
Figure 1. Association between Paroxysmal versus Persistent Atrial Fibrillation Classification and Likelihood of Antithrombotic Prescription in Patients with a Moderate to High Risk of Stroke (CHADS2 Score ≥2).
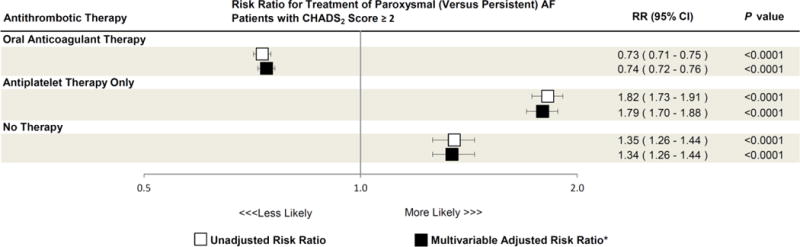
Unadjusted (white boxes) and multivariable adjusted (black boxes) risk ratios of oral anticoagulant therapy, antiplatelet only therapy, and no therapy prescription in paroxysmal versus persistent atrial fibrillation (AF) patients are shown. Error bars denote 95% confidence intervals.
Oral anticoagulant therapy was defined as prescription of either warfarin, dabigatran, or rivaroxaban. Antiplatelet therapy was defined as prescription of either individual or combination of aspirin, clopidogrel, ticlopidine, prasugrel, and/or dipyridamole.
CI = confidence interval; RR = risk ratio.
*Adjusted for age, sex, region, insurance, body mass index (BMI), CHADS2 score, congestive heart failure, hypertension, diabetes, prior stroke/transient ischemic attack, systemic embolism, coronary artery disease, prior myocardial infarction, recent coronary artery bypass grafting or percutaneous coronary intervention, stable angina, peripheral arterial disease, dyslipidemia, and tobacco use.