

Abstract
Setting: Forty hard-to-reach villages in the East and West Singhbhum Districts of Jharkhand State, India.
Objectives: To document knowledge and awareness of tuberculosis (TB) among the general population, understand gender differences and inform intervention activities for the improvement of TB control programmes in tribal-dominant hard-to-reach areas in India.
Design: A cross-sectional community-based survey was carried out among 825 respondents using population proportionate sampling.
Results: Most of the respondents were in the 18–35 years age group, tribal and married; 44% were illiterate. The study shows poor knowledge about TB symptoms, causes, modes of transmission and moderate awareness about government TB services. Correct knowledge about the cause of TB was negligible: half of the respondents reported local liquor as the cause, 61% considered TB as transmissible and one third considered sharing of food as the mode of transmission. Awareness about the availability of free treatment services at government health facilities was high, but awareness about DOTS was low. Significant gender differences were observed in knowledge and awareness levels.
Conclusion: Study findings point to the importance of urgent intensification of culturally congruent and gender-sensitive advocacy, communication and social mobilisation activities.
Keywords: community mobilisation, TB ACSM, tribal health, Jharkhand, India
Abstract
Contexte : Quarante villages difficiles d'accès de l'Est et de l'Ouest des districts de l'état de Singhbhum, Jharkhand, Inde.
Objectifs : Documenter les niveaux de connaissances et de sensibilisation en matière de la tuberculose (TB) parmi les membres de la communauté, de comprendre les différences entre les sexes et de contribuer à l'élaboration d'activités d'intervention afin d'améliorer le programme de lutte contre la TB dans des zones à dominante tribale difficiles d'accès en Inde.
Schéma : Une enquête transversale à base communautaire a été réalisée auprès de 825 répondants grâce à une méthode d'échantillonnage proportionnel de la population.
Résultats : La majorité des répondants appartenait à la tranche d'âge 18–35 ans, à une minorité ethnique et étaient mariés ; 44% étaient illettrés. L'étude a montré une faible connaissance des symptômes, causes et modes de transmission de la TB et une connaissance modérée des services gouvernementaux de TB. Les connaissances relatives à la cause exacte de la TB était négligeables—la moitié des répondants a attribué la TB à la consommation d'alcool local ; 61% savaient que la TB était transmissible et un tiers affirmait que le partage de nourriture était une voie de transmission. La connaissance de la disponibilité de services gratuits de prise en charge dans des structures de santé étatiques était élevée, mais la stratégie DOTS était très mal connue. Des différences significatives entre les sexes ont été observées en matière de niveau de connaissance et de sensibilisation.
Conclusion : Les résultats de l'étude soulignaient l'importance d'une intensification urgente des activités de plaidoyer, de communication et de mobilisation sociale culturellement adaptées et spécifiques au genre.
Abstract
Marco de referencia: Cuarenta poblaciones de difícil acceso de los distritos de Singhbhum oriental y occidental en el estado de Jharkhand de la India.
Objetivos: Documentar los conocimientos y la sensibilización en materia de tuberculosis (TB) de los miembros de la comunidad general, comprender las diferencias asociadas con el sexo y aportar recomendaciones a la formulación de intervenciones destinadas a mejorar el programa contra la TB en las zonas de difícil acceso con predominio de población tribal, en la India.
Método: Se llevó a cabo una encuesta transversal comunitaria a 825 personas escogidas mediante un muestreo proporcional a la población.
Resultados: La mayoría de las personas que respondieron a la encuesta se encontraba en el grupo etario de 18 años a 35 años, pertenecía a un grupo tribal y su estado civil era casado; el 44% era analfabeto. El estudio puso en evidencia un conocimiento precario de la TB con relación a los síntomas, las causas y los modos de transmisión y una sensibilización moderada a la existencia de servicios gubernamentales de atención de la TB. El grado de conocimientos sobre causa real de la TB era exiguo, pues en la mitad de las respuestas se atribuía la TB al consumo de un licor local. El 61% de quienes respondieron consideraba que la enfermedad era contagiosa y un tercio atribuía el modo transmisión al hecho de compartir los alimentos. Se observó un alto grado de conocimiento de la existencia de servicios de tratamiento sin costo en las instituciones públicas de salud, pero pocos conocían la estrategia DOTS. Se observaron diferencias notables entre los sexos en materia de conocimientos y sensibilización.
Conclusión: Los resultados del estudio destacan la urgencia de intensificar las actividades de promoción, comunicación y movilización social que sean culturalmente adaptadas y tomen en consideración las diferencias entre los sexos.
Nearly 2.0–2.5 million people develop tuberculosis (TB) each year in India, which accounts for 26% of the world's TB caseload.1 Every year, nearly 400 000 persons die due to TB. The Indian Government's Revised National TB Control Programme (RNTCP) takes overall responsibility for TB control and strives to ensure universal access to quality diagnosis and treatment facilities.2 The RNTCP's advocacy, communication and social mobilisation (ACSM) activities focus on sputum microscopy as the main diagnostic tool and the DOTS strategy, the globally recommended standard of TB care, to treat TB.2,3 While the RNTCP has achieved good levels of detection and cure, the government recognises the fact that marginalised and vulnerable populations, including tribal groups, face specific barriers to TB detection and treatment.4 The Tribal Action Plan developed in 2005 and the National Strategic Plan for 2012–2017 developed by the Government of India in partnership with the World Bank aim to tackle these barriers.4–6 Vulnerable populations and hard-to-reach areas are also listed as priorities under the operational research agenda.3
Despite these plans and policies, studies have highlighted the varied prevalence of TB among tribal populations.7,8 The RNTCP continues to face challenges in terms of case detection and treatment completion rates in difficult-to-reach areas.3,9 With the recent emphasis on ensuring universal access to TB services, these challenges are of critical importance, particularly in the hilly and remote tribal-dominant districts of India.
Few studies specifically documenting knowledge and awareness about TB among tribal communities have been published in recent years, and even fewer studies have clearly documented gender differences in TB knowledge and awareness levels among tribal communities.10 In the present paper, we look specifically at these issues among communities residing in tribal-dominant districts of the State of Jharkhand in India. Jharkhand, among the five Indian states that are lowest on the Human Development Index (HDI), is a predominantly tribal state11: 28% of the population in Jharkhand is tribal. The state is inhabited by 30 different tribal groups: Santhal, Munda, Ho, Oraons, Kharia and Bhumij are the major tribal communities.12 Records show that about 13 000 persons die of TB every year in Jharkhand.13 The RNTCP has identified East and West Singhbhum as difficult districts due to their low case detection rates and poor supervision.14 The Jharkhand Tribal Health Project (JTHP) is an intervention research project implemented by partners* in hard-to-reach areas of these two districts. It aims to understand the needs of the tribal population, document the underlying causes of low TB detection and suggest leads for interventions to improve the TB situation.
In this paper, we present findings from an operational research study on knowledge and awareness about TB among tribal communities residing in hilly, remote and Naxalite†-affected areas, conducted under the JTHP. The paper identifies specific issues to be addressed and measures to be undertaken to enhance the impact of TB ACSM activities in these districts.
STUDY POPULATION, DESIGN AND METHODS
A cross-sectional survey was carried out and data collection completed between September and October 2012 among the general population in 40 hard-to-reach tribal-dominant villages of the two study districts. The results of previous knowledge and awareness studies on TB in India were reviewed taking into consideration key areas of enquiry and indicators to be examined in the present study (LEPRA Health In Action, Maharashtra Association of Anthropological Sciences-Center for Health Research and Development. MP Baseline Situation Assessment Aarogya Project: Final Report. Unpublished).15–18 The review provided the expected value of proportion as 0.4. The formula for calculating sample size for proportions for large populations was used.19 One third of the tribal-dominant blocks were randomly selected; population proportionate sampling was used to calculate a sample size of 852 respondents from 20 villages in two blocks each from the West and East Singhbhum Districts. The 40 villages selected for the study were predominantly tribal, with a small proportion of non-tribal households. One adult person from each selected household was interviewed.
A semi-structured pre-tested interview schedule was used for data collection. The survey focused on documenting knowledge about TB symptoms, causes, modes of transmission, curability, diagnosis and treatment, as well as awareness about diagnosis and treatment available at government health centres and DOTS. Fifteen local field investigators, who were graduates and fluent in the local tribal languages, were trained in data collection in a week-long training programme. Two supervisors were trained and appointed to check data quality, and one of the authors was present at the time of data collection to ensure overall quality control.
Data recording and analysis
Data were entered into SPSS, version 16 (Statistical Package for the Social Sciences, Chicago, IL, USA). Descriptive statistics were initially performed to summarise data, and the data were categorised into knowledge and awareness indicators to calculate the scores for each category. Knowledge indicators were those providing biomedical information or facts about TB, whereas awareness indicators related to the availability of government TB services. Two indicators were common to both knowledge and awareness, and were thus considered as a separate category. The t-test was used to study association between knowledge and awareness indicators across sex. For all purposes, P < 0.05 (two-tailed) was considered as significant.
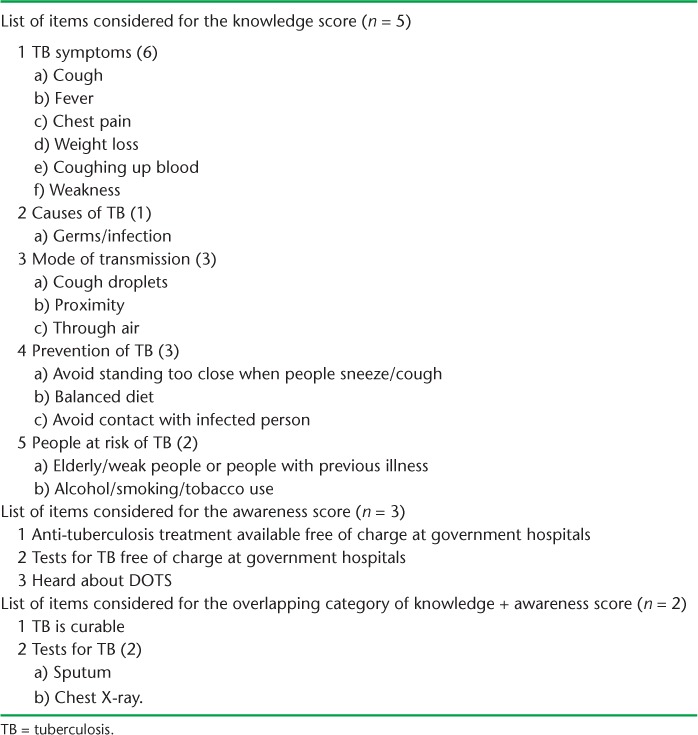
TB knowledge and awareness scores
The response options were ‘Yes,’ ‘No’ and ‘Don't know’ for knowledge and awareness items. Descriptive statistics were initially performed to summarise the data; thereafter, three new variables were created: ‘TB knowledge score’, ‘TB awareness score’ and ‘score for overlapping variables’. After testing correlation between indicators for each knowledge topic, 15 knowledge items were retained as valid (see Table 1) and included in the calculation of the knowledge score as follows: for each individual indicator, the correct answer was re-coded as ‘1’, and incorrect and ‘don't know’ answers as ‘0’. A single summary score for each knowledge topic was obtained by adding the number of correct responses and dividing the total by the number of variables in the topic. An aggregate measure was then computed, summing the values of each topic to obtain a knowledge score for each participant. The theoretical range of the knowledge score was 0–5, with higher scores indicating a higher level of knowledge. The average knowledge score for the group was obtained by summing each respondent's score and dividing it by the total number of respondents. Three awareness variables were retained as valid and included in the calculation of the awareness score; a 0–2 scale was used for the two overlapping indicators. The percentage of correct answers was calculated as representative of the score for each knowledge, awareness and overlapping category of indicators.
TABLE 1.
Items considered for knowledge, awareness and overlapping category scores
Ethical considerations
Written informed consent was provided by all study participants. For illiterate respondents, other literate family members or village-level health workers were asked to witness the reading out of the consent form and a thumb impression was taken from the respondents.
The study protocol was approved by the Institutional Ethics Committee of the Maharashtra Association of Anthropological Sciences (MAAS). Responses from interviews were noted down without names, and all data were anonymised during analysis for confidentiality.
RESULTS
Of the 852 respondents interviewed, 27 reported that either they or their family members had suffered from TB in the past 3 years. To avoid response bias, these 27 cases were excluded from further analysis, and the final sample consisted of 825 respondents.
Socio-demographic characteristics
More than half (n = 499, 61%) of the 825 respondents were in the 18–35 years age group (median age 33 years, interquartile range 25–45); 80% (n = 661) belonged to the Scheduled Tribes group and 85% of respondents were married. More than one third of the respondents (n = 365, 44%) were illiterate (Table 2).
TABLE 2.
Socio-demographic profile of respondents
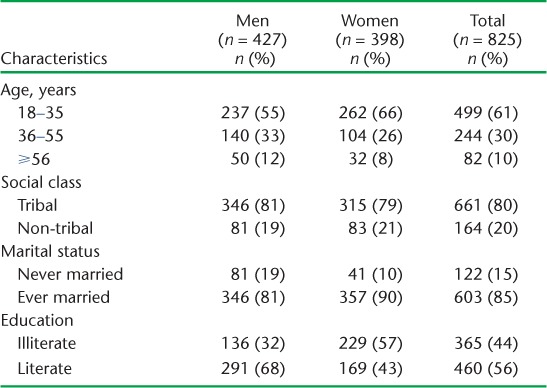
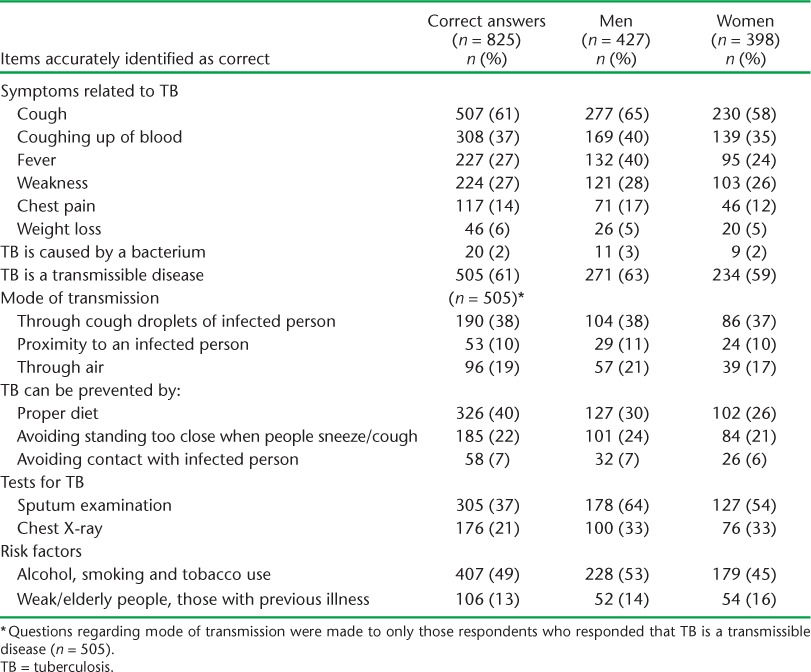
Table 3 shows the respondents' knowledge about TB. Cough was the most commonly reported symptom, followed by coughing up blood, fever and weakness; 2% of the respondents were able to report germs/infection as a cause of TB. Less than two thirds of the respondents (n = 505, 61%) considered TB to be transmissible. Proper diet was reported as a common way of preventing TB by 40% (n = 326) of the respondents. More than one third (n = 305, 37%) reported sputum examination as a test for diagnosing TB, while 21% (n = 176) mentioned chest X-ray. When asked about persons at greater risk for acquiring TB, nearly half of the respondents (n = 407, 49%) reported alcohol and tobacco addiction, while elderly or weak persons or those with a prior illness were reported by 11% (n = 92).
TABLE 3.
Knowledge about TB
Respondents' knowledge about TB in general was poor. The average knowledge score for the group was 0.98 ± 0.66, with a maximum of 5. Figure 1 shows the respondents' correct knowledge of five indicators. Respondents had poor knowledge about causes and ways of getting TB, but better knowledge about risk factors and symptoms.
FIGURE 1.
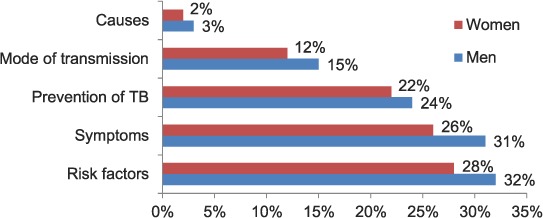
Proportion of maximal mean knowledge score (%) by topic as percentage of maximal score. TB = tuberculosis.
Half of the respondents (n = 416, 50%) reported local liquor (hadiya) consumption as a cause of TB, followed by tobacco and/or smoking. Less than two thirds of the respondents (n = 505, 61%) reported that TB was transmissible. More than one third of the respondents (n = 190, 38%) reported cough droplets as being responsible for TB transmission, 19% (n = 96) believed it was transmitted through air and 10% (n = 53) reported proximity with TB patients to be responsible. More than one third of the respondents (194/505, 38%) considered sharing food as a mode of TB transmission (data not presented in Table). Almost three quarters of the respondents (607/825, 74%) reported TB as a serious problem. When asked why they thought TB was a serious problem, less than half of the respondents (264/607, 43%) reported that it was because of its fatality, 17% (103/607) reported it was because of its infectious nature, while 13% (82/607) felt that if not treated properly or on time it could be serious.
The average awareness score for the group was 1.73 ± 0.85, with a maximum of 3. Respondents scored well on awareness indicators. Awareness about the availability of free TB diagnosis and treatment at government health centres was good; awareness about DOTS was, however, very poor (Figure 2).
FIGURE 2.
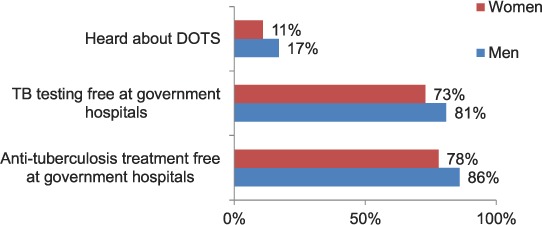
Proportion of maximal mean awareness score (%) by topic as percentage of maximal score. TB = tuberculosis.
The mean score for overlapping indicators was 1.14 ± 0.54, with a maximum of 2. Respondents were well aware about TB being curable but had a low level of knowledge about the tests for TB (Figure 3).
FIGURE 3.
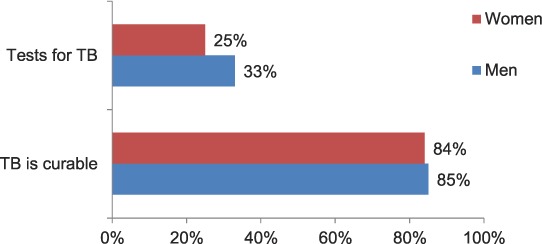
Proportion of maximal mean score overlapping indicators (%) by topic as percentage of maximal score. TB = tuberculosis.
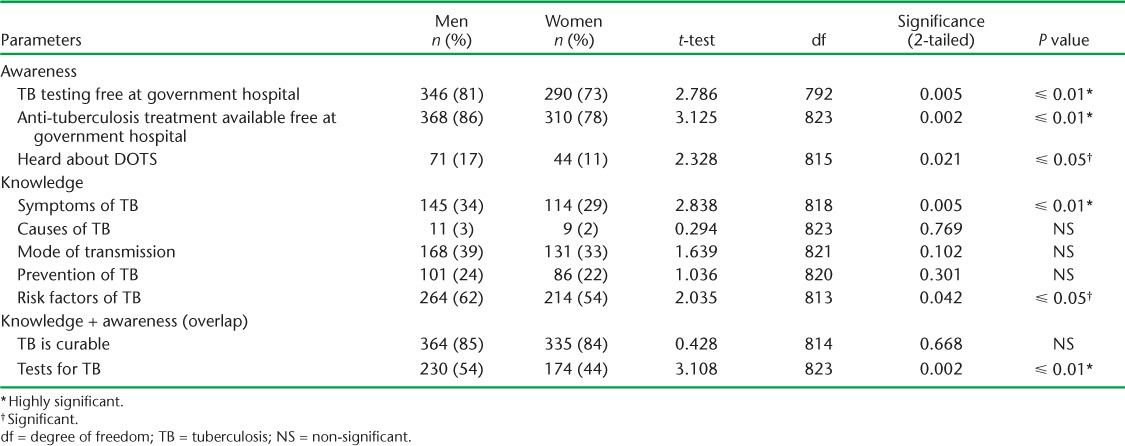
Table 4 shows gender differences in knowledge and awareness. The t-test results suggest that there is a significant difference in awareness about free anti-tuberculosis treatment, diagnosis, DOTS, TB testing, symptoms and risk factors; fewer women than men were aware of these.
TABLE 4.
Gender differences across knowledge and awareness indicators
DISCUSSION
The study findings indicate poor TB-related knowledge and moderate awareness among the general population residing in tribal-dominant study districts. Similar findings have been reported by studies conducted in other tribal districts of India.10,18,20 While cough was the most commonly reported symptom, there was no specific mention of cough of >2 weeks by respondents, which the programme has been trying to promote through ACSM interventions to ensure early detection. Correct knowledge about the causes of TB among respondents was negligible, and their concepts about causes could be attributed to the community's experiences of people consuming liquor or smoking or using tobacco as those most commonly affected by TB. This is also reflected in their understanding about risk factors, and is in line with study findings among the tribal population of Madhya Pradesh, India.10 The causes of TB reported by respondents were local liquor and smoking, while reported modes of transmission were cough droplets, proximity to an infected person and through the air, indicating a logical disconnect between perceptions regarding causes and modes of transmission. The finding of poor knowledge but higher levels of awareness about TB among this population could be explained as follows: respondents were aware about the availability of free TB diagnosis and treatment at government facilities, but were unaware about DOTS.
Sputum smear microscopy as the main diagnostic tool, the availability of free diagnosis and treatment, DOTS and the curable nature of TB are the main programme messages being emphasised by the RNTCP through its ACSM activities. However, only a third of the respondents in our study reported sputum examination as a diagnostic test for TB and little more than 10% reported awareness of DOTS. These findings indicate less penetration of RNTCP communication activities in the study districts. The National Strategic Plan recommends bridging the gap between traditional and biomedical knowledge among marginalised and vulnerable groups.4 The present study concurs with this recommendation and emphasises the need to undertake community mobilisation to address culture-specific notions, concepts and misbeliefs regarding TB. The TB knowledge and awareness indicators documented in this study would be helpful in ensuring community mobilisation and in strategic planning of ACSM activities.
A little less than half of the respondents, including a higher proportion of women, were illiterate. The direct relationship between literacy and knowledge levels has been documented in various studies on TB in India and Africa.20,21 This suggests a need for the creation of IEC (information, education and communication) material in tribal languages with more audiovisual and pictorial presentations to explain symptoms, the importance of early diagnosis, the effectiveness of DOTS, etc., which will in turn enable early detection and treatment of TB.
The study also showed gender differences: women were found to have lower levels of knowledge and awareness about TB than men. This finding is similar to other studies from India.16,20 The WHO ACSM framework for action acknowledges that the majority of people affected by TB face substantial problems in accessing treatment even when treatment facilities exist and mentions gender inequality as one of the main problems to accessing TB services.22–24 The gender-related findings from this study are in consonance with this, and the gender inequality reflected in lower levels of literacy, limited exposure to the outside world and low priority attributed to their own health, adversely affected knowledge and awareness levels among women respondents in tribal-dominant districts.
India's 12th Five-Year Plan document has identified and emphasised the need to increase awareness on health-related matters among women and deprived populations living in inaccessible areas.25 In accordance with this, the Government of India has approved the reservation of 50% of posts for women in Panchayati Raj institutions (local administrative bodies).26 Our study findings suggest there is a need to build on such initiatives and initiate strategies that can go beyond educating female community members and incorporate female empowerment measures to bring about sustainable change in knowledge and awareness levels, and subsequent health-seeking behaviour.21
CONCLUSION
The lower TB knowledge and awareness levels documented in this study underline the importance of urgent intensification of culturally congruent and gender-sensitive ACSM activities in hilly and remote tribal-dominant districts of India.
Acknowledgments
This study was funded by the BIG Lottery Fund, UK (The Jharkhand Tribal Health Project: unique reference number: ICB/2/010424145). The authors would like to thank the general community respondents of the study area; Alternative for India Development (AID India, Jamshedpur) project manager, district coordinators and fieldworkers; all administrative and project staff at Maharashtra Association of Anthropological Sciences-Center for Health Research and Development, AID India and Target TB; and U Mahajan, Pune, India, for statistical input.
Footnotes
Conflict of interest: none declared.
Alternative for India Development (Jamshedpur), Maharashtra Association of Anthropological Sciences - Centre for Health Research Development (Pune, India) and Target TB UK, Brighton, with funding from the Big Lottery Fund, London, UK.
Generic term used to refer to various Communist guerrilla groups in India.
References
- 1.World Health Organization. Global tuberculosis report 2012. Geneva, Switzerland: WHO; 2012. WHO/HTM/TB/2012.6. http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf Accessed August 2014. [Google Scholar]
- 2.Central TB Division. TB India 2012: Revised National TB Control Programme. Annual Status Report. New Delhi, India: Central TB Division, Ministry of Health & Family Welfare; 2012. tbcindia.nic.in/pdfs/TB%20India%202012-%20Annual%20Report.pdf Accessed August 2014. [Google Scholar]
- 3.Central TB Division. TB India 2013: Revised National TB Control Programme. Annual Status Report. New Delhi, India: Central TB Division, Ministry of Health & Family Welfare; 2013. www.tbcindia.nic.in/pdfs/TB%20India%202013.pdf Accessed August 2014. [Google Scholar]
- 4.Central TB Division, Department of General of Health Services. Social Action Plan 2013. RNTCP. New Delhi, India: Central TB Division; 2013. http://tbcindia.nic.in/pdfs/Social%20Action%20Plan%202013%20Final.pdf Accessed August 2014. [Google Scholar]
- 5.Kamineni V V, Wilson N, Das A et al. Addressing poverty through disease control programmes: examples from Tuberculosis control in India. Int J Equity Health. 2012;11:17. doi: 10.1186/1475-9276-11-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Central TB Division, Directorate General of Health Services, Ministry of Health & Family Welfare. RNTCP Tribal Action Plan 2005. New Delhi, India: Central TB Division; 2005. http://www.wds.worldbank.org/servlet/WDSContentServer/WDSP/IB/2005/05/10/000011823_20050510172009/Rendered/PDF/IPP127.pdf Accessed August 2014. [Google Scholar]
- 7.Narang P, Tyagi N K, Mendiratta D K, Jajoo U N, Bharambhe M S, Nayar S. Prevalence of sputum-positive pulmonary tuberculosis in tribal and non-tribal populations of the Ashti and Karanja tahsils in Wardha District, Maharashtra State, India. Int J Tuberc Lung Dis. 1999;3:478–482. [PubMed] [Google Scholar]
- 8.Datta M, Radhamani M P, Sadacharam K et al. Survey for tuberculosis in a tribal population in North Arcot District. Int J Tuberc Lung Dis. 2001;5:240–249. [PubMed] [Google Scholar]
- 9.Central TB Division. TB India 2006. New Delhi, India: Central TB Division; 2006. http://tbcindia.nic.in/pdfs/TB%20India%202006.pdf Accessed August 2014. [Google Scholar]
- 10.Rao V G, Yadav R, Bhat J, Tiwari B K, Bhondeley M K. Knowledge and attitude towards tuberculosis amongst the tribal population of Jhabua, Madhya Pradesh. Indian J Tuberc. 2012;59:243–248. [PubMed] [Google Scholar]
- 11.United Nations Development Programme. Jharkhand: economic and development indicators. New York NY, USA: UNDP; 2011. http://www.undp.org/content/dam/india/docs/jharkhand_factsheet.pdf Accessed August 2014. [Google Scholar]
- 12.Water Supply & Sanitation Department, Government of Jharkhand, Jharkhand Rural Water Supply and Sanitation Project. The World Bank-assisted Jharkhand Tribal Development Plan. IPE Global; 2013. http://112.133.209.136:8000/dwsd/Documents/World%20Bank/Tribal_Development_Plan.pdf Accessed August 2014. [Google Scholar]
- 13.The Telegraph Calcutta. Jharkhand: State prods industry to fight TB. Kolkata, India: The Telegraph; 2014. 23 May 2014. http://www.telegraphindia.com/1100707/jsp/jharkhand/story_12654542.jsp Accessed August 2014. [Google Scholar]
- 14.National Rural Health Mission Jharkhand. National Disease Control Programme Jharkhand. Ranchi, India: NHRM; 2011. http://pipnrhm-mohfw.nic.in/index_files/high_focus_non_ne/Jharkhand/Part%20D-National%20Programmes.pdf Accessed August 2014. [Google Scholar]
- 15.Yadav S P, Mathur M L, Dixit A K. Knowledge and attitude towards tuberculosis among sandstone quarry workers in desert parts of Rajasthan. Nakhon Pathom, Thailand: Index Medicus for South-East Asia Region; 2006. http://imsear.hellis.org/handle/123456789/146930 Accessed August 2014. [Google Scholar]
- 16.Maharashtra Association of Anthropological Sciences-Centre for Health Research Development. Generating evidence base to help implement India-specific TB-ACSM strategies. Pune, India: MAAS-CHRD; http://maas.org.in/images/pdf/TB-ACSM-dissemination-flier.pdf Accessed August 2014. [Google Scholar]
- 17.Devey J. Report on a knowledge, attitude and practice (KAP) survey regarding tuberculosis conducted in Northern Bihar. Human Needs and Global Resources Internship Independent Study. Raxaul, India: HNGR; 2000. http://www.eha-health.org/resources/downloads.html?task=document.viewdoc&id=118 Accessed August 2014. [Google Scholar]
- 18.Swamy R K. Baseline KAP study under RNTCP Project. New Delhi, India: Central TB Division, Government of India; 2003. http://tbcindia.nic.in/pdfs/Baseline%20KAP%20Study%20under%20RNTCP%20Project%20-%20CMS.pdf Accessed August 2014. [Google Scholar]
- 19.Israel G D. Determining sample size. University of Florida Cooperative Extension Service, Institute of Food and Agriculture Sciences, Electronic Data Information Source; 1992. http://www.soc.uoc.gr/socmedia/papageo/metaptyxiakoi/sample_size/samplesize1.pdf Accessed August 2014. [Google Scholar]
- 20.Sreeramareddy C T, Kumar H H, Arokiasamy J T. Prevalence of self-reported tuberculosis, knowledge about tuberculosis transmission and its determinants among adults in India: results from a nation-wide cross-sectional household survey. BMC Infect Dis. 2013;13:16. doi: 10.1186/1471-2334-13-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tobin E A, Okojie P W, Isah E C. Community knowledge and attitude to pulmonary tuberculosis in rural Edo state, Nigeria. Ann Afr Med. 2013;12:148. doi: 10.4103/1596-3519.117623. [DOI] [PubMed] [Google Scholar]
- 22.Stop TB Partnership, World Health Organization. Advocacy, communication and social mobilization to fight TB: a 10-year framework for action. Geneva, Switzerland: WHO; 2006. [Google Scholar]
- 23.Weiss M G, Auer C, Somma D Gender and tuberculosis: cross-site analysis and implications of a multi-country study in Bangladesh, India, Malawi and Colombia. Geneva, Switzerland: World Health Organization; 2006. TDR/SDR/SEB/RP/06.1. http://cdrwww.who.int/entity/tdr/publications/documents/sebrep3.pdf Accessed August 2014. [Google Scholar]
- 24.Morankar S, Weiss M G. Impact of gender on illness experience and behaviour: implications for tuberculosis control in rural Maharashtra. Health Adm. 2003;15:149–155. [Google Scholar]
- 25.Planning Commission Government of India. 12th Five-Year Plan 2012–2017. (Social Sectors) New Delhi, India: Sage Publications; 2013. planningcommission.gov.in/plans/planrel/12thplan/pdf/12fyp_vol3.pdf Accessed August 2014. [Google Scholar]
- 26.Press Information Bureau. Women reservation in Panchayat. New Delhi, India: PIB; 2011. http://www.pib.nic.in/newsite/erelease.aspx?relid=74501 Accessed August 2014. [Google Scholar]