

Abstract
Carcinosarcoma of the gallbladder is a rare malignancy characterized by malignant epithelial and mesenchymal components. The disease usually presents at an advanced stage, and as a result, curative resection is uncommon. This report describes a case that underwent curative resection. We herein declare the case of a patient in a 62-year-old male, with carcinosarcoma of the gallbladder with chondroid differentiation. The patient is treated by a simple cholecystectomy, a wedge resection of the underlying liver tissue and the pericholedochal lymph nodes for a tumor which occupied the entire gallbladder. Histologically, the epithelial component of the tumor was composed of adenocarcinoma and the mesenchymal component was composed of fibrosarcoma. The tumor was identified as extend to the serosa tissue and to have metastasized to no lymph node. The prognosis of carcinosarcoma of the gallbladder remains poor despite curative resection, and thus, the authors recommend that effort should be made to improve surgical outcomes. The patient survived 13 months and is still alive today.
Keywords: Gallbladder, carcinoma, carcinosarcoma, curative treatment, prognosis
Introduction
Carcinosarcomas are rare tumors that are characterized by malignant epithelial and mesenchymal elements. These tumors have been reported in many different organs, including the uterus, lung, esophagus, kidney, and pancreas [1-3]. Carcinosarcomas of the gallbladder are uncommon. Up to now, < 100 cases have been reported in the English literature. The invasive nature and aggressive biology of carcinosarcoma of gallbladder adequately explains the limited number of respectable cases. Here, we report a case of carcinosarcoma of gallbladder treated by curative radical cholecystectomy.
Case report
A 62-year-old man, with the complaints of intervallic pain before admission, presented with a 5 months of abdominal pain in the upper right quadrant. There was not any history of fever, vomiting, anorexia or weight loss. The patient reported a past medical history of chronic cholecystitis, hypertension and diabetes mellitus. A physical examination illustrated tenderness in the right upper quadrant of the abdomen. A laboratory analysis revealed haemoglobin of 98 g/L, a normal leukocyte count. The tumor marker, serum carcinoembryonic antigen, carbohydrate antigen 19-9 and α-fetoprotein (AFP) levels were normal. Liver function tests revealed that total cholesterol levels were increased to 5.22 mmol/L. Abdominal computed tomography (CT) revealed a intraluminal polypoid mass with no demonstrable lymph nodes in the pericholecystic and upper abdominal regions (Figure 1), and magnetic resonance imaging (MRI) showed irregular wall thickening with enhancement of the fundus of the gallbladder (Figure 2). The preliminary diagnosis was gallbladder cancer. During the surgery, the frozen examination revealed that it was a malignant mesenchymal tumor. A simple cholecystectomy, with a wedge resection of the underlying liver tissue and the pericholedochal lymph nodes were performed. The specimens were sent for histopathology. The macroscopic examination of the specimen showed a 5 × 4 cm tumor with a polypoid structure, which originated from the body of the gallbladder and filled the entire gallbladder lumen. The tumor was a solid mass with hemorrhagic and necrotic foci (Figure 3). Histologically, the tumor was formed of two distinct components, namely moderately-differentiated tubular adenocarcinoma and sarcomatous tissue with fibrosarcoma differentiation (Figure 4A and 4B). An immunohistochemical examination demonstrated positive staining for cytokeratin and epithelial membrane antigen (EMA) in the epithelial areas (Figure 5A, 5B), vimentin in the mesenchymal component (Figure 5C). Staining for smooth muscle actin (SMA) and S-100 was negative. This gallbladder carcinoma was classified as stage II (T2N0M0) using the classification of the International Union Against Cancer (UICC). The patient survived 13 months and is still alive today.
Figure 1.

Abdomen computed tomography showed an intraluminal polypoid masses possible gallbladder cancer.
Figure 2.
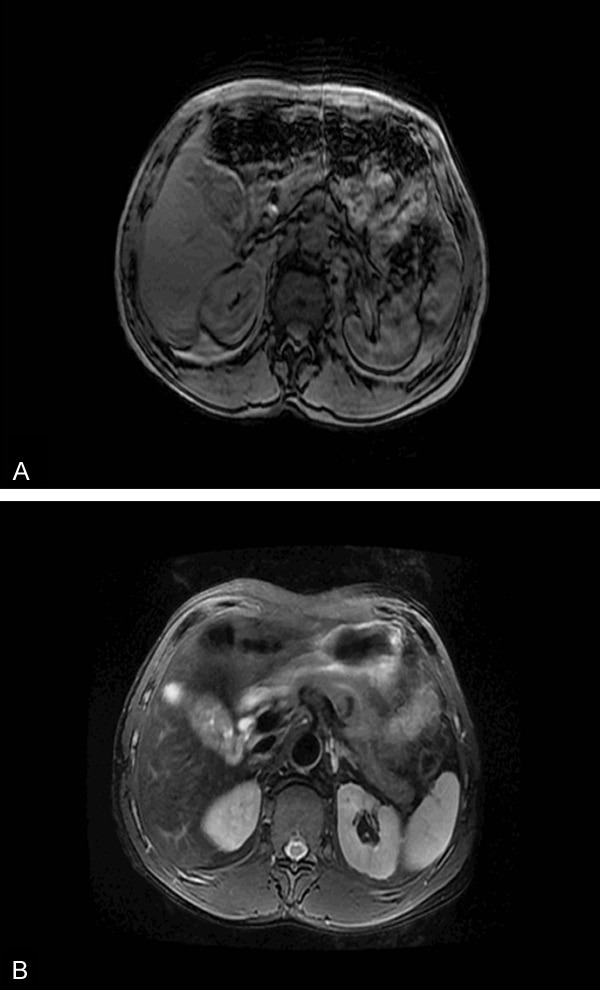
The abdominal magnetic resonance imaging (MRI) showed irirregular wall thickening with enhancement of the body of the gallbladder (A, B).
Figure 3.
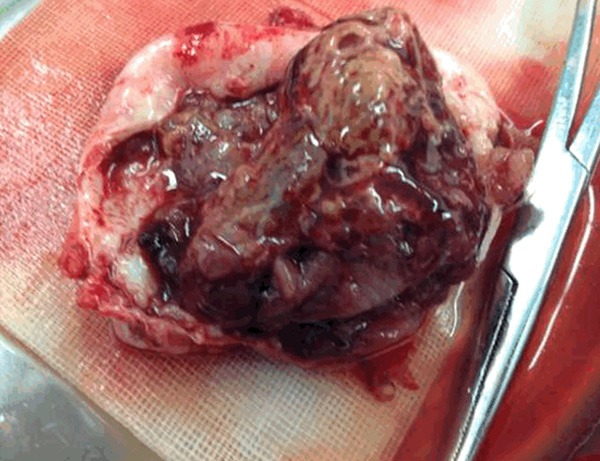
The gross examination of carcinosarcoma of the gallbladder revealed a 5 × 4 cm tumor with a polypoid structure, which originated from the body of the gallbladder and filled the entire gallbladder lumen. The tumor was a solid mass with hemorrhagic and necrotic foci.
Figure 4.
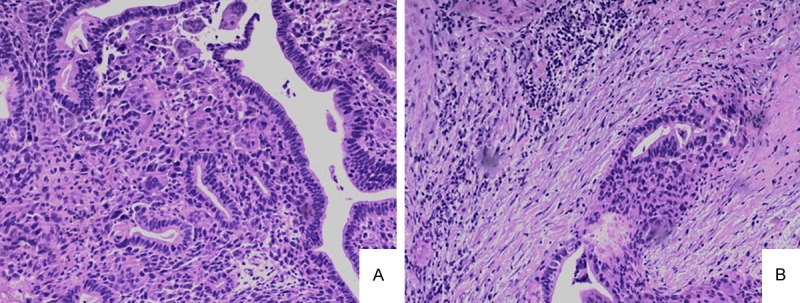
Histologically, the tumor contains two distinct components: a well to moderately differentiated adenocarcinoma (A) and fibroid differentiated sarcomatous tissue (B) (H & E stain, original magnifications: 100 ×).
Figure 5.
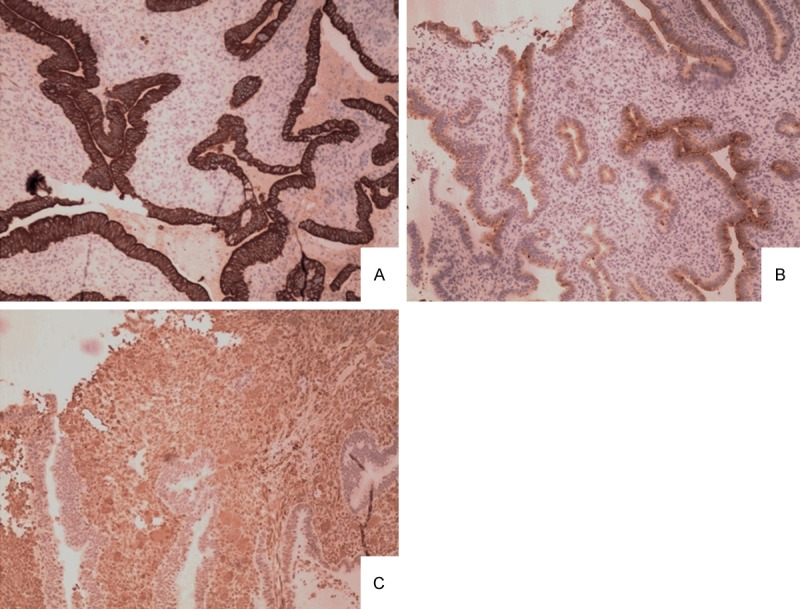
A. Strong cytokeratin positivity in malignant glands forming the epithelial component (cytokeratin, original magnifications: 100 ×). B. Strong epithelial membrane antigen (EMA) positivity in malignant glands forming the epithelial component (EMA, original magnifications: 100 ×). C. Strong vimentin positivity in the malignant mesenchymal component (vimentin, original magnifications: 100 ×).
Discussion
The first case of a carcinosarcoma of the gallbladder was reported by Landsteiner in 1907 [4]. Up to now, < 100 cases have been reported in the English literature. Carcinosarcomas of the gallbladder consist of both epithelial and mesenchymal components. The diagnosis requires the presence the two histological components. The epithelial component usually consists of adenocarcinoma, although an element of squamous cell carcinoma is also occasionally observed. The mesenchymal component typically consists of undifferentiated spindle or satellite cells, and is occasionally accompanied by various proportions of heterogenous elements, including chondrosarcoma, osteosarcoma, rhabdomyosarcoma and leiomyosarcoma [5]. Zhang et al [6] reported that adenocarcinoma was the most common epithelial component (79.2%) while squamous cell carcinoma was the least common (9.4%). Spindle cell type was the most common mesenchymal component (44.6%) when compared with osteoid, which was the least common (5.4%). In the case presented, the epithelial component of the tumor was composed of adenocarcinoma and the mesenchymal component was composed of fibrosarcoma. An immunohistochemical examination demonstrated that the epithelial component was positive for cytokeratin, while the mesenchymal component was positive for vimentin.
Although recent studies suggest some causative factors, such as multistep genetic alterations, the precise mechanisms of gallbladder carcinogenesis have not been clearly elucidated. At present, two opposing theories have been hypothesized to account for the origin of these morphologically diverse tumors. The multiclonal theory regards a carcinosarcoma as a collision tumor composed of the derivatives of two or more stem cells of separate epithelial and mesenchymal origin. The monoclonal theory proposes that carcinomatous and sarcomatous elements are derived from a single pluripotential stem cell that subsequently develops divergent differentiation along separate epithelial and mesenchymal pathways [7]. Dacic et al [8] found identical allelic losses shared by each tumor component, without discordant losses. This was consistent with the hypothesis that the carcinomatous and sarcomatous components of this neoplasm were derived from a single pluripotent stem cell and that the tumor was monoclonal.
The symptoms and signs of gallbladder carcinosarcoma are non-specific. Representative clinical symptoms include right upper abdominal pain and masses, loss of appetite, weight loss, general fatigue, jaundice, and vomiting. In addition, 66.7%-83% [9,10] of the cases presented with simultaneous cholecystolithiasis.
Zhang et al [6] reported that tumors which were smaller than 5 cm had a longer survival and that therefore, the tumor size should be considered as a major component in the future staging system. They also indicated that the presence of gallstones, epithelial and mesenchymal component types, age and sex were of little prognostic value. The most common treatments are surgery. There is no successful treatment reported with radiotherapy or chemotherapy [11].
The prognosis of this disease is normally poor. Most cases present with locally advanced disease. Liver metastasis and peritoneal dissemination are widespread in these cases. Adrenal glands, pancreas, diaphragm, and lower thoracic vertebrae are the other metastatic sites reported in the literature. Regional, retroperitoneal, and para-aortic lymph nodes may be involved. The mean survival time after diagnosis is usually only a few months [12-14]. We analyzed data from 20 patients recorded in the literature from 1980 to 2013 who underwent surgical management for carcinosarcoma of the gall bladder (Table 1). These patients consisted of 8 male and 12 female with a mean age of 65.2 years (range 45 to 83 years). Zhang et al [6] reported that for 68 patients with carcinosarcoma of the gallbladder, the mean survival time is 17.5 months, and the 1-year survival rate and 5-year survival rate are (19 ± 5)% and (16 ± 5)% respectively. As reported by Uzun MA, the longest survival time was 54 months [15]. In that case, a polypoid tumor of 2 cm in size protruded into the gallbladder lumen. A microscopic study showed that the tumor had infiltrated the surrounding connective and adipose tissue overlapping its primary site, but had not perforated the serosa nor invaded the liver. The patient was handled by a radical cholecystectomy and remained healthy for 54 months.
Table 1.
Twenty reported cases of surgical resection for carcinosarcoma of the gall bladder
| Author | Year | Age (yr) | Sex | Pistion | Stone | Size (cm) | Depth | Stage | Surivial (mo) |
|---|---|---|---|---|---|---|---|---|---|
| Mansori et al [15] | 1980 | 81 | M | Body | - | 15 | liver | IVa | 1.5 |
| Von Kuster et al [16] | 1982 | 77 | F | Fundus | - | 3 | mp | II | 311 |
| Inoshita et al [17] | 1986 | 53 | M | Neck | - | 11 | bd | IVa | 17 |
| Lumsden et al [18] | 1988 | 81 | F | Neck | - | 5 | mp | II | 121 |
| Ishihara et al [19] | 1990 | 58 | F | Fundus | - | 8 | mp | II | 71 |
| Fagot et al [20] | 1994 | 83 | F | Fundus | + | 4.5 | mp | II | 121 |
| Eriguchi et al [21] | 1999 | 65 | F | ND | + | 10 | mp | II | 161 |
| Ajiki et al [22] | 2002 | 69 | F | Body | + | 6 | liver | IVa | 7 |
| Kim et al [23] | 2003 | 61 | F | Neck | - | 4.5 | si | IVa | 21 |
| Sodergren et al [11] | 2005 | 68 | F | Neck | - | 9 | bd | IVa | 5 |
| Kubota et al [24] | 2006 | 72 | M | Body | - | 7 | liver, colon | IVa | 8 |
| Uzun et al [25] | 2009 | 70 | M | Fundus | - | 10 | mp | II | 541 |
| Shimada et al [26] | 2009 | 69 | M | Body | + | 9 | si | II | 61 |
| Okabayashi et al [27] | 2009 | 72 | F | Body | - | 2.5 | mp | II | 601 |
| Park et al [28] | 2012 | 77 | M | Fundus | - | 8 | mp | III | 2.5 |
| Kim et al [29] | 2012 | 77 | F | Fundus | - | 6.5 | ND | II | 31 |
| 81 | M | Fundus | - | 2 | liver | III | 4 | ||
| Parreira et al [30] | 2012 | 59 | F | ND | - | 5 | ND | ND | 6 |
| Khanna et al [31] | 2013 | 45 | F | body | - | 6 | mp | II | 61 |
| Wang et al [32] | 2013 | 68 | F | Fundus | - | 10 | ND | II | ND |
| Present case | 2015 | 62 | M | Body | - | 5 | si | II | 131 |
Alive patients;
si: Serosal invasion; bd: Bile duct; mp: Muscularis propria; ND: Notdescribed; Stage: Classification according to UICC (International Union Against Cancer).
Disclosure of conflict of interest
None.
References
- 1.Iwaya T, Maesawa C, Tamura G, Sato N, Ikeda K, Sasaki A, Othuka K, Ishida K, Saito K, Satodate R. Esophageal carcinosarcoma: a genetic analysis. Gastroenterology. 1997;113:973–937. doi: 10.1016/s0016-5085(97)70194-x. [DOI] [PubMed] [Google Scholar]
- 2.Higashi M, Takao S, Sato E. Sarcomatoid carcinoma of the pancreas: a case report with immunohistochemical study. Pathol Int. 1999;49:453–456. doi: 10.1046/j.1440-1827.1999.00877.x. [DOI] [PubMed] [Google Scholar]
- 3.Reuter VE. Sarcomatoid lesions of the urogenital tract. Semin Diagn Pathol. 1993;10:188–201. [PubMed] [Google Scholar]
- 4.Landsteiner K. Plattenepithelkarzinom und Sarkom der Gallenblasse in einem falle von Gallenblasse. Ztschr Klin Med. 1907;62:427–433. [Google Scholar]
- 5.Kuroki T, Tajima Y, Matsuo K, Kanematsu T. Genetic alterations in gallbladder carcinoma. Surg Today. 2005;35:101–105. doi: 10.1007/s00595-004-2906-2. [DOI] [PubMed] [Google Scholar]
- 6.Zhang L, Chen Z, Fukuma M, Lee LY, Wu M. Prognostic Signifiance of Race and Tumor Size in Carcinosarcoma of Gallbladder: a Meta-Analysis of 68 Cases. Int J Clin Exp Pathol. 2008;1:75–83. [PMC free article] [PubMed] [Google Scholar]
- 7.Uzun MA, Koksal N, Gunerhan Y, Celik A, Guneş P. Carcinosarcoma of the gallbladder: report of a case. Surg Today. 2009;39:168–171. doi: 10.1007/s00595-008-3805-8. [DOI] [PubMed] [Google Scholar]
- 8.Dacic S, Finkelstein SD, Sasatomi E, Swalsky PA, Yousem SA. Molecular pathogenesis of pulmonary carcinosarcoma as determined by microdissection‑based allelotyping. Am J Surg Pathol. 2002;26:510–516. doi: 10.1097/00000478-200204000-00015. [DOI] [PubMed] [Google Scholar]
- 9.Lazcano-Ponce EC, Miquel JF, Munoz N, Herrero R, Ferrecio C, Wistuba II, Alonso de Ruiz P, Aristi Urista G, Nervi F. Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J Clin. 2001;51:349–364. doi: 10.3322/canjclin.51.6.349. [DOI] [PubMed] [Google Scholar]
- 10.Nimura Y. Extended surgery in bilio-pancreatic cancer: The Japanese experience. Semin Oncol. 2002;29:17–22. doi: 10.1053/sonc.2002.37371. [DOI] [PubMed] [Google Scholar]
- 11.Sodergren MH, Silva MA, Read-Jones SL, Hubscher SG, Mirza DF. Carcinosarcoma of the biliary tract: two case reports and a review of the literature. Eur J Gastroenterol Hepatol. 2005;17:683–685. doi: 10.1097/00042737-200506000-00016. [DOI] [PubMed] [Google Scholar]
- 12.Hotta T, Tanimura H, Yokoyama S, Ura K, Yamaue H. So-called carcinosarcoma of the gallbladder; spindle cell carcinoma of the gallbladder: report of a case. Surg Today. 2002;32:462–467. doi: 10.1007/s005950200077. [DOI] [PubMed] [Google Scholar]
- 13.Takahashi Y, Fukushima J, Fukusato T, Shiga J. Sarcomatoid carcinoma with components of small cell carcinoma and undifferentiated carcinoma of the gallbladder. Pathol Int. 2004;54:866–871. doi: 10.1111/j.1440-1827.2004.01771.x. [DOI] [PubMed] [Google Scholar]
- 14.Iezzoni JC, Mills SE. Sarcomatoid carcinomas (carcinosarcomas) of the gastrointestinal tract: a review. Semin Diagn Pathol. 1993;10:176–187. [PubMed] [Google Scholar]
- 15.Mansori KS, Cho SY. Malignant mixed tumor of the gallbladder. Am J Clin Pathol. 1980;73:709–711. doi: 10.1093/ajcp/73.5.709. [DOI] [PubMed] [Google Scholar]
- 16.Von Kuster LC, Cohen C. Malignant mixed tumor of the gallbladder: report of two cases and a review of the literature. Cancer. 1982;50:1166–1170. doi: 10.1002/1097-0142(19820915)50:6<1166::aid-cncr2820500622>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 17.Inoshita S. Phyllodes tumor (cystosarcoma phyllodes) of the breast. A clinicopathologic study of 45 cases. Acta Pathol Jpn. 1988;38:21–33. doi: 10.1111/j.1440-1827.1988.tb01069.x. [DOI] [PubMed] [Google Scholar]
- 18.Lumsden AB, Mitchell WE, Vohman MD. Carcinosarcoma of the gallbladder: a case report and review of the literature. Am Surg. 1988;54:492–494. [PubMed] [Google Scholar]
- 19.Ishihara T, Kawano H, Takahashi M, Yokota T, Uchino F, Matsumoto N, Fukuyama N. Carcinosarcoma of the gallbladder. A case report with immunohistochemical and ultrastructural studies. Cancer. 1990;66:992–997. doi: 10.1002/1097-0142(19900901)66:5<992::aid-cncr2820660532>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 20.Fagot H, Fabre JM, Ramos J, Laffay V, Guillon F, Domergue J, Baumel H. Carcinosarcoma of the gallbladder. A case report and review of the literature. J Clin Gastroenterol. 1994;18:314–316. doi: 10.1097/00004836-199406000-00011. [DOI] [PubMed] [Google Scholar]
- 21.Eriguchi N, Aoyagi S, Hara M, Hashino K, Imamura M, Sato S, Imamura I, Kutami R, Jimi A. A so-called carcinosarcoma of the gallbladder in a patient with multiple anomalies-a case report. Kurume Med J. 1999;46:175–179. doi: 10.2739/kurumemedj.46.175. [DOI] [PubMed] [Google Scholar]
- 22.Ajiki T, Nakamura T, Fujino Y, Suzuki Y, Takeyama Y, Ku Y, Kuroda Y, Ohbayashi C. Carcinosarcoma of the gallbladder with chondroid differentiation. J Gastroenterol. 2002;37:966–971. doi: 10.1007/s005350200162. [DOI] [PubMed] [Google Scholar]
- 23.Kim MJ, Yu E, Ro JY. Sarcomatoid carcinoma of the gallbladder with a rhabdoid tumor component. Arch Pathol Lab Med. 2003;127:e406–e408. doi: 10.5858/2003-127-e406-SCOTGW. [DOI] [PubMed] [Google Scholar]
- 24.Kubota K, Kakuta Y, Kawamura S, Abe Y, Inamori M, Kawamura H, Kirikoshi H, Kobayashi N, Saito S, Nakajima A. Undifferentiated spindle-cell carcinoma of the gallbladder: an immunohistochemical study. J Hepatobiliary Pancreat Surg. 2006;13:468–471. doi: 10.1007/s00534-006-1100-x. [DOI] [PubMed] [Google Scholar]
- 25.Uzun MA, Koksal N, Gunerhan Y, Celik A, Guneş P. Carcinosarcoma of the gallbladder: report of a case. Surg Today. 2009;39:168–171. doi: 10.1007/s00595-008-3805-8. [DOI] [PubMed] [Google Scholar]
- 26.Shimada K, Iwase K, Aono T, Nakai S, Takeda S, Fujii M, Koma M, Nishikawa K, Matsuda C, Hirota M, Fushimi H, Tanaka Y. Carcinosarcoma of the gallbladder producing alpha-fetoprotein and manifesting as leukocytosis with elevated serum granulocyte colony-stimulating factor: report of a case. Surg Today. 2009;39:241–246. doi: 10.1007/s00595-008-3833-4. [DOI] [PubMed] [Google Scholar]
- 27.Okabayashi T, Sun ZL, Montgomey RA, Hanazaki K. Surgical outcome of carcinosarcoma of the gall bladder: A review. World J Gastroenterol. 2009;15:4877–4882. doi: 10.3748/wjg.15.4877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Park SB, Kim YH, Rho HL, Chae GB, Hong SK. Primary carcinosarcoma of the gallbladder. J Korean Surg Soc. 2012;82:54–58. doi: 10.4174/jkss.2012.82.1.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim HH, Hur YH, Jeong EH, Park EK, Koh YS, Kim JC, Kim HJ, Kim JW, Cho CK. Carcinosarcoma of the gallbladder: report of two cases. Surg Today. 2012;47:670–675. doi: 10.1007/s00595-012-0160-6. [DOI] [PubMed] [Google Scholar]
- 30.Parreira JM, Siqueira DE, Menacho AM, Pelizzari LL, Santos LC. Carcinosarcoma of the gallbladder: case report. Arq Bras Cir Dig. 2012;25:65–66. doi: 10.1590/s0102-67202012000100015. [DOI] [PubMed] [Google Scholar]
- 31.Khanna M, Khanna A, Manjari M. Carcinosarcoma of the gallbladder: a case report and review of the literature. J Clin Diagn Res. 2013;7:560–562. doi: 10.7860/JCDR/2013/4924.2825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wang Y, Gu X, Li Z, Xiang J, Chen Z. Gallbladder carcinosarcoma accompanied with bile duct tumor thrombi: A case report. Oncol Lett. 2013;5:1809–1812. doi: 10.3892/ol.2013.1289. [DOI] [PMC free article] [PubMed] [Google Scholar]