically increased compared with the Vas-group from day 4 (Figure 2B, P<0.05).
Figure 2.
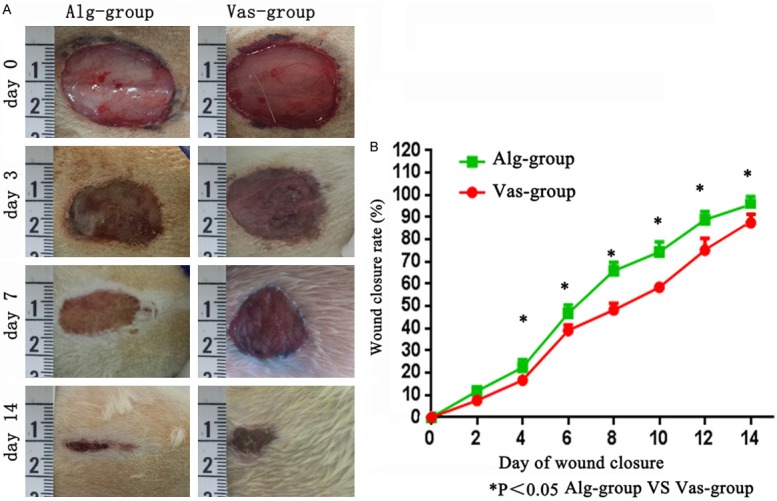
Change of wound size in the calcium alginate and vaseline groups. Representative photographs of wounds covered with alginate or Vaseline spot at days 0, 3, 5, 7 and 14 taken postoperatively (A). The wound closure rate in the alginate-treated group was increased more rapidly compared with Vaseline-treated group (B). Alg-group: Alginate-treated group, Vas-group: Vaseline-treated group. *P<0.05 when compared with the corresponding controls.
Calcium alginate treated wound skin possessed a milder inflammation and a faster epithelization
As shown in Figure 3A, on 3rd postoperative day, calcium alginate treated wounds healed with densely cell deposited matrix with abundant organized cells embedded, the inflammation was mild and moderate. While the cell deposited matrix in control wounds was relatively infrequent, with cells presented as less organized, and the inflammation was serious. On 7th day, skin in wound areas of Alg group was not completely epithelized, but inward epithelial growth was sustained. Also, epithelization irregularly started under wound crust in Vas-group. On 14th day, the epithelization in the calcium alginate group finished. However, in the Vas-group, the wound surface was covered with an incomplete layer of epidermis (Figure 3B) at 14th day after wound establishment.
Figure 3.

Histological observation of wounds treated with calcium alginate and vaseline dressing. Each wound of rat on day 3, 7 and 14 was representative of six wounds covered with Calcium alginate (A) and Vaseline (B). Masson’s Trichrome staining of wound treated with calcium alginate or vaseline (C). The collagen density in Alg-group was far more than it in Vas-group on day 3, 7, and 14 post-operation (D). Alg-group: Alginate-treated group, Vas-group: Vaseline-treated group. *P<0.05 when compared with the corresponding controls. #P<0.05 when compared with the different periods in the same group.
Calcium alginate promoted the expression of total collagen in new wound skin tissue
Masson’s trichrome staining of 3, 7 and 14 day postoperative wound granulation tissue described the clearer picture of wound healing. In Alg-group, increased fibroblast density and higher collagen deposition were found, while in control group the complete re-epithelialization with only minor to moderate fibroblast density and irregular packing of collagen fibers were observed from day 3 sustained to day 14 (Figure 3C). By the collagen density comparison, the total collagen staining in Alg-group was slightly higher than control group at day 3 (522.00±11.10 μm2 vs. 513.33±8.16 μm2, P>0.05), and it enhanced dramatically at day 7 (687.67±60.78 μm2 vs. 558.67±14.69 μm2, P<0.05), and kept a high-expression levels till day 14 (754.17±20.43 μm2 vs. 649.17±36.52 μm2, P<0.05) (Figure 3D).
Calcium alginate increased the collagen type I expression and ratio of collagen I/III
Western blotting depicted significant elevating expression of collagen type I and III in calcium alginate treated wound granulation tissue (Figure 4). Collagen I in Alg-group significantly increased compared to the Vas-group at day 3 (0.66±0.25 vs. 0.42±0.09, P<0.05), day 7 (0.84±0.17 vs. 0.62±0.10, P<0.05) and day 14 (1.09±0.14 vs. 0.78±0.16, P<0.05) (Figure 4A). In contrast, there is no statistically significant difference in collagen III expression between two groups from day 3 to day 14 (Figure 4B). And the subsequent calculated ratio of collagen I to collagen III in Alg-group was higher significantly than that in Vas-group at day 7 (1.07±0.31 vs. 0.77±0.11, P<0.05), and day 14 (1.18±0.30 vs. 0.83±0.14, P<0.05) (Figure 4C).
Figure 4.

The expression of collagen I and III, ratio of collagen I/III and hydroxyproline in Alg-group and Vas-group on the day 3, 7 and 14. (A) Expression of Collagen I in different time of wound establishment. (B) Expression of Collagen III in different time of wound establishment. (C) Ratio of collagen I to collagen III in Alg-group was higher than it in Vas-group during the diabetic wound healing. Hydroxyproline levels in wound skin homogenate treated with calcium alginate and vaseline (D) Alg-group: Alginate-treated group, Vas-group: Vaseline-treated group. *P<0.05 when compared with the corresponding controls. #P<0.05 when compared with the different periods in the same group.
Calcium alginate improved the level of hydroxyproline in skin homogenates
The hydroxyproline levels of diabetic wounded skin tissues on the 3, 7 and 14 day are shown in Figure 4D. The result indicated that a slight increase of hydroxyproline level in Alg-group on the 3rd day (30.29±0.92 ng/ml vs. 27.52±0.83 ng/ml, P<0.05), the increase of the hydroxyproline levels treated with calcium alginate on day 7 was significantly higher than Vas-group (51.04±1.31 ng/ml vs. 46.00±0.99 ng/ml, P<0.05), the hydroxyproline levels of day 14 were also greater than Vas-group (89.58±4.97 ng/ml vs. 79.30±4.42 ng/ml, P<0.05).
Discussion
Alginate dressing has been reported to accelerate diabetic foot ulcer healing [18,19]. As the results also showed in our study, the periodic observation of wound area indicated that the application of calcium alginate improved wound closure rate. However, how it works still remains inconclusive till now. This study, through the assay in vitro and diabetic wound in rats in vivo, firstly confirmed that calcium alginate promoted the healing course of diabetic wound which involved the decrease of inflammatory reaction, increase of collagen type I and the ratio of collagen I/III.
In this study, we found that the material (calcium alginate) apparently exhibits no cytotoxicity. Kondo et al considered that in the late phase of inflammation, the fibroblast cells synthesis the collagen fibers and other cytoskeleton matrix components [20,21]. Thus the low cytotoxicity of the calcium alginate to the fibroblast cells has made a significant contribution to the rapid synthesis of collagen during diabetic wound healing. We could suggest that calcium alginate can improve the content of collagen to accelerate wound closing course through decreasing the cytotoxicity of fibroblast cell.
Moreover, the wet healing theory was well-known from 50 years ago which consider that a wound heals more quickly when its surface environment is kept moist, rather than left to dry [22]. A moist environment is considered as provide optimal conditions for the cells involved with the wound healing process, which is thought to be a significant part of the healing pathway [23]. The use of wound dressings is a key driver to maintain a moist wound healing environment, calcium alginate dressing are highly hydrophilic and can absorb large volumes of wound exudation [24]. In addition, alginate is an anionic polysaccharide which has a capacity to form hydrogels which could keep a moist environment under very mild conditions [25,26]. In this study, we found that the expression of skin tissue collagen I was elevated by calcium alginate dressing application, and this dressing provide a moist environment and a faster collagen I related epithelization for diabetic wound healing.
In the present study the total healing rate of experimental wound in Alg-group at day 14 was 33.3% (2/6) and it was higher than that in Vas-group 0% (0/6), and the mean wound closing rate in Alg-group was faster than controls, this significant difference began from day 4, and lasted to day 14. These results confirmed that calcium alginate could accelerate the diabetic wound healing course. Our above results were consistent with Woo et al, who applied the calcium alginate to the circular full-thickness wounds created on the dorsum of non-diabetic rats, and they found that the wound size dramatically shrunk in the alginate-treated group compared with the control group at days 5 and 7 [26]. What actually happened, the good biocompatibility of calcium alginate played an important role in the process of diabetic wound healing. Our histological results of skin tissue on 3, 7 and 14 postoperative days revealed that the inflammatory reaction of calcium alginate treated skin was mild, it was beneficial in case of skin wound under diabetic condition, and the re-epithelialization was higher with extensive collagen deposition in mature dermis compared to vaseline treated group. This result was accordant with with Lansdown et al. They reported that calcium alginate induced a modest inflammatory reaction and possessed a good biocompatibility within the 3 month observation period [27]. The difference of the present study with theirs was that the calcium alginate was to topically apply to the diabetic wound not to implant subcutaneously in rats. The reason of its low adverse tissue reaction could be explained that the alginate has derived from natural brown seaweed and possessed low toxicity and biocompatibility [28]. Therefore, Calcium alginate treatment could induce a milder inflammation and a faster epithelization in the process of diabetic wound healing.
In the ulcer healing process, the centripetal movements of surrounding epithelial tissues which closed the wound opening was recruited by the maturing extracellular matrix [21]. And collagen is the main component of extracellular matrix which significantly contributes to the wound strength and wound healing process depends on the regulated synthesis and deposition of new collagen [29]. In this study, we found that the alginate treated group produced greater deposition of collagen in diabetic wound skin and almost all of wound closing course, and preliminarily indicated that the calcium alginate was able to promote the deposition of collagen in diabetic wound healing. This finding was also verified by the enhanced expression of collagen I and III through Western blotting. Collagen I and III are the mainly familiar collagen in connective tissue such as skin and so on which could account for at least 95% of all collagen content [30]. Thus, we mainly detected the distribution of types I and III of collagen. And our results demonstrated that calcium alginate application significantly up-regulated the expression of collagen I, whereas the expression of collagen III was not significantly altered. Whereas, the ratio of collagen I/III ascended simultaneously. Broughton et al considered that in the later stages of the normal wound healing process, collagen III is re-absorptive and a thicker collagen is formed and organized along the lines of tension which elevates the tensile strength of the wound [31], these denser beams are mainly represented by collagen I [32]. And the high percentage of collagen I compared with collagen III demonstrates the state of collagen maturation [33]. In this study we revealed that calcium alginate boosted the ratio of collagen I/III during diabetic wound healing, and this maybe the important reason of its accelerating effect on the skin wound closing course. The similar result was reported by Woo et al who found that the expression of collagen I was increased in alginate treated group at day 5 and 14 by Western blotting. However, our study differed with theirs from that the dressing they applied was the alginate (without calcium ions), their wound model was based on non-diabetic rat model, and the collagen III was not been determined in their study [26]. And the role of calcium ions in the alginate were that they could be exchanged for the sodium ions in wound fluid formed a soluble calcium/sodium alginate gel to keep a moist healing environment [34]. As we know, the distribution of collagen I and III fiber and their optimum ratio are critical to maintain required crosslinked density and mechanical toughness during the wound healing process [10]. And Birk et al considered that the ratio of collagen I/III regulated the diameter of new fiber and determined the structure of granulation tissue, and the increasing of ratio of collagen I/III could strengthen the stability of wound tissue structure [35]. Thus, the calcium alginate’s contribution to the rapid healing of diabetic wound was attributed to its upregulating effect of collagen I and keeping high ratio of collagen I/III, and this influence possesses the potential impact on the mechanism that it kept the stability of newly formed granulation and epithelium tissue and promoted it closure tightly. Hereby, our above results are of important meaning to understand the detailed mechanism of this dressing and drive its clinical utility in diabetes patients.
Moreover, it is well known that hydroxyproline is a basic component of collagen fiber structure and its contents is an index of collagen synthesis [36], and the hydroxyproline level indirectly indicated the change of collagen. In this study the hydroxyproline level of diabetic wounded skin tissues on the 3, 7 and 14 days in calcium alginate treated group are also slightly increased compared to control group. It proved that calcium alginate could greatly increase the content of hydroxyproline compared to the control group in diabetic rat. Therefore, the enhancing of hydroxyproline content also reflected the augment of collagen components stimulated by calcium alginate, and played a significant role through collagen synthesis during the diabetic wound healing.
There are some limitations of this study. Firstly, the observing period of this study was relatively short with only 2 weeks, the condition of diabetic wound on day 21 after post-operative was not evaluated because that the average wound closure rate in Alg-group more than 95% at day 14. Secondly, the Real-Time PCR technology did not applied to examination of the mRNA expression of collagen in skin tissue of wound area, and the relationship between calcium alginate and the mRNA expression of collagen in diabetes ulcerations should be explored in the future. At last, because collagen I and III are the mainly collagen in connective tissue such as skin, and they account for at least 95% of all collagen contents, only type I and III collagens were measured in this study. However, it is possible that the other types of collagen also in part contribute to diabetic wound healing, the study related to these aspects should be carried out in the future.
In conclusion, the present study revealed that calcium alginate was with the excellent cytocompatibility and histocompatibility characteristics and acted as a promoter of diabetic wound healing via increasing the contraction of wounds, attenuating inflammatory reaction, by increasing the levels of type I collagen and hydroxylproline leading to a significantly increase in the wound tensile strength. All in all, the accelerating effect of calcium alginate was due to the stimulation of collagen I expression and elevation of collagen I to III ratios to a large extent. This dressing provides a potential strategy for wound healing and provided an easily used way to ameliorate the foot ulceration and prevent the limb amputation in diabetic populations.
Acknowledgements
The authors appreciate Shangdong Yinuo Biotechnology Co., Ltd for providing calcium alginate dressing for this work. Authors are also thankful to Shanghai Key Laboratory of Diabetes for providing necessary technical support for carrying out the research work.
Disclosure of conflict of interest
None.
References
- 1.Yang W, Lu J, Weng J, Jia W, Ji L, Xiao J, Shan Z, Liu J, Tian H, Ji Q, Zhu D, Ge J, Lin L, Chen L, Guo X, Zhao Z, Li Q, Zhou Z, Shan G, He J. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362:1090–1101. doi: 10.1056/NEJMoa0908292. [DOI] [PubMed] [Google Scholar]
- 2.Xu Y, Wang LM, He J, Bi YF, Li M, Wang TG, Wang LH, Jiang Y, Dai M, Lu JL, Xu M, Li YC, Hu N, Li JH, Mi SQ, Chen CS, Li GW, Mu YM, Zhao JJ, Kong LZ, Chen JL, Lai SG, Wang WQ, Zhao WH, Ning G. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–959. doi: 10.1001/jama.2013.168118. [DOI] [PubMed] [Google Scholar]
- 3.Brem H, Tomic-Canic M. Cellular and molecular basis of wound healing in diabetes. J Clin Invest. 2007;117:1219–1222. doi: 10.1172/JCI32169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pavlovic MD, Milenkovic T, Dinic M, Misovic M, Dakovic D, Todorovic S, Dakovic Z, Zecevi RD, Doder R. The prevalence of cutaneous manifestations in young patients with type 1 diabetes. Diabetes Care. 2007;30:1964–1967. doi: 10.2337/dc07-0267. [DOI] [PubMed] [Google Scholar]
- 5.Rhett JM, Ghatnekar GS, Palatinus JA, O’Quinn M, Yost MJ, Gourdie RG. Novel therapies for scar reduction and regenerative healing of skin wounds. Trends Biotechnol. 2008;26:173–180. doi: 10.1016/j.tibtech.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 6.Kumar B, Vijayakumar M, Govindarajan R, Pushpangadan P. Ethnopharmacological approaches to wound healing-exploring medicinal plants of India. J Ethnopharmacol. 2007;114:103–113. doi: 10.1016/j.jep.2007.08.010. [DOI] [PubMed] [Google Scholar]
- 7.Wess TJ. Collagen fibril form and function. Adv Protein Chem. 2005;70:341–374. doi: 10.1016/S0065-3233(05)70010-3. [DOI] [PubMed] [Google Scholar]
- 8.Rajan V, Murray RZ. The duplicitous nature of inflammation in wound repair. Wound Practice and Research. 2008;16:122–129. [Google Scholar]
- 9.Junge K, Klinge U, Rosch R, Mertens PR, Kirch J, Klosterhalfen B, Lynen P, Schumpelick V. Decreased collagen type I/III ratio in patients with recurring hernia after implantation of alloplastic prostheses. Langenbecks Arch Surg. 2004;389:17–22. doi: 10.1007/s00423-003-0429-8. [DOI] [PubMed] [Google Scholar]
- 10.Dale PD, Sherratt JA, Maini PK. A mathematical model for collagen fibre formation during fetal and adult dermal wound healing. Proc Biol Sci. 1996;263:653–660. doi: 10.1098/rspb.1996.0098. [DOI] [PubMed] [Google Scholar]
- 11.Ishihara M, Nakanishi K, Ono K, Sato M, Kikuchi M, Saito Y, Yura H, Matsui T, Hattori H, Uenoyama M, Kurita A. Photocrosslinkable chitosan as a dressing for wound occlusion and accelerator in healing process. Biomaterials. 2002;23:833–840. doi: 10.1016/s0142-9612(01)00189-2. [DOI] [PubMed] [Google Scholar]
- 12.Jude EB, Apelqvist J, Spraul M, Martini J. Prospective randomized controlled study of Hydrofiber dressing containing ionic silver or calcium alginate dressings in non-ischaemic diabetic foot ulcers. Diabet Med. 2007;24:280–288. doi: 10.1111/j.1464-5491.2007.02079.x. [DOI] [PubMed] [Google Scholar]
- 13.Jayakumar R, Rajkumar M, Freitas H, Selvamurugan N, Nair SV, Furuike T, Tamura H. Preparation, characterization, bioactive and metal uptake studies of alginate/phosphorylated chitin blend films. Int J Biol Macromol. 2009;44:107–111. doi: 10.1016/j.ijbiomac.2008.10.010. [DOI] [PubMed] [Google Scholar]
- 14.Kristiansen KA, Schirmer B, Aachmann FL, Gudmund SB, Draget KI, Christensen BE. Novel alginates prepared by independent control of chain stiffness and distribution of G-residues: Structure and gelling properties. Carbohydr Polym. 2009;77:725–735. [Google Scholar]
- 15.Balakrishnan B, Mohanty M, Umashankar PR, Jayakrishnan A. Evaluation of an in situ forming hydrogel wound dressing based on oxidized alginate and gelatin. Biomaterials. 2005;26:6335–6342. doi: 10.1016/j.biomaterials.2005.04.012. [DOI] [PubMed] [Google Scholar]
- 16.Adetutu A, Morgan WA, Corcoran O. Antibacterial, antioxidant and fibroblast growth stimulation activity of crude extracts of Bridelia ferruginea leaf, a wound-healing plant of Nigeria. J Ethnopharmacol. 2011;133:116–119. doi: 10.1016/j.jep.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 17.Warner RL, Bhagavathula N, Nerusu K, Hanosh A, McClintock SD, Naik MK, Johnson KJ, Ginsburg I, Varani J. MDI 301, a nonirritating retinoid, improves abrasion wound healing in damaged/atrophic skin. Wound Repair Regen. 2008;16:117–124. doi: 10.1111/j.1524-475X.2007.00338.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lazaro-Martinez JL, Cecilia-Matilla A, Aragon-Sanchez J, Garcia-Morales E, Garcia-Alvarez Y, Alvaro-Afonso F. Treatment of infected diabetic foot ulcers clinical effectiveness of a dressing of alginate and hydrocolloid, with silver fiber. Analysis of results of a series of cases. Rev Enferm. 2013;36:29–34. [PubMed] [Google Scholar]
- 19.Dumville JC, O’Meara S, Deshpande S, Speak K. Alginate dressings for healing diabetic foot ulcers. Cochrane Database Syst Rev. 2013;25:26. doi: 10.1002/14651858.CD009110.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mimura Y, Ihn H, Jinnin M, Asano Y, Yamane K, Tamaki K. Epidermal growth factor induces fibronectin expression in human dermal fibroblasts via protein kinase C δ signaling pathway. J Invest Dermatol. 2004;122:1390–1398. doi: 10.1111/j.0022-202X.2004.22618.x. [DOI] [PubMed] [Google Scholar]
- 21.Kondo T, Ishida Y. Molecular pathology of wound healing. Forensic Sci Int. 2010;203:93–98. doi: 10.1016/j.forsciint.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 22.Winter GD, Scales JT. Effect of air drying and dressings on the surface of a wound. Nature. 1963;197:91. doi: 10.1038/197091b0. [DOI] [PubMed] [Google Scholar]
- 23.Cardinal M, Eisenbud DE, Armstrong DG, Zelen C, Driver V, Attinger C, Phillips T, Harding K. Serial surgical debridement: a retrospective study on clinical outcomes in chronic lower extremity wounds. Wound Repair Regen. 2009;17:306–311. doi: 10.1111/j.1524-475X.2009.00485.x. [DOI] [PubMed] [Google Scholar]
- 24.Moody M. Tissue viability. Calcium alginate: a dressing trial. Nurs Stand Spec Suppl. 1991;13:3–6. [PubMed] [Google Scholar]
- 25.Lee KY, Mooney DJ. Alginate: properties and biomedical applications. Prog Polym Sci. 2012;37:106–126. doi: 10.1016/j.progpolymsci.2011.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lee WR, Park JH, Kim KH, Kim SJ, Park DH, Chae MH, Suh SH, Jeong SW, Park KK. The biological effects of topical alginate treatment in an animal model of skin wound healing. Wound Repair Regen. 2009;17:505–510. doi: 10.1111/j.1524-475X.2009.00496.x. [DOI] [PubMed] [Google Scholar]
- 27.Lansdown AB, Payne MJ. An evaluation of the local reaction and biodegradation of calcium sodium alginate (Kaltostat) following subcutaneous implantation in the rat. J R Coll Surg Edinb. 1994;39:284–288. [PubMed] [Google Scholar]
- 28.Gombotz WR, Wee SF. Protein release from alginate matrices. Adv Drug Delivery Rev. 1998;31:267–285. doi: 10.1016/s0169-409x(97)00124-5. [DOI] [PubMed] [Google Scholar]
- 29.Maehata Y, Takamizawa S, Ozawa S, Izukuri K, Kato Y, Sato S, Lee MC, Kimura A, Hata R. Type III collagen is essential for growth acceleration of human osteoblastic cells by ascorbic acid 2-phosphate, a long-acting vitamin C derivative. Matrix Biol. 2007;26:371–381. doi: 10.1016/j.matbio.2007.01.005. [DOI] [PubMed] [Google Scholar]
- 30.Krane SM, Byrne MH, Lemaitre V, Henriet P, Jeffrey JJ, Witter JP, Liu X, Wu H, Jaenisch R, Eeckhout Y. Different collagenase gene products have different roles in degradation of type I collagen. J Biol Chem. 1996;271:28509–28515. doi: 10.1074/jbc.271.45.28509. [DOI] [PubMed] [Google Scholar]
- 31.Broughton G 2nd, Janis JE, Attinger CE. Wound healing: an overview. Plast Reconstr Surg. 2006;117:1e-S–32e-S. doi: 10.1097/01.prs.0000222562.60260.f9. [DOI] [PubMed] [Google Scholar]
- 32.Medrado AP, Soares AP, Santos ET, Reis SR, Andrade ZA. Influence of laser photobiomodulation upon connective tissue remodeling during wound healing. J Photochem Photobiol B. 2008;92:144–152. doi: 10.1016/j.jphotobiol.2008.05.008. [DOI] [PubMed] [Google Scholar]
- 33.Busnardo VL, Biondo-Simoes ML. Effects of low-level helium-neon laser on induced wound healing in rats. Rev Bras Fisioter. 2010;14:45–51. [PubMed] [Google Scholar]
- 34.Gensheimer D. A review of calcium alginates. Ostomy Wound Manage. 1993;39:34–8. 42–43. [PubMed] [Google Scholar]
- 35.Birk DE, Mayne R. Localization of collagen types I, III and V during tendon development. Changes in collagen types I and III are correlated with changes in fibril diameter. Eur J Cell Biol. 1997;72:352–361. [PubMed] [Google Scholar]
- 36.Weis MA, Hudson DM, Kim L, Scott M, Wu JJ, Eyre DR. Location of 3-Hydroxyproline residues in collagen types I, II, III and V/XI implies a role in fibril supramolecular assembly. J Biol Chem. 2010;285:2580–2590. doi: 10.1074/jbc.M109.068726. [DOI] [PMC free article] [PubMed] [Google Scholar]