
Fig. 6.
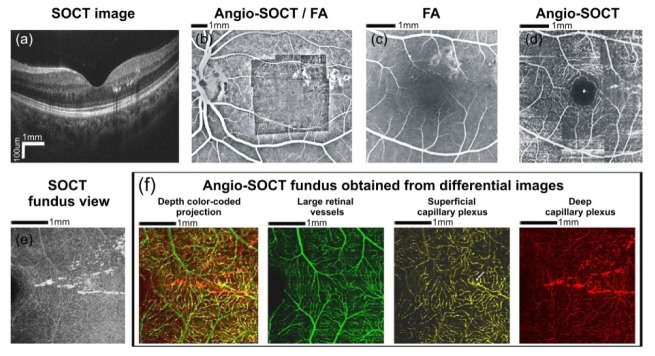
Data obtained from a 37 year-old patient with diabetic retinopathy. Visual acuity in the left eye was 20/25. (a) OCT cross-sectional image (protocol C). Hard exudates are visible in the temporal macula. (b) The automatically generated angio-OCT mosaic projected onto the fluorescein angiography image (protocol B). (c) Fluorescein angiography showing few microaneurysms. The capillary network pattern above and temporally from the fovea is obscured by the hyperfluorescence of laser scars. Hard exudates are not visible in FA image. (d) AID angio-OCT mosaic of the fundus area shown in Fig. 6(c). Laser scars do not obscure retinal vasculature as angio-OCT scans do not include RPE-generated signal. Few microaneurysms and several hard exudates are visible within temporal macula. The white punctate spot in the center corresponds to foveal reflex. Angio-OCT imaging region - 4.5 x 4.5 mm. (e) OCT fundus view of temporal macula with the hard exudates (protocol A).(f) Color-coded angio-OCT fundus views showing retinal vasculature at different levels (layers) within the temporal macula (protocol A). Large retinal vessels were coded green, the superficial capillary plexus was coded yellow and the deep capillary plexus was coded red. It is clearly visible that most hard exudates are located within the deep capillary plexus. Superficial capillary plexus is the source of hard exudates at a single site only (arrow). Angio-OCT imaging region - 3.1 x 3.1 mm.