
Figure 5.
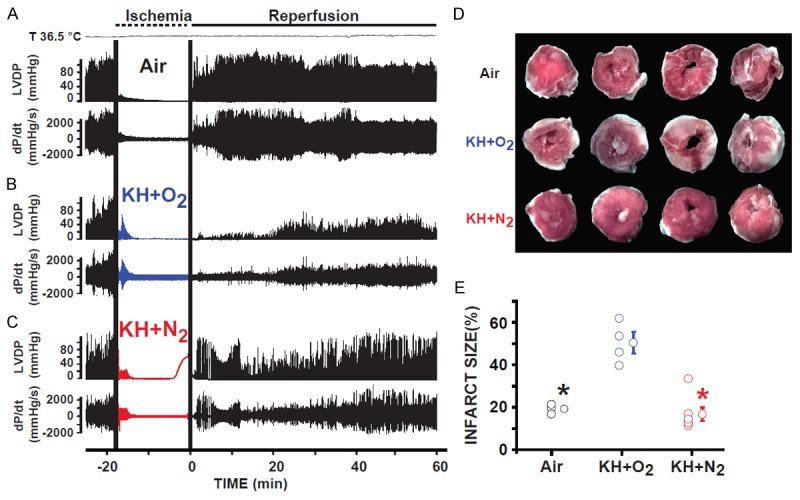
Hearts immersed in KH+N2 had improved recovery of function and reduced myocardial infarct size when compared to hearts immersed in (KH+O2 during the normothermic ischemic period. Recordings of ventricular-developed pressure (LVDP) and velocity of contraction and relaxation (dP/dt) in hearts suspended in air (A), immersed in KH+N2 (B), and immersed in KH+O2 (C) during the ischemic period and reperfused for 60 minutes. Note that the recovery of cardiac function was much greater in the groups of hearts immersed in KH+N2 than in hearts immersed in KH+O2 during the ischemic period. (D), Images of 4 slices of different regions from the same heart suspended in air, immersed in KH+N2, or immersed in KH+O2 during the ischemic period; hearts were obtained at the end of 60 minutes of reperfusion. (E) Bar graph showing the individual percentage of myocardial infarct size in the three conditions of ischemic conservation. The myocardial infarct size was much smaller in the groups of hearts suspended in air than in hearts immersed in KH+O2 during the ischemic period. The myocardial infarct size significantly decreased when hearts were immersed in KH+N2 when compared to hearts immersed in KH+O2. Values are expressed as mean ± SEM.; *P<0.05 hearts immersed in KH+O2 versus hearts maintained in air during ischemia; +P<0.05 hearts immersed in KH+O2 versus hearts immersed in KH+N2 during ischemia (n = 4-5/group).