

Abstract
Oral fluid (OF) is a new biological matrix for clinical and forensic drug testing, offering non-invasive and directly observable sample collection reducing adulteration potential, ease of multiple sample collections, lower biohazard risk during collection, recent exposure identification, and stronger correlation with blood than urine concentrations. Because cannabinoids are usually the most prevalent analytes in illicit drug testing, application of OF drug testing requires sufficient scientific data to support sensitive and specific OF cannabinoid detection. This review presents current knowledge on OF cannabinoids, evaluating pharmacokinetic properties, detection windows, and correlation with other biological matrices and impairment from field applications and controlled drug administration studies. In addition, on-site screening technologies, confirmatory analytical methods, drug stability, and effects of sample collection procedure, adulterants, and passive environmental exposure are reviewed. Delta-9-tetrahydrocannabinol OF concentrations could be > 1000 μg/L shortly after smoking, whereas minor cannabinoids are detected at 10-fold and metabolites at 1000-fold lower concentrations. OF research over the past decade demonstrated that appropriate interpretation of test results requires a comprehensive understanding of distinct elimination profiles and detection windows for different cannabinoids, which are influenced by administration route, dose, and drug use history. Thus, each drug testing program should establish cutoff criteria, collection/analysis procedures, and storage conditions tailored to its purposes. Building a scientific basis for OF testing is on-going, with continuing OF cannabinoids research on passive environmental exposure, drug use history, donor physiological conditions, and oral cavity metabolism needed to better understand mechanisms of cannabinoid OF disposition and expand OF drug testing applicability.
Introduction
Psychoactive products derived from Cannabis sativa L. have been consumed for medicinal, recreational, and spiritual purposes throughout the world for over 5000 years.[1-2] Cannabis remains the most widely abused illicit drug around the globe, with an estimated 119-224 million cannabis users (2.6-5.0% of the world population) in 2010.[3] The increased availability (due to financial affordability, drug-policy changes, cultural tolerance, and/or commercial promotion and sale),[4-6] increased medicinal usage,[2, 7] and decrease in perceived risk of cannabis use contribute to its continued popularity.[8] Thus, it is not surprising that cannabis is one of the most frequently detected illegal drugs in drivers randomly stopped for roadside drug testing,[9-12] drivers involved in road traffic accidents,[13-15] chronic pain patients,[16-17] psychiatric patients,[18-19] emergency room patients,[20] athletes,[21] and in workplace drug testing.[22-25] Cannabis also accounted for an average 64, 38, 11, 20, and 41% of all reported individuals treated for drug abuse in Africa, the Americas, Asia, Europe, and Oceania, respectively, in 2001-2010.[26] In the US, 18% of admissions to publicly funded substance abuse treatment facilities in 2010 were for cannabis abuse, lower only than alcohol and opiates admissions.[27]
Cannabis contains over 500 different chemical compounds, including more than 100 cannabinoids.[28] Δ9-tetrahydrocannabinol (THC), the primary psychoactive constituent, mediates its pharmacological effects mainly through G protein-coupled central cannabinoid (CB1) receptors in the brain. Significant binding to the receptors in cerebellum, hippocampus, basal ganglia, and cerebral cortex correlates with cannabinoid effects on pain, cognition, memory, movement, and endocrine function.[29-30] In addition, CB1 receptors are present throughout the periphery including the heart, bladder, lung, thymus, uterus, testis, spleen, and gastrointestinal tract, with a wide range of functions associated with cannabinoid receptors.[31-32] THC also is a partial agonist of the peripheral cannabinoid (CB2) receptor, which modulates immune function[33] and bone mass.[34] There is evidence that THC acts as a dopamine reuptake blocker, indirectly interacts with μ and δ opioid receptors, and facilitates brain reward circuitry in the nucleus accumbens and ventral tegmental area.[35]
As a result of complex interactions with many neurological systems, cannabis produces multiple behavioral and physiological effects. Cannabis can induce euphoria, alter time perception, reduce concentration, sedate, impair cognition and memory, and produce dysphoric reactions (e.g., anxiety, psychosis, and panic attacks).[36-37] Common physiological effects include tachycardia, conjunctival reddening, dry mouth, appetite stimulation, vasodilation, and respiratory depression.[36] Potency and variety of cannabis, route of administration, co-administered drugs, users’ expectations of effects and drug intake history, and physiological condition can affect the severity and range of outcomes.[38-39] Some such effects are exploited for medicinal applications. Synthetic cannabinoids and cannabis plant extracts showed varied efficacy in treating cachexia, emesis, cancer and rheumatoid arthritis pain, neurological symptoms, neuropathic pain, cancer, glaucoma, and cannabis dependence.[40-43] Currently, two oral synthetic cannabinoids, dronabinol or synthetic THC, and nabilone are approved by the US Food and Drug Administration to treat appetite/weight loss in AIDS patients and nausea and vomiting in chemotherapy patients.[44] Sativex®, a whole-plant cannabis extract containing approximately equal proportions of THC and cannabidiol (CBD), is an oromucosal spray administered via sublingual and buccal mucosal surfaces. Sativex is approved in Canada, the UK, Spain, Germany, Denmark, and New Zealand to treat multiple sclerosis-related neuropathic pain and/or cancer pain resistant to opioid therapy. In the US, Sativex is in phase III clinical trials for the latter indication.[45-46]
Cannabinoid testing can include monitoring for THC, its metabolites [11-hydroxy-THC (11-OH-THC), 11-nor-9-carboxy-THC (THCCOOH), conjugated cannabinoids], and/or minor cannabinoids [CBD and cannabinol (CBN)]. Having different pharmacokinetic characteristics, quantification of multiple cannabinoids provides valuable information for interpreting cannabinoid test results in driving under the influence of drugs (DUID), workplace, cannabis dependence treatment, criminal justice, and pain management settings.
Because cannabinoids are usually the most prevalent analytes in illicit drug testing, it is evident that inclusion of a new alternative matrix, such as oral fluid (OF), demands sufficient scientific data to support sensitive and specific OF cannabinoid detection. With increasing interest in OF drug testing, research on OF cannabinoids proliferated since the 1990s. This review covers current knowledge on OF cannabinoids, starting from OF as a drug testing matrix to field application and controlled drug administration findings, evaluating pharmacokinetic properties, detection windows, and correlation with other biological matrices. Other considerations for appropriate OF cannabinoid testing are discussed, including on-site screening technologies, confirmatory analytical methods, drug stability, and effects of sample collection procedure, adulterants and passive environmental exposure.
Oral Fluid Cannabinoid Testing
With advances in analytical technology, OF gained acceptance over the past decade as an alternative biological matrix for detecting drugs in forensic and clinical settings.[47-48] OF testing offers simple, non-invasive, observed specimen collection, making adulteration more difficult and eliminating the need for specialized collection facilities or same sex collectors.[25, 49] Other advantages include ease of multiple sample collections, lower biohazard risk during collection, identification of recent exposure, and stronger correlation with blood than urine concentrations.[50-52] These qualities could potentially be utilized in various drug testing programs to improve the public health and safety.
Driving under the Influence of Cannabis
Among randomly stopped, nighttime weekend drivers in the US (2007), 12.4% tested positive for illicit drugs in blood and/or OF,[9] whereas an average of 1.9% of drivers were estimated to use illicit drugs in 13 European countries (2007-2009)[12]; cannabis was the most commonly detected illicit drug in these nationwide roadside surveys with prevalence of 8.6 and 1.3%, respectively.[9, 12] Thus, cannabinoid testing is particularly important for investigating DUID and drug-related accidents. Cannabis-induced driving impairment is documented in laboratory investigations, driving simulators, and on-the-road driving tests.[53-54] Acute THC/cannabis intoxication impaired driving-related psychomotor/neurocognitive performance, including time/distance perception,[55] tracking,[56-57] reaction time,[58-59] vehicle control (lane-position, speed, and steering variability),[59-61] and divided-attention.[55, 58] These data indicate that recent cannabis intake causes impairment similar to blood alcohol concentrations (BAC) at or above the legal limit (0.05 and 0.08 g/dL for many European countries and the US, respectively), contributing to increased risk of road traffic accidents. Indeed, cannabis was associated with higher culpability odds ratios for accidents, ranging from 1.3-2.7.[62-66] OF cannabinoid testing has advantages over urine testing by identifying psychoactive THC with a shorter detection window, and provides simpler and safer collection procedures than blood testing. Furthermore, roadside OF testing is increasingly important in regulating DUID (see “OF Cannabinoid Screening Techniques”).
Workplace Safety
In the workplace environment, Macdonald et al. reported that acute intoxication from cannabis smoking may impair employees’ performance for approximately 4 h, compromising workplace safety.[67] Drug testing is utilized for pre-employment screening and as a deterrent to drug use among employees.[68] The odds ratio of accident involvement for US aviation employees testing positive for drugs was 2.9, compared to those who tested negative; cannabis accounted for 67.3% of the illicit drug use episodes.[24] Cannabis was the most frequently detected drug (52-67% of positive urine/oral fluid results) among workers in the US, UK, Italy, and Brazil.[22-23, 25, 69] Impairment from acute cannabis intoxication leads to increased risks of driving and work-related accidents.[53, 67] Depending on cutoff criteria, OF cannabinoid testing may offer short detection windows reflecting the acute impairment window for accident investigations and also long detection windows for pre-employment screening and drug use prevention over the course of employment.
Public Health
Testing for cannabis is equally important in clinical practice, where cannabis is one of the most frequently detected illicit drugs in patients.[16] A high prevalence of cannabis consumption (6.2-59%) occurs in patients with chronic pain, multiple sclerosis, and HIV/AIDS, largely for pain relief and/or sleep improvement.[16, 70-74] Concurrent use of non-prescribed drugs can interfere with proper treatment; patients may develop a substance dependence disorder or tolerance, or experience adverse events due to interaction with prescribed drugs. Presence of unauthorized drugs also can indicate substitution for the prescribed drugs that may be diverted to illegal markets, or self-medication for an unidentified disorder.[75-76] Higher rates of illicit drug use (determined by urine drug testing for THCCOOH, benzoylecgonine, 6-acetylmorphine, MDMA, methamphetamine, and phencyclidine) were significantly associated with lower compliance with prescription medications for chronic pain.[77] Repeated drug testing reduced illicit drug use in chronic pain patients[17, 76]; cannabis use declined from 16 to 9%.[17] Self-reported drug use history may be unreliable,[78-81] making toxicological analysis essential for effective patient management. Cannabis dependence programs may utilize OF drug testing to monitor abstinence from cannabis and identify cannabis relapse.[82-83] In the case of cannabinoid pharmacotherapy, OF toxicology results can monitor patient compliance (see “Controlled Cannabis Administration”).
Athletic Performance
The World Anti-Doping Agency (WADA) prohibited cannabinoid use in-competition across all sports in 2004 when cannabinoids accounted for 15.7% of the adverse analytical findings reported by the WADA accredited anti-doping laboratories.[84] The prevalence decreased to 7.9% in 2011, possibly owing to a deterrent effect of testing under the 2004 WADA code.[85] In France, 42.4% of young athletes self-reported smoking cannabis several times in their lives and 12.5% used at least once to enhance athletic performance.[86] Athletes reported cannabis intake to relieve anxiety and stress associated with competition, to reduce pain, and to promote sleep quality and relaxation.[84, 86-87] The WADA International Standard for Laboratories currently states that results obtained from other biological matrices such as OF cannot counter adverse analytical findings from urine or blood.[88] OF can be a valid alternative matrix, particularly for cannabinoids as the agency prohibits cannabis use in-competition but not out of competition, necessitating short detection windows.
Oral Fluid as a Matrix for Drug Testing
OF plays an important role in maintaining tooth integrity, protecting against microorganisms and toxins, lubricating and cleaning oral tissues, and initiating digestion.[89] OF consists of more than 97% water, and electrolytes, immunoglobulins, enzymes and other proteins, such as glycoproteins, mucin, amylase, lipase, peroxidase and dehydrogenase.[89-90] Three major salivary glands (parotid, sublingual and submandibular), the gingival fold, oral mucosa transudate, minor accessory salivary glands, and secretions from the nasal cavity and pharynx contribute to OF composition. OF also contains bacteria, epithelial cells, erythrocytes, leukocytes, and food debris.[91-93] Many hormones and enzymes in plasma are present in OF, albeit in lower concentrations, as compounds are transferred via the mucosal and gingival crevices from blood capillaries.[91, 94] Expression of cytochrome P450 enzymes, potentially involved in cannabinoid metabolism, also was identified in human oral tissue cells.[95-98]
THC undergoes extensive hepatic cytochrome P450 metabolism, producing more than 100 metabolites.[99] CYP2C9 primarily oxidizes THC to psychoactive 11-OH-THC, while other cytochrome P450 enzymes (e.g., CYP2C19 and CYP3A4) are involved in additional THC oxidation.[100] 11-OH-THC is further oxidized by microsomal alcohol dehydrogenase and aldehyde oxygenase (CYP2C subfamily) to produce the non-psychoactive metabolite, THCCOOH.[101-102] Phase II conjugation with glucuronic acid and less commonly, glutathione, sulfate, and others to the carboxyl group of THCCOOH increases water solubility, facilitating urinary excretion.[99, 101] Extra hepatic tissues such as heart, lung, brain, and intestine also metabolize cannabinoids, although to a much lower degree.[103-106] Whether oral tissue similarly metabolizes cannabinoids is an important question for OF cannabinoid research as it could affect OF cannabinoids’ pharmacokinetic properties, correlation with blood concentrations, and inter-subject variability.
Healthy adults produce approximately 0.5-1.5 L of OF per day.[89] OF pH ranged from 6.2 to7.4; OF becomes more basic when stimulated owing to the loss of dissolved carbon dioxide.[89, 107-108] OF composition and flow rate are influenced by the circadian cycle, sensory stimuli, hormonal changes, mechanical stimulation, psychological status (e.g. anger, fear, and depression), genetics, oral hygiene, sympathomimetic and parasympatholytic (anticholinergic) drugs, and systemic diseases (e.g. diabetes, kidney dysfunction, anorexia, cystic fibrosis).[91, 109] In turn, drug transfer into OF is affected by OF composition, flow rate, and pH, the drug’s pKa, protein binding, lipophilicity, spatial configuration, and molecular weight and blood pH.[50, 108] Creatinine is widely utilized to normalize urine sample volume.[110-111] Evaluation of potential biomarkers to indicate collection of representative (as opposed to diluted) OF sample volume has so far met with less success. OF creatinine concentrations showed large intra- and inter-subject variation; CV over 10-weeks was 141% (range 39-225).[112-113] OF IgG concentrations ≥0.1-1.0 mg/L were suggested, but even after a second rinse of the mouth with tap water, IgG concentrations still exceeded this criterion.[108]
When cannabis is smoked, inhaled, or sprayed into the mouth, the oral mucosa is extensively contaminated for a short time after intake.[114-115] Contamination increases OF THC detection, but reduces correlation with blood concentrations.[51] Contribution of cannabinoids from blood is minimal; depots in the oral cavity from external exposure are the primary source of THC OF concentrations.[114, 116] CBD is not psychoactive but has potential therapeutic applications[117]; some investigators suggest that CBD may have anxiolytic[118] and anti-psychotic[119] properties and possibly attenuates THC-induced effects.[120-121] CBN, a degradation product of THC oxidation, is approximately 10% as potent as THC, and increases as cannabis plant material ages.[122-123] Like THC, the source of these minor cannabinoids in OF is primarily from cannabis smoke.[124-125] In contrast, THCCOOH results from THC hepatic metabolism and is not present in cannabis smoke. [124, 126-127] THCCOOH also was not produced from THC incubated in OF at 37°C for 24 h.[126] Thus, metabolite concentrations in OF are influenced by blood concentrations and factors affecting analyte passage from blood into OF. No study, of which we are aware, documented cannabinoid metabolism in the oral mucosa. However, enzyme hydrolysis by β-glucuronidase or sulfatase produced mean 48.2% and 8.1 % increases, respectively, in OF THCCOOH (n = 1 in 4 sessions).[128] Mean OF conjugated to free THCCOOH ratio was 1.9 (CV 22.6%). Some glycoproteins and enzymes that could be involved in cannabinoid metabolism were identified in human saliva.[109, 129] UDP-glucuronosyltransferase has yet to be detected in OF, so whether Phase II metabolites are transferred from blood and/or metabolized in OF remains unclear.
Effects of cannabis smoking on oral physiology could be an additional factor. Cannabis reduces activity of the parasympathetic nervous system, inducing dry mouth (xerostomia).[130] This creates difficulty collecting a sufficient volume of OF, particularly within the initial hour after cannabis smoking.[114, 130-131] Another common oral condition associated with cannabis smoking is leukoedema (developmental alteration of the oral mucosa),[130, 132] but its effect on cannabinoid OF disposition is unknown. Blood in the oral cavity from infection, traumatic damage, stomatitis or other causes can also affect cannabinoid OF concentrations.[114, 131-132]
Regulatory Status of Cannabinoid OF Testing
DUID laws in the US differ by state. The type of biological matrix that law enforcement officers are authorized to collect also varies, but generally includes blood and/or urine. As of December 2008, 6 states (Colorado, Missouri, New York, North Dakota, Oklahoma, and Utah) permit OF testing as well.[133] “Other bodily substances” are allowed in 9 additional states (Alabama, Arizona, Georgia, Indiana, Kansas, Louisiana, North Carolina, Ohio, and South Dakota) and Puerto Rico.[133] In Canada, the federal Criminal Code stipulates OF collection to evaluate the presence of drugs in a person’s body while operating a vehicle/vessel/aircraft/railway equipment.[134] Several other countries permit either OF screening and confirmation (Belgium, Australia, and Spain) or OF screening and blood confirmation (France, Germany) or have such laws pending (Norway) for DUID investigations.[10]
For the US federal workplace, OF drug testing is not authorized, but has been proposed in the Mandatory Guidelines since 2004[135] and is increasingly utilized in state and private sector workplaces.[136-137] In Australia, the Australian Standard AS4760 was developed in 2006, specifying OF collection and analysis procedures for workplace drug testing.[138] OF also is incorporated in some Canadian workplace drug testing programs[139] and is proposed by the European Workplace Drug Testing Society.[140] THC OF cutoffs specified or proposed by countries and organizations for DUID and workplace drug testing programs are listed in Table 1.
Table 1.
Cutoff concentrations for Δ9-tetrahydrocannabinol in oral fluid as specified or proposed for driving under the influence of drugs (DUID) and workplace drug testing programs.
| Agency | Purpose | Screening Cutoff, μg/L | Confirmatory Cutoff, μg/L | Ref. |
|---|---|---|---|---|
| Australia | DUID | 30 (DrugWipe®) | 2 | [141] |
| 50 (RapiScan™) | ||||
| Belgium | DUID | 25 | 10 | [10] |
| DRUID | DUID | 1 | [12] | |
| Francea | DUID | 15 | [10] | |
| Talloires | DUID | 2 | [226] | |
| AS4760 | Workplace | 25 | 10 | [138] |
| EWDTS | Workplace | 10 | 2 | [140] |
| SAMHSA | Workplace | 4 | 2 | [135] |
AS4760 – Australian Standard 4760-2006; DRUID – Driving under the Influence of Drugs, Alcohol and Medicines; EWDTS – European Workplace Drug Testing Society; SAMHSA – Substance Abuse and Mental Health Services Administration
blood samples are utilized for confirmation
Field Application of OF Testing
The high prevalence of cannabinoids detected in OF during roadside, clinical, and workplace drug testing (Table 2) emphasizes the importance of building a scientific basis for OF cannabinoid testing. Cannabis frequently accounted for a major portion of OF samples positive for illicit drugs during random roadside (27.8-77.3%),[5, 9, 11, 141-143] clinical (11.5-46.3%),[144-145] and workplace (23.8-63.6%)[25, 146] drug testing studies. THC, CBD, and CBN concentrations in those OF samples were as high as 6484, 115, and 124 μg/L, respectively, whereas THCCOOH and 11-OH-THC were ≤400 ng/L and 12.3 μg/L, respectively (Table 2). Thus, a linear dynamic range tailored to each analyte is needed. Dilution integrity and carryover experiments during method validation should also be performed over a wide concentration range. Assessing sample collection procedures, evaluating performance of screening techniques, and validating confirmatory methods are essential for accurate cannabinoid quantification in OF samples collected in practice.
Table 2.
Field application of oral fluid cannabinoid testing in roadside, clinical, and workplace settings
| Type | Location | Yeara | N (N+)b | OF sample | Cannabinoid results | # other drugs tested | Ref. | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Collection | Analysis | Analyte (cutoff, μg/L)c | % positived | Concentration,μg/L | ||||||
| DI | France | 2000g | 198 | Salivette | GC-MS | THC (1 ng/device) | 7.1 (of total samples analyzed) | 1-103 ng/device | - | [227] |
| W | USA | 2001 | 77218 (3908) | Intercept | Immunoassay GC-MSMS | Screen (3); THC (1.5) | 63.6 | ≥1.5-50 | 7 | [25] |
| DR | Australia | 2004 | 13176 (313) | RapiScan | Onsite device GC-MS | Screen (30, DrugWipe; 50, RapiScan) THC (2) | 27.8 | 5-6484 | 6 | [141] |
| C/W | USA | 2004-2006 | 635000 (8679) | Intercept | Immunoassay GC-MS/MSMS | Screen (1); THC (0.25/0.5); CBD (0.25/1); CBN (0.25/1); 11-OH-THC (0.025/1); THCCOOH (0.025/1)e | 8.4 (cannabinoids total); 8.2 (THC); 3.4 (CBD); 3.0 (CBN); 0.5 (11-OH-THC); 0.9 (THCCOOH) | 0.3-382 (THC); 0.3-115 (CBD); 0.2-124 (CBN); 0.01-12.3 (11-OH-THC); 0.03-0.4 (THCCOOH) | 24 | [157] |
| DR | Norway | 2005-2006 | 10816 | Intercept | LC-MSMS | THC (1) | 0.6 (of total samples analyzed) | - | 30 | [228] |
| DR | Australia | 2007 | 781 (27) | RapiScan | Immunoassay GC-MS | - | 48.1 | - | Not specified | [142] |
| DR | USA | 2007 | 7719 (700) | Quantisal | Immunoassay GC-MS/LC-MSMS | Screen (4) THC (2) | 77.3 | - | 74 | [9] |
| DR | Denmark | 2008-2009 | 3002 (85) | Saliva-Sampler | LC-MSMS | THC (0.53) | 47.1 | 0.67-2280 | 28 | [143] |
| DR | Brazil | 2008-2009 | 2235 (172) | Quantisal | LC-MSMS | THC (1.04); CBN (1.3) | 7.6 (THC); 5.2 (CBN) | > 0.52-65.5 (THC); > 0.52-7.8 (CBN) | 30 | [229] |
| DR | Norway | 2008-2009 | Truck: 882 (10); Car/Van: 5305 (108) | Saliva-Sampler | LC-MSMS | THC (1) | Truck: 60.0 Car/Van: 73.1 | - | 28 | [230] |
| C | USA | 2009 | 100 | Quantisal | LC-MSMS | THC (1) | 6 (of total samples analyzed) | 2.1-72.5 | 33 | [168] |
| DR | Australia | 2009-2010 | 853 (815) | RapiScan | LC-MSMS | THC (10) THCCOOHf | 44 | - | 29 | [11] |
| C | USA | 2010 | 6441 (741) | Quantisal | Immunoassay LC-MSMS | Screen (4); THC (2); THCCOOH (2) | 46.3 (THC); 0 (THCCOOH) | 2.0-955.8 | 38 | [144] |
| W | Norway | 2010g | 524 (21) | Saliva-Sampler | LC-MSMS | THC (0.31) | 23.8 | 6-1102 | 26 | [146] |
| DR | USA | 2010 | 893 (111) | Quantisal | Immunoassay GC-MS/LC-MSMS | Screen (4); THC (2) | 73.9 | - | 13 | [5] |
| S | Sweden | 2011 | 396 (40) | Quantisal | LC-MSMS | THC (1) | 15 | - | 4 | [231] |
| C | Germany | 2012g | 939 (26) | Dräger DrugTest | Onsite device | Screen (5) | 11.5 | - | 4 | [145] |
OF – oral fluid; C – clinical setting; DR – randomly selected roadside; DI – injured drivers; S – on a cruise ship; W – workplace; CBD – cannabidiol; CBN – cannabinol; 11-OH-THC – 11-hydroxy-THC; THC – Δ9-tetrahydrocannabinol; THCCOOH – 11-nor-9-carboxy-THC; GC – gas chromatography; LC – liquid chromatography; MS – mass spectrometry
year of sample collection unless otherwise specified
N = number of total oral fluid samples analyzed; N+ = number of oral fluid samples positive for at least one illicit drug
analyte confirmation cutoffs except Screen = cutoff for cannabinoid immunoassay
THC positives among all positive results unless otherwise specified
first cutoff value is for treatment samples and the second cutoff value is for workplace samples
THCCOOH data are not presented
year of publication
Controlled Cannabis Administration
Controlled drug administration studies provide rigorous scientific data to aid in interpreting OF test results. Research findings must be interpreted in the context of study design; cannabinoid OF disposition is influenced not only by pharmacokinetic properties, but also by administered dose, participants’ cannabis use history, and efficiency of collection and quantification procedures. Controlled cannabis administration studies are summarized in Table 3. OF collection methods are described in detail in the later section “OF Collection.”
Table 3.
Oral fluid cannabinoid results after controlled cannabis administration
| Routea | THC doseb mg | OF collectionc h | Participants | OF samples | Cannabinoid results | Ref. | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| n | Smoking habitd | Collection | Analysis | LOQ, μg/L | Cinitial, μg/Le | Clast, μg/Lf | Last detection, h | ||||
| S | S, 11 | 0.33-4 | 13 | O | Expect | GC-MS | THC (not reported) | >1000g | ~10g | 4g | [152] |
|
| |||||||||||
| S | S, Low: 15.8, High: 33.8 | 0.2-24 | 6 | - | Expect | RIA | THC (1)h | Low: 864, High: 4167 | Low: 0 | Low: 4-6 | [51] |
| High: 0.3 | High: 2-24 | ||||||||||
|
| |||||||||||
| S | S, 54 | 0.25-22 | 10i | C | Expect | 2D-GC-MS | THC (0.25), CBN (1), CBD (0.25), THCCOOH (0.005) | THC: 4577 (6794), CBN: 382 (606), CBD: 218 (305), THCCOOH: 0.257 (0.209) | THC: 3.6 (4.0), CBN: 0, CBD: 0.1 (0.1), THCCOOH: 0.015 (0.010) | THC: 6-22, CBN: 1-6, CBD: 1-22, THCCOH: 4-22 | [131] |
|
| |||||||||||
| S | S, 20-25 | 1-72j | 5 | C | Intercept | GC-MSMS | THC (0.2) | Left: 27.8 (6.2), Right: 22.6 (6.2) | Left: 0.6 (0.5), Right: 0.6 (0.6) | 16-72 | [148] |
|
| |||||||||||
| S | S, 20-25 | 1-72j | 5 | O | Intercept | GC-MSMS | THC (0.2) | Left: 23.3 (7.9), Right: 25.3 (6.5) | Left: 0.2 (0.2), Right: 0.3 (0.3) | 4-72 | [148] |
|
| |||||||||||
| S | S, 20-25 | 0.25-1.75 | 5 | O | Intercept | GC-MSMS | THC (0.2) | Left: 80.6 (37.7), Right: 59.4 (21.6) | Left: 7.9 (4.1), Right: 9.6 (3.0) | 1.75 | [148] |
|
| |||||||||||
| S | S, 39.5 | 0-8k | 4 | O | Intercept | GC-MSMS | THC (0.75) | Left: 484 (438), Right: 461 (290) | Left: 2.6 (1.7), Right 4.1 (2.6) | 8 | [224] |
|
| |||||||||||
| S | S, 83.2 | 0-8 | 4 | O | Intercept | GC-MSMS | THC (0.75) | 149 (169) | 2.1 (1.0) | 8 | [224] |
|
| |||||||||||
| S | S, Low: 13.8-22.3, High: 27.5-44.5 | 0.25-6 | 10 | O | Intercept | GC-MS | THC (0.5) | Low: 900 (589), High: 1041 (652) | Low: 13.8 (11.6) High: 22.2 (12.1) | 6 | [116] |
|
| |||||||||||
| S | S, 22.5-47.5 | 0.08-8 | 12 | O | Intercept | GC-MS | THC (2.4) | 1242 (397-6438)k | 6.3 (0-25.8)l | 8 (82%)l | [147] |
|
| |||||||||||
| S | S, 22.5-47.5 | 0.08-8 | 12 | C | Intercept | GC-MS | THC (2.4) | 6202 (387-71747)k | 11.3 (0-38.8)l | 8 (91%)l | [147] |
|
| |||||||||||
| S | S | 0.5-24 | 3 | C | Quantisal | GC-MS | THC (0.5), CBN (0.5), CBD (1), THCAA (1) | THC: 75.3 (21.1), CBN: 2.6 (2.2), CBD: 0, THCAA: 13.9 (9.4) | THC: 0.4 (0.5), CBN: 0, THCAA: 0 | THC: 4-24, CBN: ND-2, THCAA: 4-8 | [154] |
|
| |||||||||||
| S | S | 0.5-48 | 1m | C | Quantisal | 2D- GC-MS | THC (0.5), THCCOOH (0.002) | THC: 80 (15- > 2000) | THC: 0 | THC: 2-24, THCCOOH: 48 | [128] |
| THCCOOH: 0.043 (0.024-0.079) | THCCOOH: 5-77 | ||||||||||
|
| |||||||||||
| S | S, 54 | 0.25-22 | 10i | C | Quantisal | 2D-GC-MS | THC (0.5), CBN (1), CBD (0.5), THCCOOH (0.075) | THC: 1687 (3063), CBN: 202 (478), CBD: 86 (177), THCCOOH: 0.136 (0.188) | THC: 2.6 (2.1), CBN: 0, CBD: 0, THCCOOH: 0.037 (0.038) | THC: 6-22, CBN: 2-6, CBD: 2-6, THCCOH: 6-22 | [114] |
|
| |||||||||||
| OC | S, 20-25 | 1-72j | 3 | O | Intercept | GC-MSMS | THC (0.2) | Left: 3.4 (3.0), Right: 5.0 (2.5) | Left: 0.5 (0.8), Right: 0.2 (0.4) | 4-72 | [148] |
|
| |||||||||||
| OTHC | M, 20 | 1-185 | 10 | C | Expect | 2D-GC-MS | THC (0.25), CBN (1), CBD (0.25), THCCOOH (0.005) | After 1st dose, THC: 0 (0-2.9), CBN: 0, CBD: 0, THCCOOH: 0.030 (0-0.248)m | After 37th dose, THC: 0 (0-0.6), THCCOOH: 0.096 (0.005-1.387)m | THC: ND-185 | [150] |
| THCCOOH: 185 | |||||||||||
|
| |||||||||||
| OTHC | M, 20 | 1-185 | 10 | C | Quantisal | 2D-GC-MS | THC (0.5), CBN (1), CBD (0.5), THCCOOH (0.075) | After 1st dose, THC: 0.7 (0-6.8), CBN: 0, CBD: 0, THCCOOH: 0.029 (0-0.557)n | After 37th dose, THC: 0, THCCOOH: 0.135 (0.025-1.056)n | THC: -18-149.5 | [158] |
| THCCOOH: 185 | |||||||||||
|
| |||||||||||
| OTHC | S, Low: 5, High: 15 | 0.25-10.5 | 14 | C-O | Quantisal | 2D-GC-MS | THC (0.5), CBN (1), CBD (0.5), THCCOOH (0.075) | Low, THC: 2.4 (4.0), CBN: 0, CBD: 0, THCCOOH: 0.032 (0.053) | Low, THC: 0.7 (1.3), CBN: 0, CBD: 0, THCCOOH: 0.032 (0.056) | THC: 0.25-10.5, CBN: ND, CBD: ND-1, THCCOOH: 4.5-10.5 | [115] |
| High, THC: 2.6 (4.9), CBN: 0, CBD: 0.1 (0.2), THCCOOH: 0.040 (0.075) | |||||||||||
| High, THC: 0.7 (1.8), CBN: 0, CBD: 0, THCCOOH: 0.054 (0.086) | |||||||||||
|
| |||||||||||
| St | S, Low: 5, High: 15 | 0.25-10.5 | 14 | C-O | Quantisal | 2D-GC-MS | THC (0.5), CBN (1), CBD (0.5), THCCOOH (0.075) | Low, THC: 3293 (3262), CBN: 156 (146), CBD: 3384 (3442), THCCOOH: 0.059 (0.081) | Low, THC: 21.8 (16.7), CBN: 0.7 (0.9), CBD: 24.4 (19.3), THCCOOH: 0.033 (0.047) | THC: 10.5, CBN: 4.5-10.5, CBD: 10.5, THCCOOH: 0.25-10.5 | [115] |
| High, THC: 7678 (5285), CBN: 559 (547), CBD: 7136 (5022), THCCOOH: 0.017 (0.034) | High, THC: 41.1 (28.1), CBN: 2.4 (2.0), CBD: 40.6 (36.2), THCCOOH: 0.035 (0.049) | ||||||||||
Studies may have multiple sections differing in participants’ smoking habits, dose, collection duration or method, and thus are described in multiple rows
OF – oral fluid; Expect – expectoration; CBD – cannabidiol; CBN – cannabinol; THC – Δ9-tetrahydrocannabinol; THCCOOH – 11-nor-9-carboxy-THC; GC – gas chromatography; LC – liquid chromatography; MS – mass spectrometry, LOD – limit of detection; LOQ – limit of quantification
S – Smoked cannabis, OC – Oral cannabis, OTHC – Oral THC, St – Sativex
S – Single dose, M – Multiple doses
OF collection after dosing
C – Chronic smokers, O – Occasional smokers; the two groups are approximately defined. Refer to original studies for detailed smoking habit of the participants
Cinitial – Concentration at the first collection time; mean (SD) unless otherwise specified. Concentrations < LOQ are considered zero
Clast – Concentration at the last collection time; mean (SD) unless otherwise specified. Concentrations < LOQ are considered zero
exact concentrations not reported
LOD
n = 6 at 22 h
Participants’ abstinence from cannabis smoking was not monitored after 4 h post smoking
OF samples before 0.75 h were collected inside the closed van
Median (range) ng/g; last detection times of 1-2 participants were not reported
1 participant completed 4 smoking sessions
Median (range)
Smoked Cannabis Administration
Maximum THC concentrations generally occur in the first OF sample collected following smoked cannabis with concentrations often > 1000 μg/L (Table 3; Figure 1). Multiple factors contribute to the wide THC concentration range within and between studies: 1) Higher potency cannabis led to higher initial concentrations due to more extensive oral cavity contamination. Fifteen min after smoking 13.8-22.3 and 27.5-44.5 mg THC cigarettes, mean THC concentrations were 900 and 1041 μg/L in Intercept® OF samples, respectively.[116] 2) Chronic cannabis smokers may have higher initial concentrations than occasional smokers due to more efficient smoking topography and/or tolerance development. Toennes et al. reported that chronic cannabis smokers had significantly higher Intercept® OF THC maximum concentrations (mean 12457 ng/g) than occasional smokers (1715 ng/g) despite body weight normalized doses (500 μg/kg THC cigarettes).[147] After smoking a 54 mg THC cigarette, maximum Quantisal™ OF sample concentrations were higher in individuals who smoked ≥10 years (mean 3122 μg/L) than in those who smoked <10 years (344 μg/L). On the other hand, Niedbala et al. reported no significant difference in Intercept® OF THC initial concentrations (mean 27.8 vs. 23.3 μg/L) between chronic and occasional smokers.[148] However, first collection was 1 h after smoking. Concentration differences between chronic and occasional smokers rapidly diminished after the initial elimination phase.[147] 3) OF collection method could affect cannabinoid quantification. With 54 mg THC cigarettes, 1733 and 4577 μg/L mean maximum THC concentrations were found in concurrently collected Quantisal™ and expectorated OF samples, respectively.[131, 149] Higher concentrations in expectorated OF could be due to cannabinoids trapped in mucus/pellet; the analytical method included addition of water and cold acetonitrile and then vortexing and centrifugation which could release analytes prior to SPE.[150] When OF samples were concurrently collected from 40 volunteers by expectoration and with the Salivette® device 10-25 min after smoking, expectorated OF samples had higher THC concentrations (51-6552 vs. 8-134 μg/L) and detection rate (100 vs. 47%).[151] The researchers subsequently observed significant THC adsorption to the Salivette® cotton roll.[151] Conversely, when specimens were collected by expectoration, it was more difficult to collect sufficient sample volume,[114, 131] analytes were less stable [149] and there was greater variability in quantification.[131] 4) Cannabinoid concentrations show large inter-subject variability. Standard deviations in these studies were comparable or higher than mean values.[57, 114, 116, 147] Participants had THC concentrations 0.25 h post smoking as low as 248, 265, and 68 μg/L and as high as 2544, 22370, and 10284 μg/L in Intercept® (27.5-44.5 mg THC), expectorated (54), and Quantisal™ (54) OF samples, respectively.[114, 116, 131]
Figure 1.
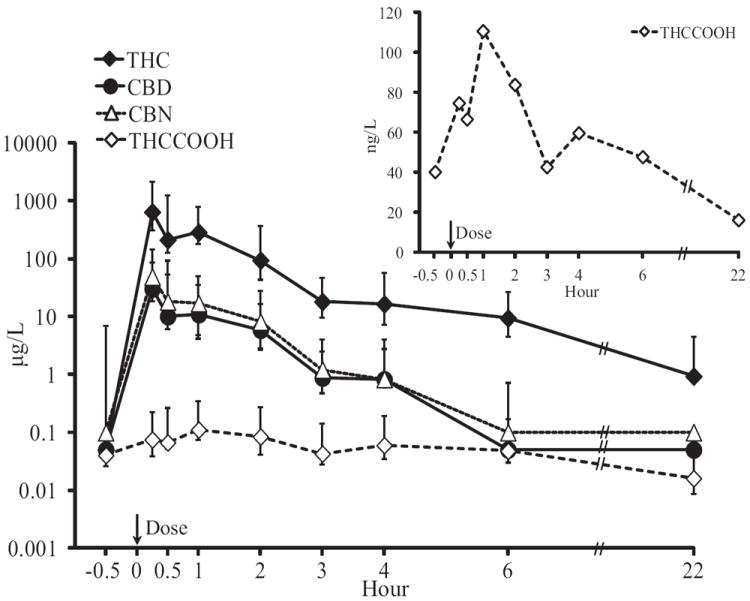
The THC elimination profile is biphasic; concentrations rapidly decrease within the first 1-2 h post smoking, and then decline more gradually, with low concentrations detectable for days in chronic smokers.[51, 116, 152-153] THC concentrations above 1000 μg/L generally decreased below 50 μg/L by 6 h [114, 116, 131] and < 10 μg/L within 22-24 h post smoking.[114, 128, 131, 148] Last THC detection times up to 72 h were reported with concentrations ≤1.3 μg/L[148]; however, in this outpatient study, participants’ cannabis abstinence was not monitored after 4 h post smoking.[148] In chronic cannabis smokers during extended, monitored abstinence, median THC detection window was 24 h (95% CI 4.8-43.2 h), but occasional positives occurred for up to 28 days, with concentrations ≤3 ng/mL.[153] Dose and cannabis smoking history had much less influence on concentrations after the initial ≤0.5 h collection; similar mean THC elimination half-lives of 1.5-1.6 (range 0.8-3) h were observed after 2 different smoked doses[116] and in chronic vs. occasional smokers.[147] Mean THC concentration 8 h post smoking was non-significantly higher in chronic smokers than occasional smokers (16.1 vs. 8.0 ng/g).[147] However, the initial amount of THC deposited in the oral cavity can influence THC’s detection windows. For example, in Quantisal™ OF samples, 2 of 3 participants reporting cannabis intake <10 years had THC < LOQ 22 h post smoking, whereas all 3 participants reporting cannabis intake ≥10 years were still THC-positive.[114]
Minor cannabinoids are present in lower concentrations in cannabis smoke, and thus, achieve lower maximum concentrations and shorter detection windows than THC. After smoking a cannabis cigarette containing approximately 2.0 mg CBD and 1.7 mg CBN, OF CBD and CBN concentrations were about 10-fold lower than THC, with mean maximum concentrations of 89.1-204 and 218-425 μg/L in Quantisal™ and expectorated OF samples, respectively.[114, 131] As the source of CBD and CBN in OF is the same as THC, CBD and CBN concentrations were strongly correlated with those of THC over time. No OF samples were positive for CBD or CBN beyond 6 h except 1 expectorated OF sample with CBD concentration at 0.3 μg/L 22 h post smoking.[114, 131] During up to 33 days of abstinence with OF collection every 24 h, CBD and CBN were detected only at admission.[153] Moore et al. reported maximum CBN and Δ9-tetrahydrocannabinolic acid (THCAA) concentrations of ≤4.1 and 20 μg/L, respectively, lower than THC concentrations (≤93 μg/L) after smoking a single cannabis cigarette.[154] Last detection times of CBN and THCAA were ≤2 and 8 h, respectively.[154] CBD was not detected in any OF samples, likely due to low content in cannabis cigarettes.[154]
OF THCCOOH increases were not as rapid as parent cannabinoids after smoking and showed a more delayed elimination time-course.[114, 131] In controlled smoked cannabis administration studies, OF THCCOOH concentrations were significantly confounded by baseline concentrations in chronic frequent cannabis smokers, interfering with accurate evaluation of the elimination time course.[114, 131, 155] As expected, THC and THCCOOH concentrations were not significantly correlated from 0.25 to 6 h after smoking because of different mechanisms of entry into OF.[114] During monitored abstinence from chronic frequent cannabis smoking, THC concentrations also were not significantly correlated to THCCOOH concentrations on admission; however, after 24 h, OF THC and THCCOOH concentrations were significantly correlated (r = 0.428; P = 0.023), possibly due to dissipation of oral cavity contamination.[153] THCCOOH detection window was often longer than THC’s in chronic cannabis smokers, due to its lower limit of quantification (LOQ) and metabolism of residual THC released from body stores; median THCCOOH detection window was 13 days (95% CI 6.4-19.4 days), with occasional positives up to 29 days.[153] THCCOOH concentrations never exceeded 320 ng/L after smoking a single cannabis cigarette, except for one participant who had blood in his OF samples. THCCOOH concentrations in those bloody OF samples were up to 763 and 3519 ng/L in Quantisal™ and expectorated OF samples, respectively.[114, 131] OF specimens contaminated with blood should not be used for cannabinoid quantification, particularly for THCCOOH because of large differences in THCCOOH concentrations between OF and blood.[114, 156] Mean OF glucuronide and sulfate THCCOOH conjugates are estimated at 48.2 and 8.1% of free THCCOOH, respectively, suggesting that hydrolysis of OF samples would increase THCCOOH detection rate.[128]
With a 0.5 μg/L LOQ, 11-OH-THC was not detected in any Quantisal samples after smoking,[114] but 4 expectorated OF samples were positive for 11-OH-THC at an LOQ of 0.25 μg/L; concentrations were 0.3-1.3 μg/L, occurring within 2 h post smoking.[131] Cone et al. found THCCOOH and 11-OH-THC in 10.8 and 5.7% of 725 cannabinoid-positive OF samples collected in treatment/workplace drug testing programs, respectively[157]. Concentration ranges were 30-400 ng/L for THCCOOH and 10-12300 ng/L for 11-OH-THC. These findings imply the potential for 11-OH-THC as another valuable analyte to monitor in OF.
Oral THC Administration
Oral mucosal contamination by encapsulated oral THC and orally ingested cannabis was minimal (Figure 2).[148, 158] Cannabis-laced (20-25 mg THC) brownies produced ≤7.1 μg/L peak OF THC concentrations 1-2 h after intake.[148] THC concentrations decreased over 8 days following a total of 37 oral 20 mg THC doses and were never above 8.0 μg/L in Quantisal OF samples.[158] In concurrent expectorated OF samples, mean THC concentrations decreased 92.4% from admission to the first dose; THC was ≤10.3 μg/L after the first THC dose.[150] Similarly, after single 5 and 15 mg oral THC doses in less than daily cannabis smokers, THC OF concentrations significantly decreased over time, co-varied with baseline concentrations, and were not significantly different from those after placebo doses.[115] Detection rates of CBD and CBN were even lower; positives were due to previously self-administered smoked cannabis and generally occurred before dosing, with concentrations ≤0.8 μg/L after dosing.[115, 150, 158]
Figure 2.
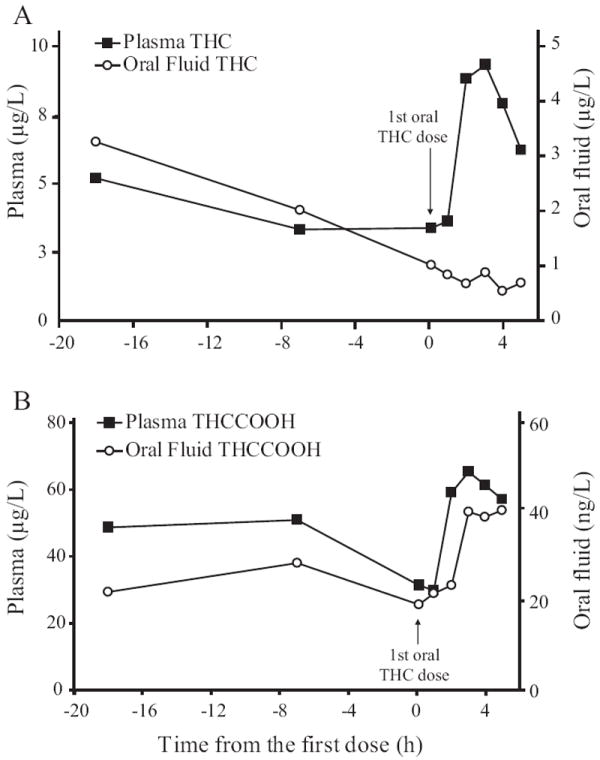
THCCOOH, on the other hand, significantly increased over time during around-the-clock oral THC administration (Figure 2),[158] although concentrations never exceeded 1118 and 1390 ng/L in Quantisal™ and expectorated OF samples, respectively.[150, 158] OF THCCOOH was the primary analyte detected during around-the-clock oral THC dosing, with most samples positive throughout the study.[150, 158] However, after single 5 and 15 mg oral THC doses, THCCOOH concentrations were not significantly different over time, likely due to the low dose and large contribution from baseline THCCOOH concentrations.[115] THCCOOH OF concentrations were nonetheless significantly higher after 15 than 5 mg oral THC and placebo doses, indicating oral THC contribution to THCCOOH OF concentrations.[115] THCCOOH concentrations were lower in less than daily cannabis smokers than in daily smokers. In fact, in some occasional smokers OF was never positive for THCCOOH throughout the study.[115] 11-OH-THC was not detected in any Quantisal™ sample after around-the-clock 20 mg oral THC for 8-days or single 5 and 15 mg oral THC dosing.[115, 158] Interestingly, one expectorated OF sample was positive for 11-OH-THC (0.5 μg/L), 161 h after the first THC dose, the time of the highest THCCOOH concentrations.[150]
Such lack of measurable OF parent cannabinoids implies that sudden increase in OF parent cannabinoids might be employed to identify relapse to smoked cannabis intake during oral THC treatment. To monitor compliance, OF THCCOOH would be a better marker than OF parent cannabinoids; however, concentrations will be influenced by cannabis use history and dosing regimen.
Sativex® Administration
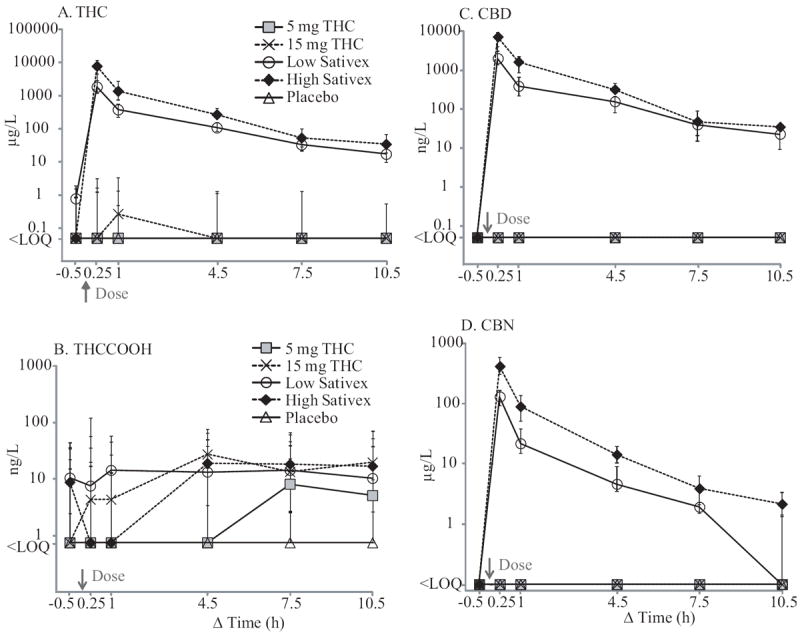
Following administration of 2 (low dose; 5.4 mg THC and 5.0 mg CBD) and 6 (high dose; 16.2 mg THC and 15.0 mg CBD) Sativex actuations, THC and CBD OF concentrations were highly increased, along with 10-fold lower CBN concentrations (Figure 3).[115] Elimination profiles were similar to those after cannabis smoking except that CBD concentrations were as high as THC. Median THC, CBD, and CBN peak concentrations after low-dose Sativex were 1815, 1975, and 140 μg/L, respectively, whereas high-dose Sativex produced higher medians of 7853, 7129, and 414 μg/L, respectively. Maximum concentrations generally occurred in the first OF samples, 15 min post-dose.[115] These results reflect approximately equal proportions of THC and CBD in Sativex. After Sativex dosing, THC and CBD were detected until 10.5 h, the last collection time, while CBN last detection times were 4.5-10.5 h.[115] THCCOOH OF concentrations increased over time only after high-dose Sativex and were significantly confounded by baseline concentrations, as with other routes of administration (Figure 3).[115] 11-OH-THC was detected in only 4 Quantisal™ OF samples collected within 1 h post-dose, with concentrations ≤2.8 μg/L.[115] High CBD concentrations after Sativex led to median OF CBD/THC ratios of 0.82-1.34 over the collection period, much higher than those after smoked cannabis, 0.04-0.06.[115] This difference could be useful for documenting compliance during Sativex pharmacotherapy. Conversely, the high CBD/THC ratio would not be altered sufficiently to identify single smoked cannabis relapses for more than a short time. Cannabis strains with high CBD content [28] might also produce higher CBD/THC ratios.
Figure 3.
Correlation with Other Biological Matrices and Impairment
An advantage of OF drug testing is greater correlation with blood concentrations compared to urine, suggesting that OF concentrations may better reflect the impairment window.[49]
OF and Blood Cannabinoids
After smoking a cannabis cigarette (6.8% THC), median whole blood (plasma) maximum concentrations were 50 (76), 1.3 (2.0), and 2.4 (3.6) μg/L for THC, CBD, and CBN, respectively[156] These cannabinoids maximum concentrations were much higher in simultaneously collected Quantisal™ OF specimens (644, 30.4, and 49.0 μg/L, respectively) although Tmax was 0.25 h post smoking initiation (the first collection) in both matrices.[114] In contrast, metabolite concentrations were more than 1000-fold higher in blood than OF; median whole blood (plasma) maximum concentrations were 6.4 (10) and 41 (67) μg/L for 11-OH-THC and THCCOOH, respectively,[156] compared to < 0.5 μg/L and 115 ng/L, respectively, in OF.[114] Compared to OF, median detection windows of THC and THCCOOH in whole blood were longer in chronic smokers; 22 and 30 days[159] vs. 24 h and 13 days.[153] However, it should be noted that these detection windows were calculated with low LOQs. Perhaps the most important advantage of monitoring blood/plasma THC is its correlation with psychomotor performance[57-58], cognitive functions,[160] and subjective and physiological drug effects.[161] Further research on possible temporal relationships between cannabinoid OF concentrations and pharmacological effects would increase applicability of OF testing.
THC OF concentrations showed a strong linear relationship with serum concentrations in a controlled smoked cannabis administration study (r = 0.84; P < 0.001).[57] Correlations were lower in field OF and blood samples from the Roadside Testing Assessment (ROSITA)-2 project (r = 0.46),[162] psychiatric patients and suspected DUID drivers (r = 0.15),[163] and Norwegian suspected DUID drivers (r = 0.35).[164] As contamination of the oral cavity during cannabis intake, rather than transfer from blood, primarily determines THC OF concentrations, smoked dose and time since last smoking significantly contribute to the OF/blood concentration relationship. This, along with differences in collection and analytical methods, likely explains the wide variation in OF/blood THC concentration ratios among studies, ranging from 0.2-3.1 in 6 drivers suspected of DUID[165] and 0.5-2.2 (mean 1.2) within 0.3-4.0 h after controlled cannabis smoking (n = 6),[51] to later roadside studies which found mean (range; n) ratios of 8.2 (0.4-41.5; 11)[163] and 15.4 (0.01-568.9; 277).[162] After administration of a single smoked cannabis cigarette (low dose, 18.2 ± 2.8 mg; high dose 36.5 ± 5.6 mg THC), mean (SD) OF/serum THC ratios over 0-6 h were 46.2 (27.0) and 35.8 (20.3), respectively.[116] Median (range) OF/serum THC ratio over 0.5-8 h post single smoking (22.5-47.5 mg THC) was 16.5 (0.3-425) with no significant difference between occasional and chronic cannabis smokers.[147] Additionally, median (range) OF/plasma THC ratio of 0.3 (0.03-12.0) and THCCOOH ratio of 0.7 (0.05-8.7) ng/μg were reported during around-the-clock controlled oral THC administration (Figure 2).[166] All those studies observed a large inter-subject variability in cannabinoid concentrations, precluding direct prediction of blood concentrations from OF concentrations. Alternatively, Gjerde and Verstraete proposed quadratic and power regression models to determine equivalent THC cutoff concentrations in blood and OF so that detection window and prevalence of positive results could be better compared across matrices.[167] With 80 paired OF and blood concentrations, accuracy was 100±20% compared to actual prevalence in blood.[167] This approach might be useful when drug policy allows both OF and blood for establishing presence of drugs in the body or when results of case-control/drug prevalence studies using different matrices are compared.
OF and Urine Cannabinoids
Urine cannabinoid detection rates were generally lower than those in OF over the first 16 h after smoking a single cannabis cigarette.[148] At 1 h post smoking, all participants were THC-positive in OF, whereas only 22% were THCCOOH-positive in urine.[148] In samples from chronic pain clinics; however, urine THCCOOH was detected 54% more often than OF THC.[168] This is due to the primary analyte in urine being a metabolite (THCCOOH), with delayed Tmax and a longer detection window than the parent compound (THC). Urine THCCOOH detection window may range from several days in occasional smokers[169] to weeks in chronic smokers.[170-171] THC and 11-OH-THC in urine after a tandem β-glucuronidase/base hydrolysis were detected for 24 days in chronic smokers.[170] Mathematical models were developed to identify new cannabis intake with urine creatinine-normalized THCCOOH concentrations for occasional[169] and chronic cannabis users.[172] However, more than one specimen collection would be needed, which may not be practical for DUID investigations. Moreover, Toennes et al. reported that while detection rate exhibited good agreement between OF THC and serum THC (accuracy 90.8%), it was less accurate between urine THCCOOH and OF THC (66.4%) or serum THC (71.0%).[173] Thus, while urine testing is useful for long-term drug monitoring such as in workplace settings, OF testing would be preferable to identify recent drug intake in DUID settings.
Acute Cannabis Impairment
OF THC concentrations were significantly correlated with subjective intoxication (within-subject r = 0.71; P = 0.026; between-subject r = 0.05, P = NS) and heart rate elevation (r = 0.55; P > 0.1; r = 0.69, P = 0.013) over 4 h post smoking[152] and with performance on the Tower of London task (r = -0.35, P = 0.006), but not on the Critical Tracking task over 6 h after smoking.[57] Considering the significant influence of oral cavity contamination on THC OF concentrations, correlation between OF THC after smoking and impairment is due to comparable detection windows rather than a causal relationship. Even so, the temporal association could be useful in DUID and post-accident investigations, where determining recent drug exposure is an important factor. Impairment determined by police observations and medical examinations led to positive drug results in similar 72-76% of serum, OF, and urine samples, but there were more false positive urine results (37%) than for serum (18%) or OF (17%).[173] These findings support the value of OF as a matrix for DUID cannabinoid testing. Further research is needed to fully elucidate the relationship between OF cannabinoids and impairment and to determine accurate OF cutoff concentrations that reflect duration of impairment.
Long-Term Effects of Cannabis
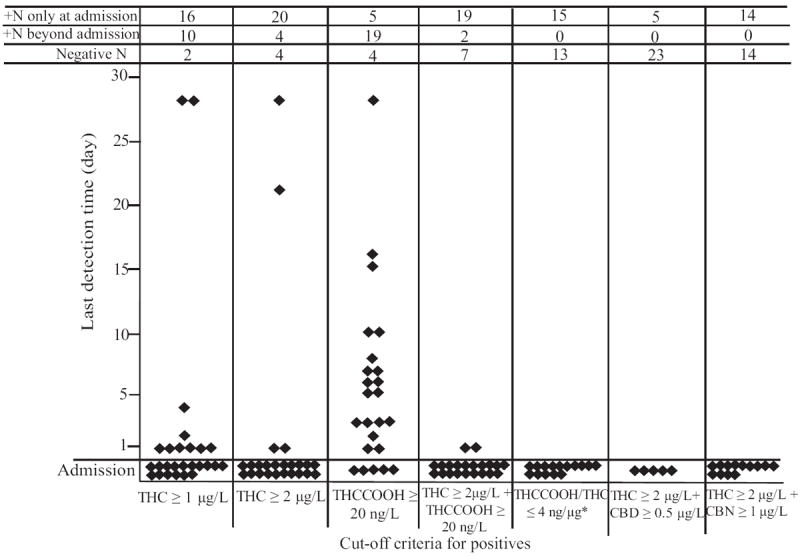
Lipophilic THC is initially absorbed into highly perfused organs such as the lungs, heart, brain, and liver.[99] THC’s Vd is approximately 3.4 L/kg, with 95-99% bound to plasma proteins, mainly lipoproteins.[174] With prolonged cannabis exposure, THC accumulates in adipose tissue, which slowly releases THC back into the circulation over time, leading to a long elimination half-life.[175-176] In chronic cannabis smokers during abstinence, low THC concentrations were detected in blood for up to 30 days,[159] and psychomotor performance in tasks validated to predict on-the-road impairment remained impaired compared to occasional smokers for 21 days.[177] In other studies, neurocognitive performance improved over 30 days in chronic frequent cannabis smokers, but was still impaired compared to occasional smokers for 7-28 days.[178-179] Hirvonen et al. reported significant brain CB1 receptor down-regulation (P < 0.05) in cortical brain regions known to be important to cannabis’ effects in chronic daily smokers that was reversed after 28 days of abstinence.[180] It is highly unlikely that OF THC concentrations play a role in long-term effects of cannabis. OF THC and THCCOOH were detected for up to 28 and 29 days in chronic daily cannabis smokers, most likely due to release of THC stored in fat.[153] Including THCCOOH, CBD, and CBN, as well as THC results may eliminate positive OF tests due to residual cannabinoid excretion in chronic frequent cannabis smokers (Figure 4).[153]
Figure 4.
OF Collection
For laboratory-based cannabinoid immunoassay screening or chromatographic confirmation, OF can be collected by passive drool, expectoration, or commercial collection devices. Each collection technique has advantages and limitations.
Passive Drool
Passive drool drug concentrations may be closest to concentrations excreted from salivary glands, because mechanical stimulation by expectoration or even insertion of a collection device into the mouth can increase salivary excretion to a small extent.[49] However, passive drool collection is unpleasant for donors and collectors.[49]
Expectoration
Expectoration offers drug concentration measurement in neat OF without buffer dilution, increasing assay sensitivity. The process is more cost-efficient than for collection devices; however, expectorated OF is viscous and contains mucus, food particles, and/or other mouth debris. Samples that are spun to remove precipitant material may yield lower concentrations due drug loss in the pellet, and drug adsorption to the tube during storage. In fortified expectorated OF samples centrifuged for 10 min, only 28.8% THC was recovered from supernatant; 51.7% was recovered from protein pellet and 14.7% from the polypropylene tube after addition of surfactant Triton® X-100.[181] Mucus in neat OF prevented good interaction with sorbent material during solid phase extraction, reducing drug concentrations and increasing imprecision.[150] Dry mouth following cannabis smoking also makes expectoration difficult and often yields low sample volumes.[131] Cannabinoids in expectorated OF showed poorer stability than those in OF collected with the Quantisal™ collection devices, likely due to lack of the stabilizing buffer, varied pH, and presence of enzymes that can bind or degrade analytes.[149] Stimulation of OF with paraffin, citric acid, chewing gum, and lozenges increased salivary flow rate, but also increased pH due to higher bicarbonate concentration, thereby lowering basic drug concentrations.[182-183]
OF Collection Devices
Commercial OF collection devices generally include a pad or sponge to absorb OF and a buffer to better stabilize drugs and extract them from the collection pad. Collection takes a few minutes, varying by device and amount of OF collected.[184] The absorbent pad also filters OF, reducing collection of extraneous materials. The buffer reduces OF viscosity and adsorption of lipophilic cannabinoids onto container surfaces.[150] These advantages make OF collection with a device preferable to expectoration. Amount of OF collected is determined by volume-adequacy indicators (Quantisal™, Saliva-Sampler™, Oral-Eze®), marking on the vial (Salicule™), dilution of a dye in the extraction solution (Greiner), or weighing the device before and after OF collection.
Variability in OF and buffer volumes between devices makes comparison among studies using different devices problematic due to varied dilution factors. Reporting concentrations in terms of neat OF rather than OF/buffer mixture is essential for comparing results. There can be additional variability in OF volume within a device; OF amount collected by the older OraSure Intercept® device ranged from 0.38-1.53 g.[185] Newer devices demonstrated narrower within-device variability of < 10% for Quantisal™ devices and < 5% for the Cozart® and Saliva-Sampler™ devices.[184] Another limitation with OF collection devices is adsorption of drugs onto the pad that may lead to false-negative results. THC loss in polypropylene tubes ranged from 22.8-29.3%.[181] The elution buffer reduces OF viscosity, but also dilutes analyte concentrations. Preservatives, stabilizing salts, and surfactants in buffer increased matrix effects in LC-MS methods, necessitating an extraction step prior to instrument analysis. Ion enhancement of 35% was observed for THCCOOH and suppression of 65% for THC.[186] Collecting OF from the left and right sides of the mouth showed no significant concentration difference for THC in Intercept® samples after smoking,[148] and for THC and THCCOOH in Quantisal™ samples during multiple 20 mg oral THC doses.[158] OF collection devices are described in Table 4.
Table 4.
Description of oral fluid collection devicesa
| Device (manufacturer) | Components | OF volume collected, mL | THC recovery, %b | Ref. |
|---|---|---|---|---|
| Certus (Concateno) | Pad, container, buffer (3mL), volume adequacy indicator | 1 | 37-44 (71-85) | [232] |
|
| ||||
| Cozart (Cozart Bioscience) | Pad, container, buffer (2mL), volume adequacy indicator | 1 | 75.9 (6.2) | [184, 233-234] |
| 94.5 (0.02) | ||||
| 67.4 | ||||
|
| ||||
| Greiner (Greiner Bio-One GmbH) | Rinsing solution (6mL), OF extraction solution (4mL), collection beaker, 2 OF vacuum transfer tubes | Determined spectro-photometrically w/dye in extraction solution | 73.6 (4.3) | [184] |
|
| ||||
| Intercept (OraSure Technologies) | Cotton fiber pad, plastic container, buffer (0.8mL) | 37.6 (9.0) | [184-185, 234] | |
| 37.8 (9.4) | ||||
| 39.2 | ||||
|
| ||||
| Quantisal (Immunalysis) | Cellulose pad, plastic container, buffer (3mL), volume adequacy indicator | 1 ± 0.1c | 55.8 (12.0) | [184, 232, 235] |
| 81.3-94.4 (4.8-12.1) | ||||
| 74-80 (12-16) | ||||
|
| ||||
| OraCol (Malvern Medical Developments) | Foam swab, centrifuge tube | 1 | < 12.5 | [184] |
|
| ||||
| OraTube (Varian) | Pad, plastic container, expresser | 47.5 (8.0) | [184] | |
|
| ||||
| Salicule (Acro Biotech) | Expectoration straw, container marked w/scale | 45.9 (10.9) | [184] | |
|
| ||||
| Saliva-Sampler (Statsure Diagnostic Systems) | Cellulose pad, plastic container, buffer (1 mL), volume adequacy indicator | 1 | 85.4 (7.0) | [184, 232] |
| 100-106 (5-6) | ||||
|
| ||||
| Salivette (Sarstedt AG & Co.) | Cotton swab, plastic container | < 12.5 | [184] | |
OF – oral fluid; THC – Δ9-tetrahydrocannabinol
This table covers only the devices reviewed between 2006-2013. OF collection devices are rapidly changed and new devices are continually developed. Device performance of different versions may differ.
values are mean (SD) unless otherwise specified
SD reported by the manufacturer
OF Cannabinoid Screening Techniques
Cannabinoid prevalence and concentrations vary across biological fluids and tissues; these differences must be taken into account when modifying cannabinoid screening assays for OF. Challenges include simultaneously extracting parent and metabolite cannabinoids that have different physicochemical characteristics, low OF volume, achieving ng/L limits of detection for metabolites, linear ranges encompassing the wide concentration ranges in parent compounds immediately after smoking and following oral THC, and validating carryover/dilution procedures to account for high THC concentrations found following smoked cannabis.[49]
Laboratory-Based OF Screening Methods
For laboratory-based screening, THC was identified in OF by thin layer chromatography and colorimetric development in early reports.[187-188] Enzyme immunoassay and radioimmunoassay methods to monitor OF THC first appeared in the 1970-80s.[187, 189] Schwope et al. comprehensively validated the Immunalysis Sweat/OF THC Direct ELISA method (THC cutoff = 4 μg/L), confirming OF cannabinoids by 2-dimensional GC-MS with a THC cutoff of 1 μg/L.[190] Diagnostic sensitivity, specificity, and efficiency were 85.5, 92.0, and 91.0%, respectively. When proficiency testing OF samples were screened by the OraSure micro-plate Intercept enzyme immunoassay kit (THC cutoff = 1 μg/L) and confirmed by GC/LC-MSMS, sensitivity and specificity were 73 and 100%, respectively.[191] Recent advances in analytical technology allow LC-MS to screen for THC along with multiple other drugs of abuse in OF.[192] Additionally, there is one immunoassay developed by Immunalysis (Ultra-sensitive Cannabinoids ELISA kit) intended for hair analysis that targets low THCCOOH concentrations with a cutoff of 20 ng/L neat OF.[128]
On-Site OF Screening Devices
The feasibility of utilizing OF for on-site screening was one of main advantages of OF compared to other matrices, particularly for DUID testing. OF on-site screening devices are continually evolving and frequently modified to improve performance, especially for cannabinoid detection; thus, evaluations summarized in Table 5 are limited to those reported since 2007. The ROSITA project supported by the European Commission (Directorate-General Transport) from 1999-2005 first evaluated device performance.[193] Initially, 3 on-site OF screening devices (DrugWipe®, ORALscreen™, and RapiScan™) were evaluated, comparing results with confirmatory blood concentrations and OF collected with the Intercept® device. The reference methods utilized GC-MS and, in some cases, HPLC-DAD or GC-ECD.[194] Although drivers and police preferred OF over urine or blood in most countries, no on-site OF screening device was sufficiently accurate for cannabinoid roadside drug testing.[194] Specificity of the ORALscreen™ and RapiScan™ ranged from 84-94%, but sensitivity was low (16-50%), producing a high rate of false negative results; no cannabis-positive results were obtained with DrugWipe®.[194]
Table 5.
Evaluation of on-site screening devices for Δ9-tetrahydrocannabinol in oral fluid.
| Device | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Name (manufacturer) | Year | THC Cutoff, μg/L | Resultb | OF Confirmation (cutoff, μg/L) | Typed | Sensitivity, % | Specificity, % | Efficiency, % | Ref. |
| BIOSENS (Biosensor) | 2011 | - | Instrumental | UPLC-MSMS | S | 50 | - | 51 | [198] |
| GC-MS (1) | |||||||||
|
| |||||||||
| Cozart DDS (Cozart) | 2011 | 31a | Instrumental | UPLC-MSMS | D, C | 22 | 100 | 71 | [198] |
| GC-MS (1) | |||||||||
| 2012 | GC-MS (1) | D | 37.8 | 100 | 94.3 | [199] | |||
| 2012 | UPLC-MSMS (10) | C | 28.2 | 100 | 78.7 | [236] | |||
|
| |||||||||
| Cozart DDSV (Cozart) | 2009 | - | Visual | GC-MS (0.5) | C | 41.2 | 100 | 60 | [237] |
|
| |||||||||
| Dräger DrugTest (Dräger) | 2007 | 20 | Instrumental | LC-MS (2) | D | 58.6 | 89.8 | 77.7 | [238] |
| 2010 | 25 | GC-MS (2)c | D | 72 | 50 | 68 | [239] | ||
| 2010 | 5 | GC-MS (2)c | D | 93 | 71 | 90 | [239] | ||
| 2011 | 25/5 | UPLC-MSMS | D, C, C | 59 | 96 | 82 | [198] | ||
| GC-MS (1) | |||||||||
| 2012 | 5 | 2D-GC-MS (2) | A | 90.7 | 75.0 | 87.9 | [200] | ||
| 2012 | 5 | GC-MS (1) | D | 92.3 | 96.7 | 96.7 | [199] | ||
| 2012 | 5 | UPLC-MSMS (10) | C | 80.8 | 95.5 | 92.0 | [236] | ||
|
| |||||||||
| DrugWipe (Securetec) | 2007 | 30 | Visual | HPLC/GC-MS | F | 80.0 | 100 | 82.9 | [240] |
| 2010 | GC-MS (2)c | D | 71 | 50 | 63 | [239] | |||
| 2011 | GC-MS (1) | D, C | 43 | 96 | 88 | [241] | |||
| 2012 | GC-MS (1) | D | 46.6 | 98.9 | 92.8 | [199] | |||
|
| |||||||||
| Impact (LifePoint) | 15 | Instrumental | HPLC/GC-MS | F | 100 | 33.3 | 71.4 | [240] | |
|
| |||||||||
| OraLab (Varian) | 2007 | 100 | Visual | HPLC/GC-MS | F | 40.0 | 100 | 76.0 | [240] |
| 2007 | LC-MS (2) | D | 93.3 | 98.6 | 98.1 | [238] | |||
| 2011 | 50 | UPLC-MSMS | D, C | 16 | 99 | 61 | [198] | ||
| GC-MS (1) | |||||||||
|
| |||||||||
| OrAlert (Innovacon) | 2011 | 100 | Visual | UPLC-MSMS | D, C | 11 | 100 | 78 | [198] |
| GC-MS (1) | |||||||||
| 2012 | UPLC-MSMS (10) | C | 23.1 | 100 | 90.9 | [236] | |||
|
| |||||||||
| OraLine IV (Sun Biomedical) | 2007 | 100 | Visual | HPLC/GC-MS | F | 100 | 36.0 | 54.3 | [240] |
|
| |||||||||
| OralStat (American Bio Medica) | 2007 | 25 | Visual | HPLC/GC-MS | F | 70.0 | 100 | 91.4 | [240] |
|
| |||||||||
| Oratect (Branan) | 2007 | 100 | Visual | HPLC/GC-MS | F | 0 | 100 | 77.8 | [240] |
| 2011 | 40 | UPLC-MSMS | C | 32 | 100 | 41 | [198] | ||
| GC-MS (1) | |||||||||
|
| |||||||||
| RapiScan (Cozart) | 2007 | 600 | Instrumental | HPLC/GC-MS | F | - | 100 | 100 | [240] |
|
| |||||||||
| RapidSTAT (Mavand) | 2010 | GC-MS (1.6) | D | 85.0 | 87.0 | 86.7 | [242] | ||
| 2011 | 15 | Visual | GC-MS (1) | D, C | 68 | 89 | 86 | [241] | |
| 2011 | UPLC-MSMS | D, C, S | 56 | 90 | 78 | [198] | |||
| GC-MS (1) | |||||||||
| 2012 | GC-MS (1) | D | 72 | 97 | 93 | [199] | |||
| 2012 | UPLC-MSMS (10) | C | 43.3 | 88.3 | 78.2 | [236] | |||
| 2012 | GC-MS (2)c | D | 71 | 55 | 66 | [239] | |||
|
| |||||||||
| SalivaScreen (Ulti-Med) | 2007 | > 100 | Visual | HPLC/GC-MS | F | - | 100 | 100 | [240] |
|
| |||||||||
| Uplink (OraSure) | 2007 | 25 | Instrumental | HPLC/GC-MS | F | 100 | 92.0 | 95.6 | [240] |
OF – oral fluid; THC – Δ9-tetrahydrocannabinol; 2D-GC – 2-dimensional GC; GC – gas chromatography; HPLC – high performance LC; LC – liquid chromatography; MS – mass spectrometry; UPLC – ultra performance LC
determined by the cutoff experiment using real patient samples
results interpreted visually or with an instrument
confirmation in plasma
A – controlled drug administration; C – clinical setting; D – driving under influence of drugs; F – fortified; S – Dutch coffee shops
The ROSITA-2 project (2003-2005) further evaluated nine on-site OF drug testing devices including DrugWipe® (Securetec Detektions-Systeme AG), Impact® (Lifepoint Inc.), OraLab® (Varian Inc.), OraLine® (Sun Biomedical Laboratories), OralStat® (American Bio Medica Corp.), Oratect™ II (Branan Medical Corp.), RapiScan™ (Cozart Bioscience Ltd.), SalivaScreen™ 5 (Ulti Med Products GmbH), and Dräger/OraSure DrugTest®/Uplink®. THC cutoffs ranged from 2 to 150 μg/L. More than 25% of devices failed due to low sample volume, high OF viscosity, or device malfunction; DrugWipe®, OralStat®, RapiScan™, and Dräger® had failure rates of < 5-10%.[195] On-site testing for cannabis exhibited sensitivity ranging from 0 to 74% and specificity between 70-100%, with OF collected with the Intercept® and analyzed by GC/LC-MS methods for confirmation.[195] DrugWipe® produced negative results when up to 205 μg/L THC was confirmed by GC-MS analysis of Intercept® collected OF samples.[196] Low sensitivity could be attributed to low cross-reactivity with THC when on-site immunoassays were modified from assays designed to identify urine THCCOOH. Additional possibilities included high limits of detection, adsorption to the device, and/or poor drug recovery from the collection pad.[196-197] The ROSITA project proposed criteria for sensitivity and specificity of > 90%, efficiency of > 95%, and device failure rate of 5-10% for acceptable on-site OF screening devices,[195] but no device met these criteria in 2005.
In 2006, a new EU project, Driving under the Influence of Drugs, Alcohol and Medicine (DRUID), was initiated to continue evaluation of on-site OF screening devices. DRUID recommended sensitivity, specificity, and efficiency ≥80%. Eight devices were evaluated with OF samples obtained from drivers suspected of DUI, patients at drug treatment facilities, and patrons at Dutch coffee shops, including BIOSENS® Dynamic (Biosensor Applications Sweden AB), Cozart® DDS 806 (Cozart Bioscience Ltd.), DrugWipe® 5+ (Securetec Detektions-Systeme AG), Dräger DrugTest® 5000 (Dräger Safety AC&CO.) OraLab® 6 (Varian Inc.), OrAlert™ (Innovacon Inc.), Oratect® III (Branan Medical Corp.), and RapidSTAT® (Mavand Solutions GmbH).[198] Compared with ROSITA results, specificity remained acceptable (90-100%) for all devices, but sensitivity was still low (11-59%), which reduced efficiency (41-88%).[198] A large difference in cutoff concentrations between the confirmatory LC-MSMS/GC-MS methods (THC 1 μg/L) and on-site screening devices (average 39 μg/L; range 5-100 μg/L) decreased sensitivity.[198] Although high after smoking cannabis, OF THC concentrations rapidly decrease within a few hours after smoking, creating the potential for false negative results if a cutoff is too high.[114, 116] When OF samples were obtained near Dutch coffee shops where individuals likely smoked cannabis recently, sensitivity of the DrugTest® 5000 for cannabis was much higher (76%), even with the older version of the device, compared to results from OF samples collected at the roadside (53%).[198]
In the ROSITA and DRUID projects, device-specific limitations were documented by operators: long collection time (Oratect® III, OraLine®), insufficient sample volume (Impact®, SalivaScreen™, OraLab®), frequent device failure (OraLab®, Oratect®), difficulty in transferring OF to the test device (ORALscreen™), reading results (ORALscreen™, DrugWipe®, OralStat®, OraLine®, OraLab®) and transporting the device (RapiScan™), poor performance in cold/rainy weather (DrugWipe®, OraLine®), and complex sample-preparation procedure (RapiScan™, Dräger DrugTest®/OraSure Uplink®).[194-195, 198] Thus, high sensitivity for detecting cannabis intake, a short and simple collection procedure, easily distinguishable outcome, and convenient device transportation are important considerations when developing on-site OF screening devices. Among currently available on-site drug testing devices, the new version of the Dräger DrugTest® 5000 performed well following controlled cannabis smoking as compared to 2D-GC-MS confirmation with the Quantisal™ OF collection device.[199] Diagnostic sensitivity, specificity, and efficiency at DrugTest® 5000’s 5 μg/L screening cutoff and 0.5-2 μg/L THC confirmatory cutoffs were 86.2-90.7, 75.0-77.8, and 84.8-87.9%, respectively; however, owing to few true negative samples, specificity was inadequately evaluated.[200] Ease of use and automated result reading were additional advantages of this device.[199]
Confirmatory Methods
Early chromatographic assays published in the 1970-80s employed GC-ECD,[201] GC-MS,[202] HPLC-MS,[203] and HPLC-ED[204] to detect THC at limits of detection (LOD) of 1-2 μg/L. As analytical technologies improved, OF methods to identify THC simultaneously with other drugs of abuse and/or multiple cannabinoids were developed. A method using HPLC-UV detector coupled with immunoaffinity chromatography for sample clean-up detected THC, CBD, and CBN at LODs of 2, 1, and 0.8 μg/L, respectively.[205] A more sensitive assay with solid-phase microextraction (SPME) and quadrupole ion trap GC-MS identified THC, Δ8-THC, CBD, and CBN with a 1 μg/L LOD.[206] In the 2000s, methods for OF THC and 4-9 other common drugs of abuse with (LOD = 20 μg/L)[207] or without (LOQ = 5 μg/L)[208] CBD and CBN were published, utilizing SPME and GC-MS.
More recent OF methods had lower LOQs for cannabinoids and/or include more drugs of abuse. Moore et al. reported a GC-MS method to quantify THCAA, THC, CBD, and CBN with LOQs of 0.5-1 μg/L.[154] Choi et al.[209] employed GC-MS with automated SPE to quantify OF THC and THCCOOH (LOQs = 2 μg/L), whereas Sergi et al.[210] utilized LC-MSMS after sample filtration for OF THC and THCCOOH analysis (LOQs = 3.7 and 3.5 μg/L) along with 11 other drugs. Another validated method with HPLC and quadrupole-time-of-flight MS analyzed OF THC and THCCOOH at LOQs of 0.1 and 0.5 μg/L, respectively.[211] SPE coupled with LC-MSMS,[212] UPLC-MSMS,[213] and GC-MS[214] were utilized to quantify 22, 29, and 30 drugs of abuse including THC at LOQs of 1, 0.5, and 2 μg/L, respectively, in OF. The need to minimize positive results from passive environmental exposure precipitated development of analytical methods sufficiently sensitive to monitor OF THCCOOH. Day et al.[126] developed a GC-MSMS method, while Moore et al.[155] used 2-dimensional GC-MS to quantify OF THCCOOH at LOQs of 10 and 2 ng/L, respectively. Another 2-dimensional GC-MS assay was the first to quantify OF THCCOOH (LOQ = 7.5 ng/L) as well as THC, CBD, CBN, and 11-OH-THC (LOQs = 0.5-1 μg/L).[215] In the past year, LC-MSMS,[186, 216] microflow LC-MSMS,[217-218] and isotope dilution LC-MSMS[219] methods to analyze OF for THCCOOH (LOQs = 7.5-15 ng/L) and THC (0.25-1 μg/L) were published. Chromatographic OF confirmation assays for cannabinoids published since 2003 are described in Table 6.
Table 6.
Chromatographic methods for quantifying cannabinoids in oral fluid.
| OF Sample | Analyte | Sample preparation | Method | LLOQ, μg/L | # of Other drugs | Ref. | ||
|---|---|---|---|---|---|---|---|---|
| Collection | Volume, μLa | Separation | Detection | |||||
| RapiScan | 200 | THC; CBD; CBN | Direct immersion/Head space SPME | GC | MS (EI) | 20/50b | 9 | [207] |
| Salivette | 1000 | THC | Acidification, SPME | GC | MS (EI) | 5 | 4 | [208] |
| Expectoration | 200 OF | THC | LLE | LC | MS (ESI) | 2 | - | [243] |
| Expectoration | 250 OF | THC | SPE, derivatization | GC | MS (EI) | 2 | 29 | [214] |
| Expectoration, Salivette | 500 OF | THC | SPE | HPLC | MS (ESI) | 2 | - | [151] |
| Intercept | 100/500 | THC | LLE | LC | MSMS (ESI) | 0.5/0.1 | - | [244] |
| Intercept | 100 OF | THCCOOH | Hydrolysis, SPE, derivatization | GC | MSMS (NCI) | 10 | - | [126] |
| Quantisal | 1000 | THCCOOH | SPE, derivatization | 2D-GC | MS (NCI) | 0.002 | - | [155] |
| Quantisal | 1000 | THC; THCAA; CBD; CBN | SPE, derivatization | GC | MS (EI) | 0.5; 1; 1; 0.5 | - | [154] |
| Quantisal | 1000 | THC | SPE, derivatization | GC | MS (EI) | 0.5 | - | [128] |
| 500 OF | THC; THCCOOH | LLE | HPLC | TOF MSMS (HESI) | 0.1; 0.5 | - | [211] | |
| Intercept | 500 | THC | LLE | HPLC | MSMS (ESI) | < 0.16b | 31 | [192] |
| Salivette | 1000 | THC; CBD; CBN; 11-OH-THC; THCCOH | SPE, derivatization | GC | MS (EI) | 1.9; 0.9; 5.6; 12.7; 4.8 | 25 | [245] |
| Expectoration | 500 OF | THC | SPE | LC | MS (ESI) | 5 | - | [246] |
| Saliva-Sampler | 1000 | THC | SPE | LC | MSMS (ESI) | 1 | 22 | [212] |
| Saliva-Sampler | 200 mg OF + buffer | THC | SPE | UPLC | MSMS (ESI) | 0.5 | 28 | [213] |
| Expectoration | 250 OF | THC; THCCOOH | SPE | GC | MS (EI) | 2; 2 | - | [209] |
| Expectoration | 150 OF | THC; THCCOOH | Centrifugation, filtration | HPLC | MSMS (ESI) | 5; 4.3 | 11 | [210] |
| Quantisal | 1000 | THC; CBD; CBN; 11-OH-THC; THCCOOH | SPE; derivatization | 2D-GC | MS (EI, NCI) | 0.5; 0.5; 1; 0.5; 0.0075 | - | [215] |
| Quantisal | 1000 | THC; THCCOOH | Hydrolysis, SPE, derivatization | LC | MSMS (ESI) | 1; 0.01 | - | [186] |
| Oral-Eze | 400 | THC; THCCOOH | Centrifugation, filtration | Microflow LC | MSMS (HESI) | ND; 0.0075 | - | [217] |
| Expectoration | 250 OF | THC; THCCOOH | Derivatization, LLE | Isotope dilution HPLC | MSMS (ESI) | 0.025; 0.01 | - | [219] |
| Expectorationd | 250 OF | THC; CBD; CBN; 11-OH-THC; THCCOOH | Derivatization, LLE/SPE | LC | MSMS (ESI) | 0.05/0.025; 0.05/0.3; 0.1/0.005; 0.1/0.005; 0.1/0.005b | - | [247] |
| RapiScan | 200 OF + buffer | THC | LLE | LC | MSMS (ESI) | 1 | - | [221] |
| Quantisal | 500 | THC; CBN | LLE | LC | MSMS (ESI) | 1.04; 1.3 | 30 | [229] |
| Certus, Quantisal, Saliva-Sampler | 50 OF + buffer | THC (CBD; CBN)c | LLE | UPLC | MSMS (ESI) | 5 | - | [232] |
| Intercept | 400 | THC; THCCOOH | SPE | LC | MSMS (HESI) | 0.2; 0.2 | - | [248] |
| Quantisal; Oral-Eze | 1000; 750 | THC; CBD; CBN; THCCOOH | SPE | Microflow LC | MSMS (HESI) | 0.5; 0.5; 0.5; 0.015 | - | [218] |
| Quantisal | 1000 | THCCOOH | SPE | HPLC | MSMS (ESI) | 0.012 | - | [216] |
CBD – cannabidiol; CBN – cannabinol; 2D-GC – 2-dimensional GC; EI – electron impact ionization; ESI – electronspray ionization; GC – gas chromatography; HESI – heated ESI; HPLC – high performance LC; LC – liquid chromatography; LLE – liquid-liquid extraction; LLOQ – low limit of quantification; MS – mass spectrometry; NCI – negative chemical ionization; ND – not determined; OF – oral fluid; 11-OH-THC – 11-hydroxy-THC; SPE – solid phase extraction; THC – Δ9-tetrahydrocannabinol; THCAA – Δ9-tetrahydrocannabinolic acid A; THCCOOH – 11-nor-9-carboxy-THC; UPLC – ultra performance LC
Oral fluid mixed with buffer, unless otherwise specified
for qualitative identification only (limit of detection)
CBD and CBN were chromatographically identified but not included in validation
validation data not reported
OF Cannabinoid Stability
Drug stability during storage is an important consideration for accurate understanding of drug and metabolites’ pharmacokinetic profile. It is especially important in interpretation of drug concentrations for forensic and clinical purposes due to the significant impact of test results. Cannabinoid OF stability depends on collection methods, buffer composition in commercial collection devices, analytes, storage containers, temperature and storage duration. Furthermore, stability in fortified synthetic or authentic OF could differ from stability in authentic OF samples collected after controlled cannabis administration. In fortified OF collected with the Quantisal™ device, < 20% THC loss occurred after storage at 2-8°C for 14 days; the loss increased to over 50% with fluorescent light exposure or storing with serum separators.[220] THC, CBD, CBN, and THCAA were stable in fortified synthetic OF collected with the Quantisal™ device for 10 days at 4°C; cannabinoids other than CBN decreased approximately 50% at room temperature over the same period.[154] With the Intercept® OF collection device, 13, 45, and 39% THC losses in fortified OF were reported after 2 weeks at -20, 4, and 21°C, respectively; after 6 weeks, there were 21, 87, and 86% THC losses.[108]
Langel et al. evaluated cannabinoid stability in fortified OF collected with 9 different collection devices (Cozart®, Greiner Bio-One, Intercept®, OraCol, OralTube™, Quantisal™, Salicule™, Saliva-Sampler™, and Salivette®), as well as in polypropylene tubes; cannabinoid stability was assessed after 0, 14, and 28 days of storage at -18°C for all devices except Greiner, which was stored at 4°C.[184] THC loss was < 20% with Cozart®, Intercept®, Quantisal™, and polypropylene tubes for 28 days. With Saliva-Sampler™, THC was 95.2% of baseline on Day 14 and declined to 78.8% on Day 28; with OraTube™, THC was 77.8% on Day 14 increasing to 84.6% on Day 28. Greater than 50% THC loss occurred with Greiner and Salicule™, and THC was not detected with OraCol and Salivette® on Day 14.[184] When THC and THCCOOH stability was evaluated in fortified, expectorated OF diluted in 0.1 M phosphate buffer over 6 days, analyte losses were < 10% when stored in glass tubes but > 20% in polypropylene tubes at both room temperature and 4°C. THC degradation was more significant than THCCOOH (up to 86% after 6 days) and the larger polypropylene tubes (diameter 1 vs. 5 cm) led to poorer stability.[209] THC loss (22.8-29.3%) from adsorption to polypropylene tubes was similarly observed by Molnar et al.; this loss was minimized by addition of surfactant Triton® X-100 with > 96% THC recovery.[181] Moreover, fortified OF samples in phosphate buffer with and without preservative sodium azide showed a similar THC loss of approximately 25% at 4°C and 50% at room temperature after 4 weeks, suggesting that oxidative degradation may contribute more to OF THC instability than microbial action.[181] The Cozart® fortified OF samples had minimal loss even at room temperature over 4 weeks.[181] The researchers previously reported that when authentic OF samples (N = 48) collected with Cozart® devices were re-analyzed after 13-18 months and 4°C storage, an average THC recovery of 89% was observed[221]; > 50% THC loss in fortified, expectorated OF at room temperature in 1 day; at both 4 and -18°C, THC concentrations decreased to 70-85% and 65% after 1 and 14 days, respectively.[221] In OF proficiency samples (exact composition of samples unknown), THCCOOH was stable for 3 months at 4°C, but showed approximately 50 and 100% loss after 6 and 12 months, respectively.[186] These fortified OF stability data indicated that 1) THC in OF collected with certain devices (e.g., Cozart®, Intercept®, Quantisal™, Saliva-Sampler™) were stable at freezing temperature for 2-4 weeks and preferred over expectoration and other collection devices; 2) storage at room temperature should be avoided; 3) short-term storage at refrigerated temperature was stable in Quantisal™ but not Intercept® collected OF; and 4) addition of surfactant is important for THC recovery from collection tubes.
In authentic Quantisal™ OF samples after controlled cannabis smoking (n = 10), cannabinoid concentrations were stable (< 20% change from baseline) for 1 week at 4°C; after 4 wks at 4°C, as well as 4 and 24 wks at -20°C, THC was stable in 90, 80, and 80% and THCCOOH in 89, 40, and 50% of Quantisal™ samples, respectively. CBD showed stability similar to THCCOOH, but CBN, unlike other analytes, increased over time, likely due to the fact that CBN is a THC degradation product. Cannabinoids in concurrently collected expectorated OF were less stable than in Quantisal™ samples when refrigerated or frozen, and exhibited instability even after 7 days. Large inter-subject variability in stability results also was observed.[149] Overall, these findings highlight the importance of stabilizing/elution buffer to maintain cannabinoid integrity during storage. Expectorated OF samples showed similar cannabinoid stability at 4 or -20°C, but should be analyzed as soon as possible. Storage at 4°C and analysis within 4 weeks are recommended for Quantisal™ OF samples. Optimal storage conditions could be different with other collection methods.
Adulteration
Because OF collection is directly observable, sample adulteration is much less likely than for urine, but exogenous interference experiments with common medicines and drugs of abuse are important components in analytical method validation.[154, 186, 215] Two commercial OF adulterants, “Clear Choice® Fizzy Flush™” and “Test’in™ Spit n Kleen Mouthwash,” did not significantly affect fortified OF THC concentrations analyzed by GC-MS.[222] For screening assays, common foods, beverages, food ingredients, cosmetics, and personal hygiene products produced no false positives with the on-site Oratect® drug screening device.[222] Listerine® mouthwash, orange juice, toothpaste, coffee, and soy milk also did not interfere with performance of the Immunalysis Sweat/OF THC Direct ELISA.[190]
Passive Cannabis Smoke Exposure
False positive results from passive environmental cannabis smoke are a major concern in OF drug testing because parent cannabinoids in drug-laden smoke deposit on the oral mucosa. Gross et al. conducted a passive inhalation experiment in a closed room (3 × 3 m) in which smokers and non-smokers (n = 8) sat alternatively in a circle. After each smoker smoked 1 cannabis cigarette (27 mg THC), OF samples from non-smokers contained a mean of 18 μg/L THC at 15 min, which was negative by 30 min.[189] Niedbala et al. initially conducted a passive exposure study in a closed room (3 × 4 × 3 m) in which a single cannabis cigarette was provided to each of 5 cannabis smokers; 4 non-smokers sat approximately 1.5 m from smokers.[223] OF was collected from non-smokers for 4 h. Mean OF THC concentration in non-smokers was 13.4 μg/L immediately after smoking, which decreased to 0.3 μg/L and < LOQ 45 and 75 min post smoking, respectively. Because collection was performed inside the room, THC concentrations in room air (up to 0.19 μg/L detected in air samples) could have contaminated OF collection devices.[223]
In the authors’ second study, passive smoke exposure conditions were created in an unventilated 8-passenger van.[224] Four non-smokers sat beside 4 smokers who each smoked a cannabis cigarette containing 39.5 mg THC (Session 1) or 83.2 mg THC (Session 2). In Session 1, where OF collection occurred inside the van for 1 h post smoking and subsequently outside the van for up to 72 h, mean THC concentration was 5.3 μg/L immediately after smoking in non-smokers; no one was positive by 6 h. When collected outside of the van (Session 2), THC concentrations were ≤1.1 μg/L in non-smokers right after smoking; all became negative by 2 h. When OF collection devices were exposed to the air during smoking, THC concentrations as high as 14 μg/L were detected within 45 min.[224] More recently, Moore et al. performed a passive exposure study in which 10 non-smokers were in one of 2 Dutch coffee-shops for 3 h; OF collection occurred outside the shops.[127] At Location 1, 4-16 smokers were present in the 5 × 7 × 3.5 m smoking area. All 5 non-smokers were THC-positive, with concentrations ranging from 0.5 to 6.8 μg/L over 0.3-3 h of exposure; 2 were positive (1.0-1.1 μg/L) after 12-22 h post-exposure. Three non-smokers were CBN-positive (0.5-1.7 μg/L) as well after 2-3 h of exposure. At Location 2, 0-6 smokers were present in the 2 × 7 × 3 m smoking area. Non-smokers were not THC-positive until 1 h of exposure, but by 3 h all were positive (1.3-17 μg/L). Three non-smokers also were CBN-positive by 3 h (1.1-2.0 μg/L). CBD and THCCOOH were not detected in any non-smokers at LOQs of 1 μg/L and 2 ng/L, respectively. Collection pads exposed to the air had high THC (212-290 μg/L), CBD (16-38 μg/L), and CBN (40-48 μg/L) concentrations, but no THCCOOH.[127] Therefore, OF collection should always take place outside the cannabinoid smoke exposure area to avoid environmental contamination of collection devices with parent cannabinoids.
These results further confirm that OF THCCOOH was not present in cannabis smoke and OF was THCCOOH-negative following passive exposure. 11-OH-THC also could be a valuable analyte for identifying active cannabis intake if it is not formed in oral tissue from THC deposits. CYP2C9, the primary cytochrome P450 enzyme converting THC to 11-OH-THC was found in gingival tissue along with CYP1A1, 1A2, 2E1, and 3A4.[98] Whether THC that accumulates in oral tissue after active or passive exposure is metabolized to 11-OH-THC to an extent detectable in OF needs to be investigated. Additional research is required to systemically evaluate environmental OF cannabinoid contamination. Contamination may vary according to the potency of cannabis cigarettes, proximity to the smoker, and duration of exposure. Evaluation of OF cannabinoid concentrations in non-smoking family members in households where medical marijuana smoking occurs on a regular basis also is needed.
Concluding Remarks
Prevalence of OF drug testing grew greatly in recent years. Research on its validity and reliability is accordingly proliferating. A simple and observable collection procedure and short detection window to identify recent drug exposure make OF testing increasingly popular in DUID, workplace, and clinical drug testing programs. Current knowledge of OF cannabinoids presented in this review demonstrates many factors (pharmacokinetic properties, collection procedure, analytical method, drug stability, and passive environmental exposure) to consider when interpreting OF cannabinoid results. Different cannabinoids have distinct elimination profiles and detection windows, which are influenced by routes of administration, dose, and drug use history. Thus, each drug testing program should establish cutoff criteria, collection/analysis procedures, and storage conditions appropriate for its purposes. For instance, because the goals of workplace drug testing are pre-employment screening and drug use deterrence over the course of employment, cutoff criteria that allow long detection windows would be beneficial. In contrast, it is important for DUID and post-accident investigations to identify recent drug intake reflecting impairment. For this purpose, our laboratory suggested several OF cutoff criteria to eliminate misinterpretation of residual THC excretion, utilizing multiple cannabinoids.[114-115, 131, 153] Increasing cutoff concentrations can also shorten detection windows. Issues of drug stability and passive environmental exposure are particularly important for forensic testing, where test results can have substantial legal or financial consequences. Similarly, the shorter detection window with OF testing may be advantageous in anti-doping, as WADA prohibits cannabinoids in-competition only; urine THCCOOH ≥15 μg/L defines an adverse analytical finding.[84] In clinical settings, the absence of OF THC, CBD, and CBN can be monitored to identify relapse to cannabis smoking during oral THC pharmacotherapy for cannabis dependence. Alternatively, to monitor compliance with oral THC treatment, THCCOOH would be a better OF analyte than parent cannabinoids. High OF CBD/THC ratios distinguish Sativex intake from cannabis smoking, and thus, could document compliance with Sativex pharmacotherapy. However, within the last 2 years, interest in cannabis plants with high CBD content (> 4%) has grown; smoking CBD-rich strains (e.g., Harlequin, Jamaican Lion, etc.)[225] also could lead to high OF CBD/THC ratios.
Building a scientific basis for OF testing is an on-going process. OF is a relatively new biological matrix for cannabinoid testing, with some aspects of OF cannabinoid testing yet to be evaluated, e.g., the elimination profile of 11-OH-THC at ng/L OF. There could be other OF cannabinoid markers (cannabigerol, tetrahydrocannabivarin, THC-glucuronide, etc.) that may identify recent drug intake and/or minimize the possibility of passive environmental contamination. Biomarkers to normalize OF volume are yet to be accepted due to a lack of scientific data supporting their use. Relationships between cannabinoid OF concentrations and pharmacological effects (e.g., impairment, tolerance, and withdrawal) have not been fully evaluated. Our laboratory recently completed pharmacokinetic and stability analyses on cannabinoids in expectorated OF and OF collected with the Quantisal device, and currently are evaluating these parameters for OF collected with Oral-Eze® and Saliva-Sampler™ devices. Such assessments are needed for each collection device. Our upcoming data comparing OF cannabinoid disposition between occasional and chronic cannabis smokers will further improve interpretation of OF test results and establishing cutoff criteria. Most clinical studies evaluating OF cannabinoids employed single-dose cannabis administration. As many cannabis smokers consume cannabis multiple times a day,[153, 158] it is important to assess OF cannabinoid elimination patterns after multiple smoking episodes. Lastly, at least within different drug testing disciplines (e.g., workplace, DUID, sports, clinical practice), the effort to standardize OF collection, storage, and analysis procedures and to institute quality control systems should continue. The standardization of OF testing could be facilitated by involvement of regulatory agencies like EWDTS, SAMHSA, and DRUID, accrediting bodies like the American Society of Crime Laboratory Directors/Laboratory Accreditation Board, and scientific guidelines committees such as the Scientific Working Group for Forensic Toxicology (SWGTOX).
OF clearly offers many advantages as an alternative matrix for monitoring cannabis use. The reliability of test results depends on the reliability of the overall testing process from collection, transportation/storage, analysis, to data interpretation. We present valuable information for establishing appropriate OF testing procedures. This scientific foundation is essential for incorporating OF testing into drug monitoring for DUID, criminal justice, sports, and workplace settings and the development/management of cannabinoid pharmacotherapy. Continuing research on OF cannabinoids, particularly in relation to passive environmental exposure, drug use history, donor physiological conditions, and metabolism in the oral cavity is needed to better understand mechanisms of cannabinoid OF disposition and expand applicability of OF drug testing.
References
- 1.Pertwee RG. Br J Pharmacol. 2006;147(Suppl 1):S163. doi: 10.1038/sj.bjp.0706406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bostwick JM. Mayo Clin Proc. 2012;87:172. doi: 10.1016/j.mayocp.2011.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.United Naitons Office on Drugs and Crime. World Drug Report 2012 United Nations Publication. Vienna, Austria: 2012. Sales No E.12.XI.1. [Google Scholar]
- 4.van den Brink W. Curr Opin Psychiatry. 2008;21:122. doi: 10.1097/YCO.0b013e3282f57e04. [DOI] [PubMed] [Google Scholar]
- 5.Johnson MB, Kelley-Baker T, Voas RB, Lacey JH. Drug Alcohol Depend. 2012;123:105. doi: 10.1016/j.drugalcdep.2011.10.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.ter Bogt T, Schmid H, Gabhainn SN, Fotiou A, Vollebergh W. Addiction. 2006;101:241. doi: 10.1111/j.1360-0443.2006.01309.x. [DOI] [PubMed] [Google Scholar]
- 7.O’Connell TJ, Bou-Matar CB. Harm Reduct J. 2007;4:1. doi: 10.1186/1477-7517-4-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Substance Abuse and Mental Health Services Administration. Results from the 2011 National Survey on Drug Use and Health. Rockville, MD: 2012. Summary of National Findings NSDUH Series H-44, HHS Publication No. (SMA) 12-4713. [Google Scholar]
- 9.Lacey JH, Kelley-Baker T, Furr-Holden B, Voas RB, Romano E, Ramirez A, et al. 2007 National Roadside Survey of Alcohol and Drug Use by Drivers: Drug Results National Highway Traffic Safety Administration DOT HS 811 249 [Google Scholar]
- 10.Van der Linden T, Legrand SA, Silverans P, Verstraete AG. J Anal Toxicol. 2012;36:418. doi: 10.1093/jat/bks038. [DOI] [PubMed] [Google Scholar]
- 11.Chu M, Gerostamoulos D, Beyer J, Rodda L, Boorman M, O H D. Forensic Sci Int. 2012;215:28. doi: 10.1016/j.forsciint.2011.05.012. [DOI] [PubMed] [Google Scholar]
- 12.Houwing S, Hagenzieker M, Mathijssen R, Bernhoft IM, Hels T, Janstrup K, van der Linden T, Legrand SA, Verstraete A. Prevalence of alcohol and other psychoactive substances in drivers in general traffic Part I: general results DRUID Deliverable 2.2.3. 2011 www.druid-project.eu.
- 13.Kelly E, Darke S, Ross J. Drug Alcohol Rev. 2004;23:319. doi: 10.1080/09595230412331289482. [DOI] [PubMed] [Google Scholar]
- 14.Walsh JM, Flegel R, Cangianelli LA, Atkins R, Soderstrom CA, Kerns TJ. Traffic Inj Prev. 2004;5:254. doi: 10.1080/15389580490465319. [DOI] [PubMed] [Google Scholar]
- 15.Drummer OH, Kourtis I, Beyer J, Tayler P, Boorman M, Gerostamoulos D. Forensic Sci Int. 2012;215:14. doi: 10.1016/j.forsciint.2011.01.040. [DOI] [PubMed] [Google Scholar]
- 16.Cone EJ, Caplan YH, Black DL, Robert T, Moser F. J Anal Toxicol. 2008;32:530. doi: 10.1093/jat/32.8.530. [DOI] [PubMed] [Google Scholar]
- 17.Pesce A, West C, Rosenthal M, Mikel C, West R, Crews B, Almazan P, Latyshev S, Horn PS. Pain Physician. 2011;14:189. [PubMed] [Google Scholar]
- 18.Mordal J, Holm B, Mørland J, Bramness JG. J Clin Psychopharmacol. 2010;30:455. doi: 10.1097/JCP.0b013e3181e61923. [DOI] [PubMed] [Google Scholar]
- 19.de Beaurepaire R, Lukasiewicz M, Beauverie P, Castéra S, Dagorne O, Espaze R, Falissard B, Giroult P, Houery M, Mahuzier G, Matheron I, Niel P, Padovani P, Poisson N, Richier JP, Rocher J, Ruetsh O, Touzeau D, Visinoni A, Molimard R. Eur Psychiatry. 2007;22:540. doi: 10.1016/j.eurpsy.2007.05.001. [DOI] [PubMed] [Google Scholar]
- 20.Vitale S, van de Mheen D. Drug Alcohol Depend. 2006;82:1. doi: 10.1016/j.drugalcdep.2005.08.017. [DOI] [PubMed] [Google Scholar]
- 21.Strano Rossi S, Botrè F. J Sports Sci. 2011;29:471. doi: 10.1080/02640414.2010.543915. [DOI] [PubMed] [Google Scholar]
- 22.Silva OA, Yonamine M. Rev Saude Publica. 2004;38:552. doi: 10.1590/s0034-89102004000400011. [DOI] [PubMed] [Google Scholar]
- 23.George S. Occup Med (Lond) 2005;55:69. doi: 10.1093/occmed/kqi017. [DOI] [PubMed] [Google Scholar]
- 24.Li G, Baker SP, Zhao Q, Brady JE, Lang BH, Rebok GW, DiMaggio C. Addiction. 2011;106:1287. doi: 10.1111/j.1360-0443.2011.03388.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cone EJ, Presley L, Lehrer M, Seiter W, Smith M, Kardos KW, Fritch D, Salamone S, Niedbala RS. J Anal Toxicol. 2002;26:541. doi: 10.1093/jat/26.8.541. [DOI] [PubMed] [Google Scholar]
- 26.United Nations Office on Drugs and Crime. World Drug Report 2010 United Nations Publications. Vienna, Austria: 2010. Sales No. E.10.XI.13. [Google Scholar]
- 27.Substance Abuse and Mental Health Services Administration. Treatment Episode Data Set (TED) 2000-2010; National Admissions to Substance Abuse Treatment Services DASIS Series S-61. Rockville, MD: 2012. HHS Publication No. (SMA) 12-4701. [Google Scholar]
- 28.Mehmedic Z, Chandra S, Slade D, Denham H, Foster S, Patel AS, Ross SA, Khan IA, ElSohly MA. J Forensic Sci. 2010;55:1209. doi: 10.1111/j.1556-4029.2010.01441.x. [DOI] [PubMed] [Google Scholar]
- 29.Howlett AC, Bidaut-Russell M, Devane WA, Melvin LS, Johnson MR, Herkenham M. Trends Neurosci. 1990;13:420. doi: 10.1016/0166-2236(90)90124-s. [DOI] [PubMed] [Google Scholar]
- 30.Herkenham M, Lynn AB, Little MD, Johnson MR, Melvin LS, de Costa BR, Rice KC. Proc Natl Acad Sci U S A. 1990;87:1932. doi: 10.1073/pnas.87.5.1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lutz B. Prostaglandins Leukot Essent Fatty Acids. 2002;66:123. doi: 10.1054/plef.2001.0342. [DOI] [PubMed] [Google Scholar]
- 32.Elphick MR, Egertová M. Philos Trans R Soc Lond B Biol Sci. 2001;356:381. doi: 10.1098/rstb.2000.0787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Basu S, Dittel BN. Immunol Res. 2011;51:26. doi: 10.1007/s12026-011-8210-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Idris AI, Sophocleous A, Landao-Bassonga E, van’t Hof RJ, Ralston SH. Endocrinology. 2008;149:5619. doi: 10.1210/en.2008-0150. [DOI] [PubMed] [Google Scholar]
- 35.Gardner EL, Lowinson JH. Pharmacol Biochem Behav. 1991;40:571. doi: 10.1016/0091-3057(91)90365-9. [DOI] [PubMed] [Google Scholar]
- 36.Huestis MA. Cannabis (marijuana) - effects on human behavior and performance. Central Police University Press; Taipei: 2002. pp. 15–60. [PubMed] [Google Scholar]
- 37.Maldonado R, Berrendero F, Ozaita A, Robledo P. Neuroscience. 2011;181:1. doi: 10.1016/j.neuroscience.2011.02.035. [DOI] [PubMed] [Google Scholar]
- 38.Ashton CH. Br J Anaesth. 1999;83:637. doi: 10.1093/bja/83.4.637. [DOI] [PubMed] [Google Scholar]
- 39.Ashton CH. Br J Psychiatry. 2001;178:101. doi: 10.1192/bjp.178.2.101. [DOI] [PubMed] [Google Scholar]
- 40.Wright S. Mol Neurobiol. 2007;36:129. doi: 10.1007/s12035-007-0003-4. [DOI] [PubMed] [Google Scholar]
- 41.Di Marzo V, Petrocellis LD. Annu Rev Med. 2006;57:553. doi: 10.1146/annurev.med.57.011205.135648. [DOI] [PubMed] [Google Scholar]
- 42.Guzmán M. Nat Rev Cancer. 2003;3:745. doi: 10.1038/nrc1188. [DOI] [PubMed] [Google Scholar]
- 43.Hart CL, Haney M, Ward AS, Fischman MW, Foltin RW. Drug Alcohol Depend. 2002;67:301. doi: 10.1016/s0376-8716(02)00084-4. [DOI] [PubMed] [Google Scholar]
- 44.U.S. Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.DrugDetails.
- 45.Oreja-Guevara C. Expert Rev Neurother. 2012;12:3. doi: 10.1586/ern.12.11. [DOI] [PubMed] [Google Scholar]
- 46.Portenoy RK, Ganae-Motan ED, Allende S, Yanagihara R, Shaiova L, Weinstein S, McQuade R, Wright S, Fallon MT. J Pain. 2012;13:438. doi: 10.1016/j.jpain.2012.01.003. [DOI] [PubMed] [Google Scholar]
- 47.Pil K, Verstraete A. Ther Drug Monit. 2008;30:196. doi: 10.1097/FTD.0b013e318167d563. [DOI] [PubMed] [Google Scholar]
- 48.Moore C. Drug Test Anal. 2012;4:89. doi: 10.1002/dta.322. [DOI] [PubMed] [Google Scholar]
- 49.Bosker WM, Huestis MA. Clin Chem. 2009;55:1910. doi: 10.1373/clinchem.2008.108670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Choo RE, Huestis MA. Clin Chem Lab Med. 2004;42:1273. doi: 10.1515/CCLM.2004.248. [DOI] [PubMed] [Google Scholar]
- 51.Huestis MA, Cone EJ. J Anal Toxicol. 2004;28:394. doi: 10.1093/jat/28.6.394. [DOI] [PubMed] [Google Scholar]
- 52.Gjerde H, Normann PT, Christophersen AS. J Anal Toxicol. 2010;34:416. doi: 10.1093/jat/34.7.416. [DOI] [PubMed] [Google Scholar]
- 53.Ramaekers JG, Berghaus G, van Laar M, Drummer OH. Drug Alcohol Depend. 2004;73:109. doi: 10.1016/j.drugalcdep.2003.10.008. [DOI] [PubMed] [Google Scholar]
- 54.Hartman RL, Huestis MA. Clin Chem. 2012;59:478. doi: 10.1373/clinchem.2012.194381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Chait LD, Perry JL. Psychopharmacology (Berl) 1994;115:340. doi: 10.1007/BF02245075. [DOI] [PubMed] [Google Scholar]
- 56.Ramaekers JG, Robbe HW, O’Hanlon JF. Hum Psychopharmacol. 2000;15:551. doi: 10.1002/1099-1077(200010)15:7<551::AID-HUP236>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 57.Ramaekers JG, Moeller MR, van Ruitenbeek P, Theunissen EL, Schneider E, Kauert G. Drug Alcohol Depend. 2006;85:114. doi: 10.1016/j.drugalcdep.2006.03.015. [DOI] [PubMed] [Google Scholar]
- 58.Ramaekers JG, Kauert G, Theunissen EL, Toennes SW, Moeller MR. J Psychopharmacol. 2009;23:266. doi: 10.1177/0269881108092393. [DOI] [PubMed] [Google Scholar]
- 59.Lenné MG, Dietze PM, Triggs TJ, Walmsley S, Murphy B, Redman JR. Accid Anal Prev. 2010;42:859. doi: 10.1016/j.aap.2009.04.021. [DOI] [PubMed] [Google Scholar]
- 60.Ronen A, Gershon P, Drobiner H, Rabinovich A, Bar-Hamburger R, Mechoulam R, Cassuto Y, Shinar D. Accid Anal Prev. 2008;40:926. doi: 10.1016/j.aap.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 61.Ronen A, Chassidim HS, Gershon P, Parmet Y, Rabinovich A, Bar-Hamburger R, Cassuto Y, Shinar D. Accid Anal Prev. 2010;42:1855. doi: 10.1016/j.aap.2010.05.006. [DOI] [PubMed] [Google Scholar]
- 62.Drummer OH, Gerostamoulos J, Batziris H, Chu M, Caplehorn J, Robertson MD, Swann P. Accid Anal Prev. 2004;36:239. doi: 10.1016/s0001-4575(02)00153-7. [DOI] [PubMed] [Google Scholar]
- 63.Bédard M, Dubois S, Weaver B. Can J Public Health. 2007;98:6. doi: 10.1007/BF03405376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Laumon B, Gadegbeku B, Martin JL, Biecheler MB. BMJ. 2005;331:1371. doi: 10.1136/bmj.38648.617986.1F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Li MC, Brady JE, DiMaggio CJ, Lusardi AR, Tzong KY, Li G. Epidemiol Rev. 2012;34:65. doi: 10.1093/epirev/mxr017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Asbridge M, Hayden JA, Cartwright JL. BMJ. 2012;344:e536. doi: 10.1136/bmj.e536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Macdonald S, Hall W, Roman P, Stockwell T, Coghlan M, Nesvaag S. Addiction. 2010;105:408. doi: 10.1111/j.1360-0443.2009.02808.x. [DOI] [PubMed] [Google Scholar]
- 68.French MT, Roebuck MC, Kébreau Alexandre P. Soc Sci Res. 2004;33:45. doi: 10.1016/s0049-089x(03)00038-3. [DOI] [PubMed] [Google Scholar]
- 69.Vignali C, Stramesi C, Morini L, Pozzi F, Collo G, Groppi A. Drug Test Anal. 2013 doi: 10.1002/dta.1458. In press. [DOI] [PubMed] [Google Scholar]
- 70.Manchikanti L, Cash KA, Damron KS, Manchukonda R, Pampati V, McManus CD. Pain Physician. 2006;9:215. [PubMed] [Google Scholar]
- 71.Ware MA, Doyle CR, Woods R, Lynch ME, Clark AJ. Pain. 2003;102:211. doi: 10.1016/s0304-3959(02)00400-1. [DOI] [PubMed] [Google Scholar]
- 72.Ware MA, Rueda S, Singer J, Kilby D. J Cannabis Ther. 2003;3:3. [Google Scholar]
- 73.Clark AJ, Ware MA, Yazer E, Murray TJ, Lynch ME. Neurology. 2004;62:2098. doi: 10.1212/01.wnl.0000127707.07621.72. [DOI] [PubMed] [Google Scholar]
- 74.Ware MA, Adams H, Guy GW. Int J Clin Pract. 2005;59:291. doi: 10.1111/j.1742-1241.2004.00271.x. [DOI] [PubMed] [Google Scholar]
- 75.Compton P. Pain Manag Nurs. 2007;8:166. doi: 10.1016/j.pmn.2007.06.001. [DOI] [PubMed] [Google Scholar]
- 76.Katz NP, Sherburne S, Beach M, Rose RJ, Vielguth J, Bradley J, Fanciullo GJ. Anesth Analg. 2003;97:1097. doi: 10.1213/01.ANE.0000080159.83342.B5. [DOI] [PubMed] [Google Scholar]
- 77.Pesce A, West C, Gonzales E, Rosenthal M, West R, Mikel C, Almazan P, Latyshev S, Horn P. Pain Physician. 2012;15:E687. [PubMed] [Google Scholar]
- 78.Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS. Clin J Pain. 1999;15:184. doi: 10.1097/00002508-199909000-00005. [DOI] [PubMed] [Google Scholar]
- 79.Magura S, Kang SY. Subst Use Misuse. 1996;31:1131. doi: 10.3109/10826089609063969. [DOI] [PubMed] [Google Scholar]
- 80.Harrison L. NIDA Res Monogr. 1997;167:17. [PubMed] [Google Scholar]
- 81.Akinci IH, Tarter RE, Kirisci L. Addict Behav. 2001;26:613. doi: 10.1016/s0306-4603(00)00146-5. [DOI] [PubMed] [Google Scholar]
- 82.Budney AJ, Moore BA, Vandrey RG, Hughes JR. J Abnorm Psychol. 2003;112:393. doi: 10.1037/0021-843x.112.3.393. [DOI] [PubMed] [Google Scholar]
- 83.Kouri EM, Pope HG. Exp Clin Psychopharmacol. 2000;8:483. doi: 10.1037//1064-1297.8.4.483. [DOI] [PubMed] [Google Scholar]
- 84.Huestis MA, Mazzoni I, Rabin O. Sports Med. 2011;41:949. doi: 10.2165/11591430-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.World Anti-Doping Agency. 2011 Laboratory Testing Figures [Google Scholar]
- 86.Lorente FO, Peretti-Watel P, Grelot L. Addict Behav. 2005;30:1382. doi: 10.1016/j.addbeh.2005.01.019. [DOI] [PubMed] [Google Scholar]
- 87.Peretti-Watel P, Guagliardo V, Verger P, Pruvost J, Mignon P, Obadia Y. Addiction. 2003;98:1249. doi: 10.1046/j.1360-0443.2003.00490.x. [DOI] [PubMed] [Google Scholar]
- 88.World Anti-Doping Agency. International Standard for Laboratories Version 7.0. 2012 [Google Scholar]
- 89.Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Oral Dis. 2002;8:117. doi: 10.1034/j.1601-0825.2002.02851.x. [DOI] [PubMed] [Google Scholar]
- 90.Höld KM, de Boer D, Zuidema J, Maes RAA. Int J Drug Test. 1996;1:1. [Google Scholar]
- 91.Aps JK, Martens LC. Forensic Sci Int. 2005;150:119. doi: 10.1016/j.forsciint.2004.10.026. [DOI] [PubMed] [Google Scholar]
- 92.Edgar WM. Br Dent J. 1992;172:305. doi: 10.1038/sj.bdj.4807861. [DOI] [PubMed] [Google Scholar]
- 93.de Almeida Pdel V, Grégio AM, Machado MA, de Lima AA, Azevedo LR. J Contemp Dent Pract. 2008;9:72. [PubMed] [Google Scholar]
- 94.Vining RF, McGinley RA. Crit Rev Clin Lab Sci. 1986;23:95. doi: 10.3109/10408368609165797. [DOI] [PubMed] [Google Scholar]
- 95.Vondracek M, Xi Z, Larsson P, Baker V, Mace K, Pfeifer A, Tjälve H, Donato MT, Gomez-Lechon MJ, Grafström RC. Carcinogenesis. 2001;22:421. doi: 10.1093/carcin/22.3.481. [DOI] [PubMed] [Google Scholar]
- 96.Yang SP, Raner GM. Toxicol Appl Pharmacol. 2005;202:140. doi: 10.1016/j.taap.2004.06.014. [DOI] [PubMed] [Google Scholar]
- 97.Sacks PG, Zhao ZL, Kosinska W, Fleisher KE, Gordon T, Guttenplan JB. Food Chem Toxicol. 2011;49:2348. doi: 10.1016/j.fct.2011.06.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Zhou LX, Pihlstrom B, Hardwick JP, Park SS, Wrighton SA, Holtzman JL. Clin Pharmacol Ther. 1996;60:191. doi: 10.1016/S0009-9236(96)90135-6. [DOI] [PubMed] [Google Scholar]
- 99.Huestis MA. Pharmacokinetics and metabolism of the plant cannabinoids, delta-9-tetrahydrocannabinol, cannabidiol and cannabinol. Springer; New York: 2005. [DOI] [PubMed] [Google Scholar]
- 100.Watanabe K, Yamaori S, Funahashi T, Kimura T, Yamamoto I. Life Sci. 2007;80:1415. doi: 10.1016/j.lfs.2006.12.032. [DOI] [PubMed] [Google Scholar]
- 101.Maurer HH, Sauer C, Theobald DS. Ther Drug Monit. 2006;28:447. doi: 10.1097/01.ftd.0000211812.27558.6e. [DOI] [PubMed] [Google Scholar]
- 102.Wall ME, Sadler BM, Brine D, Taylor H, Perez-Reyes M. Clin Pharmacol Ther. 1983;34:352. doi: 10.1038/clpt.1983.179. [DOI] [PubMed] [Google Scholar]
- 103.Widman M, Nordqvist M, Dollery CT, Briant RH. J Pharm Pharmacol. 1975;27:842. doi: 10.1111/j.2042-7158.1975.tb10227.x. [DOI] [PubMed] [Google Scholar]
- 104.Greene ML, Saunders DR. Gastroenterology. 1974;66:365. [PubMed] [Google Scholar]
- 105.Watanabe K, Tanaka T, Yamamoto I, Yoshimura H. Biochem Biophys Res Commun. 1988;157:75. doi: 10.1016/s0006-291x(88)80013-5. [DOI] [PubMed] [Google Scholar]
- 106.Krishna DR, Klotz U. Clin Pharmacokinet. 1994;26:144. doi: 10.2165/00003088-199426020-00007. [DOI] [PubMed] [Google Scholar]
- 107.Davenport HW. Physiology of the digestive tract: an introductory text. Year Book Medical Publishers; Chicago: 1977. pp. 85–94. [Google Scholar]
- 108.Crouch DJ. Forensic Sci Int. 2005;150:165. doi: 10.1016/j.forsciint.2005.02.028. [DOI] [PubMed] [Google Scholar]
- 109.Humphrey SP, Williamson RT. J Prosthet Dent. 2001;2001:126. doi: 10.1067/mpr.2001.113778. [DOI] [PubMed] [Google Scholar]
- 110.Lafolie P, Beck O, Blennow G, Boréus L, Borg S, Elwin CE, Karlsson L, Odelius G, Hjemdahl P. Clin Chem. 1991;37:1927. [PubMed] [Google Scholar]
- 111.Smith ML, Barnes AJ, Huestis MA. J Anal Toxicol. 2009;33:185. doi: 10.1093/jat/33.4.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Chiou WL, Hsu FH, Westenfelder C, Kurtzman NA. Res Commun Chem Pathol Pharmacol. 1977;16:549. [PubMed] [Google Scholar]
- 113.Chiou WL, Pu FS. Clin Pharmacol Ther. 1979;25:777. doi: 10.1002/cpt1979256777. [DOI] [PubMed] [Google Scholar]
- 114.Lee D, Schwope DM, Milman G, Barnes AJ, Gorelick DA, Huestis MA. Clin Chem. 2012;58:748. doi: 10.1373/clinchem.2011.177881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Lee D, Karschner EL, Milman G, Barnes AJ, Goodwin RS, Huestis MA. Drug Alcohol Depend. 2013;130:68. doi: 10.1016/j.drugalcdep.2012.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Kauert GF, Ramaekers JG, Schneider E, Moeller MR, Toennes SW. J Anal Toxicol. 2007;31:288. doi: 10.1093/jat/31.5.288. [DOI] [PubMed] [Google Scholar]
- 117.Mechoulam R, Parker LA, Gallily R. J Clin Pharmacol. 2002;42:11S. doi: 10.1002/j.1552-4604.2002.tb05998.x. [DOI] [PubMed] [Google Scholar]
- 118.Gomes FV, Resstel LB, Guimarães FS. Psychopharmacology (Berl) 2011;213:465. doi: 10.1007/s00213-010-2036-z. [DOI] [PubMed] [Google Scholar]
- 119.Zuardi AW, Crippa JA, Hallak JE, Moreira FA, Guimarães FS. Braz J Med Biol Res. 2006;39:421. doi: 10.1590/s0100-879x2006000400001. [DOI] [PubMed] [Google Scholar]
- 120.Zuardi AW, Shirakawa I, Finkelfarb E, Karniol IG. Psychopharmacology (Berl) 1982;76:245. doi: 10.1007/BF00432554. [DOI] [PubMed] [Google Scholar]
- 121.Karniol IG, Shirakawa I, Kasinski N, Pfeferman A, Carlini EA. Eur J Pharmacol. 1974;28:172. doi: 10.1016/0014-2999(74)90129-0. [DOI] [PubMed] [Google Scholar]
- 122.ElSohly MA. Chemical Constituents of Cannabis. Haworth Integrative Healing Press; New York: 2002. [Google Scholar]
- 123.Turner CE, Elsohly MA, Boeren EG. J Nat Prod. 1980;43:169. doi: 10.1021/np50008a001. [DOI] [PubMed] [Google Scholar]
- 124.Davis KH, McDaniel IA, Cadwell IW, Moody PL. Some smoking characteristics of marijuana cigarettes. Academic Press; Orlando: 1984. [Google Scholar]
- 125.Pomahacova B, Van der Kooy F, Verpoorte R. Inhal Toxicol. 2009;21:1108. doi: 10.3109/08958370902748559. [DOI] [PubMed] [Google Scholar]
- 126.Day D, Kuntz DJ, Feldman M, Presley L. J Anal Toxicol. 2006;30:645. doi: 10.1093/jat/30.9.645. [DOI] [PubMed] [Google Scholar]
- 127.Moore C, Coulter C, Uges D, Tuyay J, van der Linde S, van Leeuwen A, Garnier M, Orbita J. Forensic Sci Int. 2011;212:227. doi: 10.1016/j.forsciint.2011.06.019. [DOI] [PubMed] [Google Scholar]
- 128.Moore C, Rana S, Coulter C, Day D, Vincent M, Soares J. J Anal Toxicol. 2007;31:187. doi: 10.1093/jat/31.4.187. [DOI] [PubMed] [Google Scholar]
- 129.Walz A, Stühler K, Wattenberg A, Hawranke E, Meyer HE, Schmalz G, Blüggel M, Ruhl S. Proteomics. 2006;6:1631. doi: 10.1002/pmic.200500125. [DOI] [PubMed] [Google Scholar]
- 130.Versteeg PA, Slot DE, van der Velden U, van der Weijden GA. Int J Dent Hyg. 2008;6:315. doi: 10.1111/j.1601-5037.2008.00301.x. [DOI] [PubMed] [Google Scholar]
- 131.Milman G, Schwope DM, Gorelick DA, Huestis MA. Clin Chim Acta. 2012;413:765. doi: 10.1016/j.cca.2012.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Darling MR, Arendorf TM. Community Dent Oral Epidemiol. 1993;21:78. doi: 10.1111/j.1600-0528.1993.tb00725.x. [DOI] [PubMed] [Google Scholar]
- 133.Walsh JM. A State-by-State analysis of laws dealing with driving under the influence of drugs National Highway Traffic Safety Administration. 2009 DOT HS 811 236. [Google Scholar]
- 134.Canada Federal Legislation. Criminal Code. http://laws-lois.justice.gc.ca/eng/acts/C-46/
- 135.Bush DM. Forensic Sci Int. 2008;174:111. doi: 10.1016/j.forsciint.2007.03.008. [DOI] [PubMed] [Google Scholar]
- 136.OraSure. http://www.orasure.com/docs/pdfs/products/intercept/Oral_Fluid-Common_Myths.pdf.
- 137.WFC & Associates. http://www.statedrugtestinglaws.com/newsletter.
- 138.Standards Australia. Australian Standard AS 4760-2006: Procedures for specimen collection and the detection and quantitation of drugs in oral fluid. 2006 [Google Scholar]
- 139.Barbara Butler and Associates Inc. Recent Alcohol and Drug Workplace Policies in Canada - Considerations for the Nuclear Industry Canadian Nuclear Safety Commission. 2012 INFO-0831. [Google Scholar]
- 140.European Workplace Drug Testing Society. Guidelines for Oral Fluid, version 001. doi: 10.1002/dta.284. http://www.ewdts.org/guidelines.html. [DOI] [PubMed]
- 141.Drummer OH, Gerostamoulos D, Chu M, Swann P, Boorman M, Cairns I. Forensic Sci Int. 2007;170:105. doi: 10.1016/j.forsciint.2007.03.028. [DOI] [PubMed] [Google Scholar]
- 142.Davey J, Freeman J. Traffic Inj Prev. 2009;10:231. doi: 10.1080/15389580902826817. [DOI] [PubMed] [Google Scholar]
- 143.Simonsen KW, Steentoft A, Hels T, Bernhoft IM, Rasmussen BS, Linnet K. Forensic Sci Int. 2012;221:33. doi: 10.1016/j.forsciint.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 144.Heltsley R, DePriest A, Black DL, Robert T, Marshall L, Meadors VM, Caplan YH, Cone EJ. J Anal Toxicol. 2011;35:529. doi: 10.1093/anatox/35.8.529. [DOI] [PubMed] [Google Scholar]
- 145.Kork F, Kleinwächter R, Weiss-Gerlach E, Broecker S, Pragst F, Wernecke KD, Spies C. J Int Med Res. 2012;40:194. doi: 10.1177/147323001204000120. [DOI] [PubMed] [Google Scholar]
- 146.Gjerde H, Christophersen AS, Moan IS, Yttredal B, Walsh JM, Normann PT, Mørland J. J Occup Med Toxicol. 2010;5:1. doi: 10.1186/1745-6673-5-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Toennes SW, Ramaekers JG, Theunissen EL, Moeller MR, Kauert GF. J Anal Toxicol. 2010;34:216. doi: 10.1093/jat/34.4.216. [DOI] [PubMed] [Google Scholar]
- 148.Niedbala RS, Kardos KW, Fritch DF, Kardos S, Fries T, Waga J, Robb J, Cone EJ. J Anal Toxicol. 2001;25:289. doi: 10.1093/jat/25.5.289. [DOI] [PubMed] [Google Scholar]
- 149.Lee D, Milman G, Schwope DM, Barnes AJ, Gorelick DA, Huestis MA. Clin Chem. 2012;58:1101. doi: 10.1373/clinchem.2012.184929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Milman G, Barnes AJ, Schwope DM, Schwilke EW, Goodwin RS, Kelly DL, Gorelick DA, Huestis MA. Anal Bioanal Chem. 2011;401:599. doi: 10.1007/s00216-011-5066-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Teixeira H, Proença P, Verstraete A, Corte-Real F, Vieira DN. Forensic Sci Int. 2005;150:205. doi: 10.1016/j.forsciint.2004.11.026. [DOI] [PubMed] [Google Scholar]
- 152.Menkes DB, Howard RC, Spears GF, Cairns ER. Psychopharmacology (Berl) 1991;103:277. doi: 10.1007/BF02244217. [DOI] [PubMed] [Google Scholar]
- 153.Lee D, Milman G, Barnes AJ, Goodwin RS, Hirvonen J, Huestis MA. Clin Chem. 2011;57:1127. doi: 10.1373/clinchem.2011.164822. [DOI] [PubMed] [Google Scholar]
- 154.Moore C, Rana S, Coulter C. J Chromatogr B Analyt Technol Biomed Life Sci. 2007;852:459. doi: 10.1016/j.jchromb.2007.02.016. [DOI] [PubMed] [Google Scholar]
- 155.Moore C, Coulter C, Rana S, Vincent M, Soares J. J Anal Toxicol. 2006;30:409. doi: 10.1093/jat/30.7.409. [DOI] [PubMed] [Google Scholar]
- 156.Schwope DM, Karschner EL, Gorelick DA, Huestis MA. Clin Chem. 2011;57:1406. doi: 10.1373/clinchem.2011.171777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Cone EJ, Clarke J, Tsanaclis L. J Anal Toxicol. 2007;31:424. doi: 10.1093/jat/31.8.424. [DOI] [PubMed] [Google Scholar]
- 158.Milman G, Barnes AJ, Schwope DM, Schwilke EW, Darwin WD, Goodwin RS, Kelly DL, Gorelick DA, Huestis MA. Clin Chem. 2010;56:1261. doi: 10.1373/clinchem.2009.141853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Bergamaschi MM, Karschner EL, Goodwin RS, Scheidweiler KB, Hirvonen J, Queiroz RH, Huestis MA. Clin Chem. 2013;59:519. doi: 10.1373/clinchem.2012.195503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Curran HV, Brignell C, Fletcher S, Middleton P, Henry J. Psychopharmacology (Berl) 2002;164:61. doi: 10.1007/s00213-002-1169-0. [DOI] [PubMed] [Google Scholar]
- 161.Schwope DM, Bosker WM, Ramaekers JG, Gorelick DA, Huestis MA. J Anal Toxicol. 2012;36:405. doi: 10.1093/jat/bks044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Wille SM, Raes E, Lillsunde P, Gunnar T, Laloup M, Samyn N, Christophersen AS, Moeller MR, Hammer KP, Verstraete AG. Ther Drug Monit. 2009;31:511. doi: 10.1097/FTD.0b013e3181ae46ea. [DOI] [PubMed] [Google Scholar]
- 163.Gjerde H, Mordal J, Christophersen AS, Bramness JG, Mørland J. J Anal Toxicol. 2010;34:204. doi: 10.1093/jat/34.4.204. [DOI] [PubMed] [Google Scholar]
- 164.Vindenes V, Lund HME, Andresen W, Gjerde H, Ikdahl SE, Christophersen AS, Øiestad EL. Forensic Sci Int. 2012;219:165. doi: 10.1016/j.forsciint.2012.01.001. [DOI] [PubMed] [Google Scholar]
- 165.Samyn N, van Haeren C. Int J Legal Med. 2000;113:150. doi: 10.1007/s004140050287. [DOI] [PubMed] [Google Scholar]
- 166.Milman G, Schwope DM, Schwilke EW, Darwin WD, Kelly DL, Goodwin RS, Gorelick DA, Huestis MA. Clin Chem. 2011;57:1597. doi: 10.1373/clinchem.2011.169490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Gjerde H, Verstraete AG. Forensic Sci Int. 2011;212:e26. doi: 10.1016/j.forsciint.2011.06.024. [DOI] [PubMed] [Google Scholar]
- 168.Heltsley R, Depriest A, Black DL, Crouch DJ, Robert T, Marshall L, Meadors VM, Caplan YH, Cone EJ. J Anal Toxicol. 2012;36:75. doi: 10.1093/jat/bkr019. [DOI] [PubMed] [Google Scholar]
- 169.Huestis MA, Cone EJ. J Anal Toxicol. 1998;22:445. doi: 10.1093/jat/22.6.445. [DOI] [PubMed] [Google Scholar]
- 170.Lowe RH, Abraham TT, Darwin WD, Herning R, Cadet JL, Huestis MA. Drug Alcohol Depend. 2009;105:24. doi: 10.1016/j.drugalcdep.2009.05.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Ellis GM, Mann MA, Judson BA, Schramm NT, Tashchian A. Clin Pharmacol Ther. 1985;38:572. doi: 10.1038/clpt.1985.226. [DOI] [PubMed] [Google Scholar]
- 172.Schwilke EW, Gullberg RG, Darwin WD, Chiang CN, Cadet JL, Gorelick DA, Pope HG, Huestis MA. Addiction. 2011;106:499. doi: 10.1111/j.1360-0443.2010.03228.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Toennes SW, Kauert GF, Steinmeyer S, Moeller MR. Forensic Sci Int. 2005;152:149. doi: 10.1016/j.forsciint.2004.08.002. [DOI] [PubMed] [Google Scholar]
- 174.Grotenhermen F. Clin Pharmacokinetics. 2003;42:327. doi: 10.2165/00003088-200342040-00003. [DOI] [PubMed] [Google Scholar]
- 175.Leuschner JT, Harvey DJ, Bullingham RE, Paton WD. Drug Metab Dispos. 1986;14:230. [PubMed] [Google Scholar]
- 176.Hunt CA, Jones RT. J Pharmacol Exp Ther. 1980;215:35. [PubMed] [Google Scholar]
- 177.Bosker WM, Karschner EL, Lee D, Goodwin RS, Hirvonen J, Innis RB, Theunissen EL, Kuypers KPC, Huestis MA, Ramaekers JG. PLoS One. 2013:e53127. doi: 10.1371/journal.pone.0053127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Pope HG, Gruber AJ, Hudson JI, Huestis MA, Yurgelun-Todd D. Arch Gen Psychiatry. 2001;58:909. doi: 10.1001/archpsyc.58.10.909. [DOI] [PubMed] [Google Scholar]
- 179.Bolla KI, Brown K, Eldreth D, Tate K, Cadet JL. Neurology. 2002;59:133. doi: 10.1212/01.wnl.0000031422.66442.49. [DOI] [PubMed] [Google Scholar]
- 180.Hirvonen J, Goodwin RS, Li CT, Terry GE, Zoghbi SS, Morse C, Pike VW, Volkow ND, Huestis MA, Innis RB. Mol Psychiatry. 2012;17:642. doi: 10.1038/mp.2011.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Molnar A, Lewis J, Fu S. Forensic Sci Int. 2012 doi: 10.1016/j.forsciint.2011.01.045. [DOI] [PubMed] [Google Scholar]
- 182.Drummer OH. Clin Biochem Rev. 2006;27:147. [PMC free article] [PubMed] [Google Scholar]
- 183.Dawes C, Macpherson LMD. Caries Res. 1992;26:176. doi: 10.1159/000261439. [DOI] [PubMed] [Google Scholar]
- 184.Langel K, Engblom C, Pehrsson A, Gunnar T, Ariniemi K, Lillsunde P. J Anal Toxicol. 2008;32:393. doi: 10.1093/jat/32.6.393. [DOI] [PubMed] [Google Scholar]
- 185.Kauert GF, Iwersen-Bergmann S, Toennes SW. J Anal Toxicol. 2006;30:274. doi: 10.1093/jat/30.4.274. [DOI] [PubMed] [Google Scholar]
- 186.Coulter C, Garnier M, Moore C. J Anal Toxicol. 2012;36:413. doi: 10.1093/jat/bks039. [DOI] [PubMed] [Google Scholar]
- 187.Cairns ER, Howard RC, Hung CT, Menkes DB. Saliva THC levels and cannabis intoxication Department of Scientific and Industrial Research. New Zealand: Chemistry Division Report No. 2411. [Google Scholar]
- 188.Just WW, Filipovic N, Werner G. J Chromatogr. 1974;96:189. doi: 10.1016/s0021-9673(00)98561-3. [DOI] [PubMed] [Google Scholar]
- 189.Gross SJ, Worthy TE, Nerder L, Zimmermann EG, Soares JR, Lomax P. J Anal Toxicol. 1985;9:1. doi: 10.1093/jat/9.1.1. [DOI] [PubMed] [Google Scholar]
- 190.Schwope DM, Milman G, Huestis MA. Clin Chem. 2010;56:1007. doi: 10.1373/clinchem.2009.141754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191.Clarke J, Wilson JF. Forensic Sci Int. 2005;150:161. doi: 10.1016/j.forsciint.2004.11.025. [DOI] [PubMed] [Google Scholar]
- 192.Øiestad EL, Johansen U, Christophersen AS. Clin Chem. 2007;53:300. doi: 10.1373/clinchem.2006.074237. [DOI] [PubMed] [Google Scholar]
- 193.Wille SM, Ramírez-Fernandez Mdel M, Samyn N, De Boeck G. Bioanalysis. 2010;2:791. doi: 10.4155/bio.10.29. [DOI] [PubMed] [Google Scholar]
- 194.Verstraete A. Drugs of abuse: body fluid testing. Humana Press Inc.; Totowa, NJ: 2005. pp. 271–92. [Google Scholar]
- 195.Verstraete AG, Raes E, editors. Rosita-2 project: final report. www.rosita.org/docs/Rosita2%20Final%20report%20May2006.pdf.
- 196.Kintz P, Bernhard W, Villain M, Gasser M, Aebi B, Cirimele V. J Anal Toxicol. 2005;29:724. doi: 10.1093/jat/29.7.724. [DOI] [PubMed] [Google Scholar]
- 197.Gallardo E, Queiroz JA. Biomed Chromatogr. 2008;22:795. doi: 10.1002/bmc.1009. [DOI] [PubMed] [Google Scholar]
- 198.Blencowe T, Pehrsson A, Lillsunde P, Vimpari K, Houwing S, Smink B, Mathijssen R, Van der Linden T, Legrand SA, Pil K, Verstraete A. Forensic Sci Int. 2011;208:173. doi: 10.1016/j.forsciint.2010.11.026. [DOI] [PubMed] [Google Scholar]
- 199.Strano-Rossi S, Castrignanò E, Anzillotti L, Serpelloni G, Mollica R, Tagliaro F, Pascali JP, di Stefano D, Sgalla R, M C. Forensic Sci Int. 2012;221:70. doi: 10.1016/j.forsciint.2012.04.003. [DOI] [PubMed] [Google Scholar]
- 200.Desrosiers NA, Lee D, Schwope DM, Milman G, Barnes AJ, Gorelick DA, Huestis MA. Clin Chem. 2012;58:1418. doi: 10.1373/clinchem.2012.189001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201.Maseda C, Hama K, Fukui Y, Matsubara K, Takahashi S, Akane A. Forensic Sci Int. 1986;32:259. doi: 10.1016/0379-0738(86)90202-1. [DOI] [PubMed] [Google Scholar]
- 202.Peel HW, Perrigo BJ, Mikhael NZ. J Forensic Sci. 1984;29:185. [PubMed] [Google Scholar]
- 203.Valentine JL, Bryant PJ, Gutshall PL, Gan OH, Thompson ED, Niu HC. NIDA Res Monogr. 1976;7:96. [PubMed] [Google Scholar]
- 204.Thompson LK, Cone EJ. J Chromatogr. 1987;421:91. doi: 10.1016/0378-4347(87)80382-1. [DOI] [PubMed] [Google Scholar]
- 205.Kircher V, Parlar H. J Chromatogr B Biomed Appl. 1996;677:245. doi: 10.1016/0378-4347(95)00451-3. [DOI] [PubMed] [Google Scholar]
- 206.Hall BJ, Satterfield-Doerr M, Parikh AR, Brodbelt JS. Anal Chem. 1998;70:1788. doi: 10.1021/ac971228g. [DOI] [PubMed] [Google Scholar]
- 207.Fucci N, De Giovanni N, Chiarotti M. Forensic Sci Int. 2003;134:40. doi: 10.1016/s0379-0738(03)00098-7. [DOI] [PubMed] [Google Scholar]
- 208.Yonamine M, Tawil N, Moreau RL, Silva OA. J Chromatogr B Analyt Technol Biomed Life Sci. 2003;789:73. doi: 10.1016/s1570-0232(03)00165-x. [DOI] [PubMed] [Google Scholar]
- 209.Choi H, Baeck S, Kim E, Lee S, Jang M, Lee J, Choi H, Chung H. Sci Justice. 2009;49:242. doi: 10.1016/j.scijus.2009.09.015. [DOI] [PubMed] [Google Scholar]
- 210.Sergi M, Bafile E, Compagnone D, Curini R, D’Ascenzo G, Romolo FS. Anal Bioanal Chem. 2009;393:709. doi: 10.1007/s00216-008-2456-3. [DOI] [PubMed] [Google Scholar]
- 211.Quintela O, Andrenyak DM, Hoggan AM, Crouch DJ. J Anal Toxicol. 2007;31:157. doi: 10.1093/jat/31.3.157. [DOI] [PubMed] [Google Scholar]
- 212.Concheiro M, de Castro A, Quintela O, Cruz A, López-Rivadulla M. Anal Bioanal Chem. 2008;391:2329. doi: 10.1007/s00216-008-2135-4. [DOI] [PubMed] [Google Scholar]
- 213.Badawi N, Simonsen KW, Steentoft A, Bernhoft IM, Linnet K. Clin Chem. 2009;55:2004. doi: 10.1373/clinchem.2008.122341. [DOI] [PubMed] [Google Scholar]
- 214.Gunnar T, Ariniemi K, Lillsunde P. J Mass Spectrom. 2005;40:739. doi: 10.1002/jms.846. [DOI] [PubMed] [Google Scholar]
- 215.Milman G, Barnes AJ, Lowe RH, Huestis MA. J Chromatogr A. 2010;1217:1513. doi: 10.1016/j.chroma.2009.12.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 216.Scheidweiler KB, Himes SK, Chen X, Liu HF, Huestis MA. Anal Bioanal Chem. 2013 doi: 10.1007/s00216-013-7027-6. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 217.He X, Kozak M, Nimkar S. Anal Chem. 2012;84:7643. doi: 10.1021/ac3019476. [DOI] [PubMed] [Google Scholar]
- 218.Concheiro M, Lee D, Lendoiro E, Huestis MA. J Chromatogr A. 2013;1297:123. doi: 10.1016/j.chroma.2013.04.071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219.Lee PD, Chang YJ, Lin KL, Chang YZ. Anal Bioanal Chem. 2012;402:851. doi: 10.1007/s00216-011-5439-8. [DOI] [PubMed] [Google Scholar]
- 220.Moore C, Vincent M, Rana S, Coulter C, Agrawal A, Soares J. Forensic Sci Int. 2006;164:126. doi: 10.1016/j.forsciint.2005.12.011. [DOI] [PubMed] [Google Scholar]
- 221.Molnar A, Lewis J, Doble P, Hansen G, Prolov T, Fu S. Forensic Sci Int. 2012;215:92. doi: 10.1016/j.forsciint.2011.01.045. [DOI] [PubMed] [Google Scholar]
- 222.Wong RC, Tran M, Tung JK. Forensic Sci Int. 2005;150:175. doi: 10.1016/j.forsciint.2005.02.023. [DOI] [PubMed] [Google Scholar]
- 223.Niedbala S, Kardos K, Salamone S, Fritch D, Bronsgeest M, Cone EJ. J Anal Toxicol. 2004;28:546. doi: 10.1093/jat/28.7.546. [DOI] [PubMed] [Google Scholar]
- 224.Niedbala RS, Kardos KW, Fritch DF, Kunsman KP, Blum KA, Newland GA, Waga J, Kurtz L, Bronsgeest M, Cone EJ. J Anal Toxicol. 2005;29:607. doi: 10.1093/jat/29.7.607. [DOI] [PubMed] [Google Scholar]
- 225.Project CBD. http://projectcbd.org/
- 226.Walsh JM, Verstraete AG, Huestis MA, Mørland J. Addiction. 2008;103:1258. doi: 10.1111/j.1360-0443.2008.02277.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227.Kintz P, Cirimele V, Ludes B. J Anal Toxicol. 2000;24:557. doi: 10.1093/jat/24.7.557. [DOI] [PubMed] [Google Scholar]
- 228.Gjerde H, Normann PT, Pettersen BS, Assum T, Aldrin M, Johansen U, Kristoffersen L, Øiestad EL, Christophersen AS, Mørland J. Accid Anal Prev. 2008;40:1765. doi: 10.1016/j.aap.2008.06.015. [DOI] [PubMed] [Google Scholar]
- 229.Zancanaro I, Limberger RP, Bohel PO, dos Santos MK, De Boni RB, Pechansky F, Caldas ED. Forensic Sci Int. 2012;223:208. doi: 10.1016/j.forsciint.2012.08.048. [DOI] [PubMed] [Google Scholar]
- 230.Gjerde H, Christophersen AS, Normann PT, Pettersen BS, Sabaredzovic A, Samuelsen SO, Mørland J. Traffic Inj Prev. 2012;13:43. doi: 10.1080/15389588.2011.627957. [DOI] [PubMed] [Google Scholar]
- 231.Gripenberg-Abdon J, Elgán TH, Wallin E, Shaafati M, Beck O, Andréasson S. Subst Abuse Treat Prev Policy. 2012;7:1. doi: 10.1186/1747-597X-7-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 232.Wille SM, Di Fazio V, Ramírez-Fernandez Mdel M, Kummer N, Samyn N. Ther Drug Monit. 2013;35:101. doi: 10.1097/FTD.0b013e318278dbe4. [DOI] [PubMed] [Google Scholar]
- 233.Speedy T, Baldwin D, Jowett G, Gallina M, Jehanli A. Forensic Sci Int. 2007;170:117. doi: 10.1016/j.forsciint.2007.03.038. [DOI] [PubMed] [Google Scholar]
- 234.Ventura M, Pichini S, Ventura R, Leal S, Zuccaro P, Pacifici R, de la Torre R. Ther Drug Monit. 2009;31:277. doi: 10.1097/FTD.0b013e318198670b. [DOI] [PubMed] [Google Scholar]
- 235.Quintela O, Crouch DJ, Adrenyak DM. J Anal Toxicol. 2006;30:614. doi: 10.1093/jat/30.8.614. [DOI] [PubMed] [Google Scholar]
- 236.Vanstechelman S, Isalberti C, Van der Linden T, Pil K, Legrand SA, Verstraete AG. J Anal Toxicol. 2012;36:136. doi: 10.1093/jat/bkr016. [DOI] [PubMed] [Google Scholar]
- 237.Kintz P, Brunet B, Muller JF, Serra W, Villain M, Cirimele V, Mura P. Ther Drug Monit. 2009;31:131. doi: 10.1097/FTD.0b013e3181947916. [DOI] [PubMed] [Google Scholar]
- 238.Concheiro M, de Castro A, Quintela O, Cruz A, López-Rivadulla M. Forensic Sci Int. 2007;170:156. doi: 10.1016/j.forsciint.2007.03.034. [DOI] [PubMed] [Google Scholar]
- 239.Wille SM, Samyn N, Ramírez-Fernández Mdel M, De Boeck G. Forensic Sci Int. 2010;198:2. doi: 10.1016/j.forsciint.2009.10.012. [DOI] [PubMed] [Google Scholar]
- 240.Walsh JM, Crouch DJ, Danaceau JP, Cangianelli L, Liddicoat L, Adkins R. J Anal Toxicol. 2007;31:44. doi: 10.1093/jat/31.1.44. [DOI] [PubMed] [Google Scholar]
- 241.Pehrsson A, Blencowe T, Vimpari K, Langel K, Engblom C, Lillsunde P. J Anal Toxicol. 2011;35:211. doi: 10.1093/anatox/35.4.211. [DOI] [PubMed] [Google Scholar]
- 242.Röhrich J, Zörntlein S, Becker J, Urban R. J Anal Toxicol. 2010;34:155. doi: 10.1093/jat/34.3.155. [DOI] [PubMed] [Google Scholar]
- 243.Concheiro M, de Castro A, Quintela O, Cruz A, López-Rivadulla M. J Chromatogr B Analyt Technol Biomed Life Sci. 2004;810:319. doi: 10.1016/j.jchromb.2004.08.017. [DOI] [PubMed] [Google Scholar]
- 244.Laloup M, Ramirez Fernandez Mdel M, Wood M, De Boeck G, Henquet C, Maes V, Samyn N. J Chromatogr A. 2005;1082:15. doi: 10.1016/j.chroma.2005.03.031. [DOI] [PubMed] [Google Scholar]
- 245.Pujadas M, Pichini S, Civit E, Santamariña E, Perez K, de la Torre R. J Pharm Biomed Anal. 2007;44:594. doi: 10.1016/j.jpba.2007.02.022. [DOI] [PubMed] [Google Scholar]
- 246.Teixeira H, Verstraete A, Proença P, Corte-Real F, Monsanto P, Vieira DN. Forensic Sci Int. 2007;107:148. doi: 10.1016/j.forsciint.2007.03.026. [DOI] [PubMed] [Google Scholar]
- 247.Fabritius M, Giroud C. Anal Bioanal Chem. 2013;405:435. doi: 10.1007/s00216-012-6515-4. [DOI] [PubMed] [Google Scholar]
- 248.Bylda C, Leinenbach A, Thiele R, Kobold U, Volmer DA. Drug Test Anal. 2012;4:668. doi: 10.1002/dta.1334. [DOI] [PubMed] [Google Scholar]