

Abstract
We reviewed the underlying principles that allow for safe and effective ablation for premature ventricular complexes. Clinical scenarios that necessitate consideration for ablation, the underlying anatomy, and the unique consideration to maximize energy delivery without compromising safety are sequentially examined.
Keywords: premature ventricular complexes, ablation, anatomy, safety, outflow tract

A. Noheria, M.B.B.S., S.M.
Introduction
Premature ventricular complexes (PVCs) occur fairly commonly in the general population and are more frequent in patients with hypertension, obesity, sleep apnea, and structural heart disease. In general, occasional PVCs in the structurally normal heart are considered benign,1 though they have been associated with a more than two-fold higher risk of cardiovascular outcomes including stroke2 and mortality.3 PVCs commonly arise from the right ventricular (RV) outflow tract (RVOT) and sometimes the left ventricular (LV) outflow tract (LVOT).4 Other sites for PVCs include the His-Purkinje system, especially the left posterior fascicle (predominantly in young males); endocavitary structures including the papillary muscles, moderator band, and false tendons5; and the annuli of the aortic, pulmonary, and both atrioventricular (AV) valves.6,7 In the case of structural heart disease, PVCs can originate from reentry in the presence of unidirectional block and slow conduction through electrically viable tissue within areas of scar.8 An implanted defibrillator lead, inflow cannula of a LV assist device, or interaction between the papillary muscles in mitral valve prolapse9 can cause stretch, mechanical irritation, and fibrosis that result in PVCs.
Mechanism of PVCs
Benign outflow tract PVCs are thought to originate from tissue embryologically derived from remnant dead-end conduction tissue.4,10 Further, 1 in 10 patients with RVOT PVCs will have clinical or inducible AV nodal reentrant tachycardia.11 Mechanistically, it has been proposed that RVOT PVCs are caused by delayed after depolarizations or triggered automaticity, provoked by catecholamines, exercise, and menstrual cycles, and inhibited by adenosine.4,12–14 However, anisotropic extensions of cardiomyocytes above the fibrous valvular annuli have also been hypothesized to allow conduction slowing and unidirectional block, which can lead to reentrant PVCs.4,15–17 Delayed after depolarizations also cause pathologic PVCs, frequently in a bigeminal pattern, in channelopathies such as Andersen-Tawil syndrome or catecholaminergic polymorphic ventricular tachycardia (VT), and in digoxin toxicity. On the other hand, early after depolarizations may cause PVCs that are precursors for torsades de pointes in long QT syndromes and drug-related QT prolongation. Reentry is the likely mechanism for PVCs originating from regions of fibrosis or infiltration in cardiomyopathies such as ischemic heart disease, arrhythmogenic RV cardiomyopathy, sarcoidosis, Chagas disease, hypertrophic cardiomyopathies, primary dilated cardiomyopathies, valvular cardiomyopathy, congenital heart disease, muscular dystrophies (e.g., myotonic dystrophy, Emery-Dreifuss muscular dystrophy), and metabolic disorders such as Fabry disease, Pompe disease, Danon disease, and mitochondrial diseases. PVCs can originate due to reentry around surgical scars. Fascicular PVCs are due to small reentry circuits involving the fascicles18,19 or to triggered or enhanced automaticity.20
Electrocardiogram Features
The electrocardiogram (ECG) is the basic tool to predict the presence of scar from prior myocardial infarction or cardiomyopathy. ECGs in classic arrhythmogenic RV cardiomyopathy have QRS duration > 100 ms with terminal QRS notching or epsilon wave and T-wave inversions in right precordial leads. Cardiac sarcoidosis, myotonic dystrophy, and dilated cardiomyopathy related to LMNA mutations have a predilection for conduction system abnormalities. In some patients, ECGs can suggest the presence of RV hypertrophy and conduction delay, for example, in those with mitral stenosis and congenital heart disease such as atrial septal defect, Ebstein's anomaly, repaired Tetralogy of Fallot with pulmonic stenosis, ventricular septal defect, AV canal defect, and AV switch with Senning or Mustard procedures in d-transposition of the great arteries. Congenitally corrected transposition presents with Q-waves in right precordial leads and the absence of septal Q-waves in lateral leads.
PVC Localization with ECG
A point source origin of ventricular activation has a characteristic QRS pattern on ECG as the electrical wavefront traverses the contiguous myocardium and tracks around anatomic boundaries to activate both the ventricles in a predictable manner. Thus, the QRS morphology on ECG can predict the PVC's site of origin or exit to the larger myocardial mass (Table 1).13 The site of origin or earliest activation is the target of ablation for focal PVCs; for reentrant PVCs, the critical arrhythmogenic tissue can often be targeted in proximity to the exit site. Outflow tract PVCs typically have an inferior frontal plane axis with tall positive R waves in inferior leads (II, III, aVF) and QS complexes in aVR and aVL.4 Positive or negative QRS polarity in lead I can help localize PVCs to the right versus left parts of the outflow tracts. PVCs originating in the para-Hisian region close to the RV inflow are positive in leads I and aVL, whereas lead I is negative with leftward origin above the pulmonary valve or left coronary cusp. PVCs originating anteriorly from the free wall of the RVOT are wider compared to those from the septum and have left bundle branch block (BBB) morphology (QS in lead V1 with precordial R/S transition ≥ V3). Lead V1 starts to show R waves with PVCs originating further cephalad and leftwards close to the pulmonary valve, or posteriorly from the septum or adjacent locations in the LVOT including the right coronary cusp. PVCs from progressively posterior locations of the left coronary cusp, the noncoronary cusp, and aortomitral continuity (qR in V1) have progressively taller R waves in V1, and PVCs from the mitral annulus have a completely positive R wave in V1 (Figure 1). LVOT PVCs typically have an earlier precordial R/S transition (≤ V3) compared to RVOT PVCs.21 PVCs originating from epicardial sites have a pseudo-delta wave, with slurring of the initial part of the QRS complex and delayed intrinsicoid deflection in the precordial leads, and can often be accessed through epicardial veins close to the great cardiac vein-anterior interventricular vein (GCV-AIV) junction.22,23
Table 1.
Summary of electrocardiographic features that suggest particular region as site of origin/exit of premature ventricular complexes.
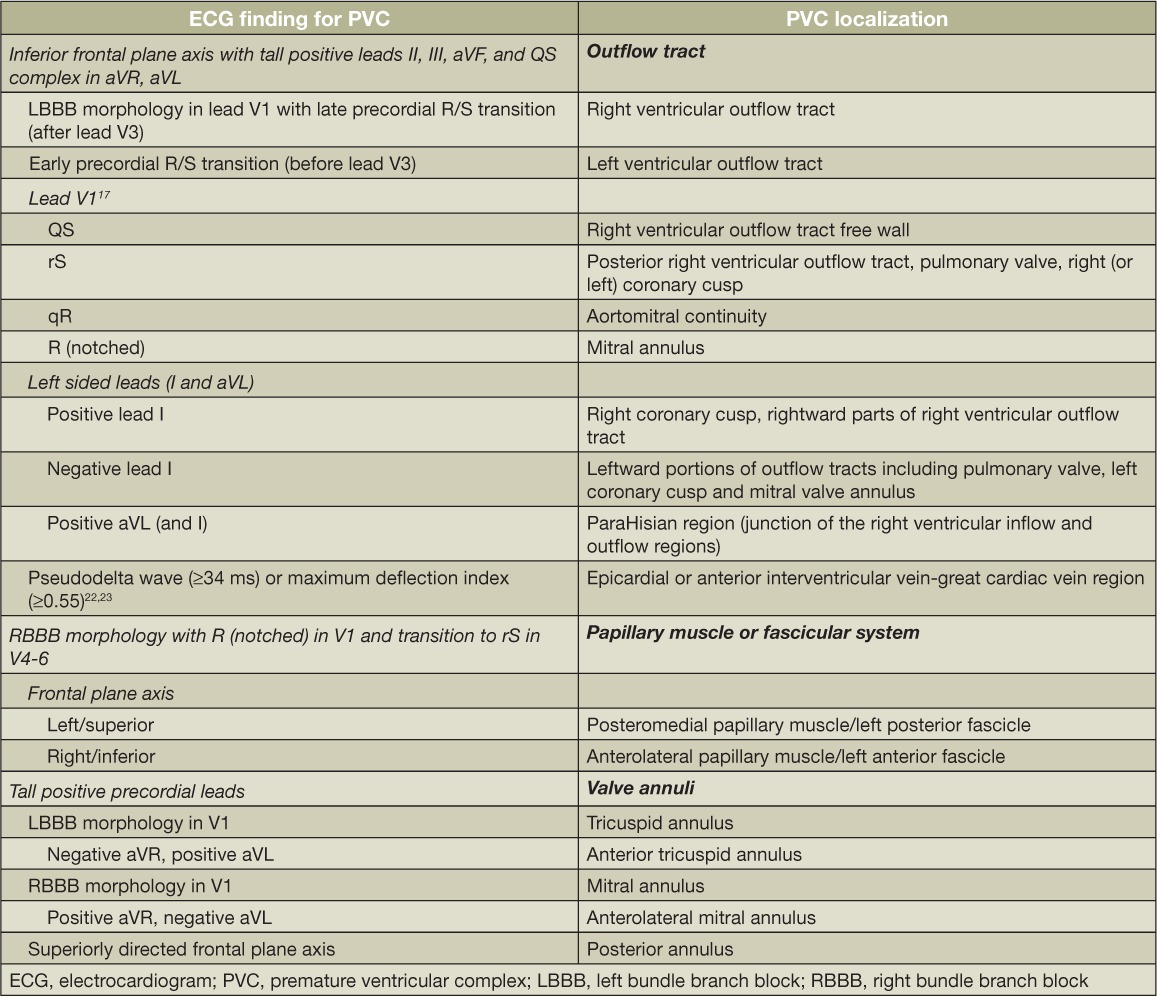
Figure 1.
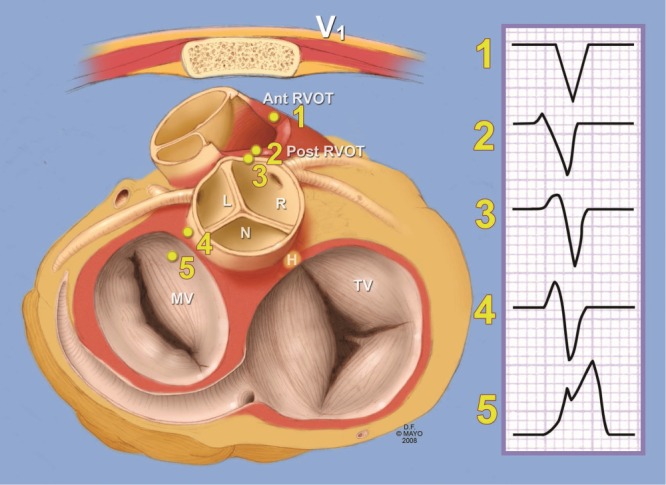
Illustration showing the regional anatomy of the base of the heart and the cardiac valves in relation to the sternum and location of electrocardiographic chest lead V1, as viewed from the atrial aspect. Also shown is the expected polarity of the PVC morphology in lead V1, with an entirely negative vector for RVOT free wall PVC with progressively larger R wave and the PVC site is sequentially more posterior in the heart. Note that the region above the pulmonary valve (pulmonary artery) is on left of the body. Ant, anterior; post, posterior; RVOT, right ventricular outflow tract; R, right coronary cusp; L, left coronary cusp; N, non-coronary cusp; H, His bundle; MV, mitral valve; TV, tricuspid valve. Used with permission of Mayo Foundation for Medical Education and Research, from Tabatabaei N, Asirvatham SJ. Supravalvular arrhythmia: identifying and ablating the substrate. Arrhythmia and electrophysiology. Circulation. 2009;2(3):316–326. All rights reserved.
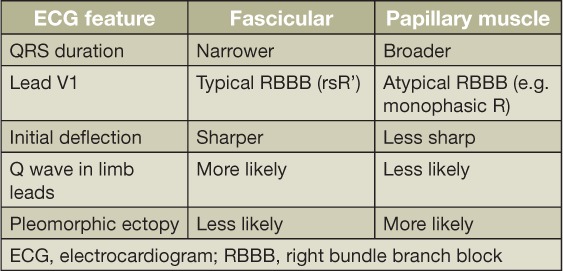
PVCs originating from the fascicular system have a relatively narrow QRS with a sharp initial deflection as the Purkinje system is engaged. PVCs originating in the left posterior fascicle have a typical right BBB morphology with superior frontal plane axis, while PVCs from the anterior fascicle have a rightward axis.18,19 PVCs originating from the LV posterior and anterior papillary muscles are similar to the respective fascicular PVCs. However, papillary muscle PVCs lack the typical rsR' in V1, and Q waves in limb leads have a less sharp QRS onset, an overall longer QRS duration, and pleomorphic PVC morphologies due to multiple exit sites (Table 2).24,25 PVCs originating from moderator band or false tendons can have two disparate morphologies or axes as the ectopy exits from the two separate attachments.5
Table 2.
Electrocardiographic features suggesting fascicular versus papillary muscle origin/exit of premature ventricular complexes.24,25
PVC Coupling Interval
The coupling interval of PVCs to the previous QRS complex can provide mechanistic and prognostic information. A stable coupling interval of PVCs that shortens with increased sympathetic tone and prolongs or suppresses PVCs with parasympathetic drive suggests triggered automaticity.14 A variable coupling interval might be related to variability in conduction across the fibrous annuli related to reentrant PVCs targeted near the semilunar valves or at the GCV-AIV junction,26 although reentrant PVCs can certainly occur with a fixed coupling interval. As opposed to relatively benign long-coupled PVCs, short-coupled PVCs can induce rapid and unstable ventricular tachyarrhythmias.27,28
Additional Testing
Holter monitoring is useful to identify the various morphologies of PVCs, their relative burden, diurnal variations, and coupling intervals, though these can vary on a day-to-day basis. A signal-averaged ECG might suggest underlying cardiomyopathy and aid diagnosis of conditions such as arrhythmogenic RV cardiomyopathy. Testing with coronary angiography, cardiac magnetic resonance imaging, and endomyocardial biopsy can help diagnose various cardiomyopathies. Exercise testing tends to provoke “triggered” outflow tract or fascicular PVCs and “mechanically stimulated” papillary muscle PVCs in mitral valve prolapse, but it might suppress long-coupled reentrant PVCs as the sinus rate accelerates.
Justification for Ablation of PVCs
Symptomatic Arrhythmia and Cardiac Arrest
Though PVCs are fairly infrequent and asymptomatic in most cases, in some patients they may be more frequent and cause symptoms including palpitations, chest pain, and dyspnea. The spectrum of “benign” outflow tract PVCs ranges from single PVCs to repetitive nonsustained VT to paroxysmal sustained VT.29 In rare cases, short-coupled RVOT PVCs can trigger polymorphic VT,27 while even shorter-coupled PVCs often originating from the fascicular system or papillary muscles can trigger ventricular fibrillation.20,28 PVCs in severe bileaflet mitral valve prolapse have been shown to be antecedents of malignant ventricular tachyarrhythmia.9 PVCs are the frequent trigger for reentrant VT in patients with structural heart disease. PVC suppression with catheter ablation becomes necessary in such situations to prevent recurrent sudden cardiac arrest and implantable cardioverter defibrillator shocks.
PVC-Mediated Cardiomyopathy
PVCs have increasingly been recognized as a primary cause for worsening LV systolic function and heart failure in some patients once obvious causes like cardiac ischemia, valvular disease, toxic-metabolic or infiltrative diseases, and persistent tachycardia have been excluded. In addition to the underlying cardiac structural abnormalities, predictors for development of PVC-mediated cardiomyopathy include patient factors (obesity,30 absence of palpitations31) and PVC characteristics (burden > 20%, left BBB morphology, wide QRS, large variability in the coupling interval, PVCs interpolated between consecutive sinus beats32).30,33,34 Despite such clinical associations, it is often unclear at presentation if the PVCs are a cause or the result of an otherwise idiopathic cardiomyopathy or contributing to decline in LV function in a patient with underlying structural heart disease. The pathogenesis of PVC-mediated cardiomyopathy is uncertain, and hypotheses include ventricular dyssynchrony, hemodynamic impairment, increased oxygen demand, autonomic dysregulation, alterations in intracellular calcium handling, and altered heart rate dynamics.13,33 In a canine model of LV dysfunction induced with RV pacing, there was no evidence of myocardial histopathologic findings such as inflammation, fibrosis, mitochondrial abnormalities, or accelerated apoptosis.35 PVCs increased dispersion of action potential duration due to heterogeneous reduction in Ito, IK1 and ICaL and caused abnormalities in myocardial calcium handling.36
Suppression of PVCs with ablation is often required to potentially reverse the cardiomyopathy. PVCs are culpable in preventing recovery of LV dysfunction in patients with ventricular conduction abnormalities treated with cardiac resynchronization therapy (CRT). Reduction in delivery of true biventricular pacing with CRT to < 90% due to any reason, including a high burden of PVCs, is associated with a lack of improvement in LV systolic function.37
Ablation versus Medical Therapy
Medications can be used to suppress PVCs and are often employed as the first-line option. Drug selection is often based on the underlying cause and mechanism of PVCs, and the potential for adverse events. Outflow tract PVCs tend to respond to beta-blockers and calcium channel-blockers.33 Idiopathic fascicular PVCs are particularly sensitive to verapamil. Rarely, sotalol or amiodarone may be required for idiopathic outflow tract or fascicular PVCs. Sodium channel-blockers (class I antiarrhythmics) flecainide and mexiletine can inhibit PVCs triggered by delayed after depolarizations. Reentrant PVCs are suppressed with class III antiarrhythmics including sotalol, dofetilide, and amiodarone, though class I agents also have a complementary role. Medical therapy is, however, limited by lack of efficacy for many patients. Additionally, beta-blockers, calcium channel-blockers, and sodium channel-blockers might cause unacceptable adverse effects such as fatigue or reduced ventricular inotropy and are difficult to take regularly on a long-term basis. Furthermore, class I (e.g., flecainide) and class III (e.g., sotalol and dofetilide) antiarrhythmic drugs have the risk of life-threatening proarrhythmia. In light of these shortcomings, patients may choose to pursue catheter ablation of PVCs implicated in causing symptoms, ventricular tachyarrhythmia, or cardiomyopathy.38,39
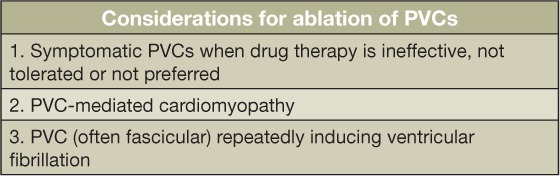
According to the American College of Cardiology/American Heart Association/European Society of Cardiology 2006 Guidelines, PVC ablation is reasonable (Class IIa) for symptomatic PVCs when drug therapy is ineffective, not tolerated, or not preferred by the patient. PVC ablation may also be considered (Class IIb) to treat or prevent PVC-mediated cardiomyopathy or for fascicular system PVCs that reproducibly induce ventricular fibrillation (Table 3).40
Table 3.
Most common justifications for management of premature ventricular complexes (PVCs) with catheter ablation.40
Techniques for PVC Ablation
Planning the Procedure
Prior to bringing the patient to the electrophysiology laboratory, a careful evaluation and discussion of the justification and risks of ablation is required. Mapping and ablation strategy has to be individualized based on patient, anatomic, and mechanistic considerations, and a review of the ECG, Holter monitor, and imaging data helps to plan the procedure. Triggered PVCs are exquisitely catecholamine sensitive and can be completely inhibited with anesthesia; therefore, general anesthesia should be avoided at the outset if possible. Opiates and benzodiazepines should be avoided. Anesthetic agents with rapid onset and offset kinetics such as ketamine or propofol are preferable, and if inhalational anesthesia is required, nitrous oxide is preferable to fluranes. Sympathomimetic agents (isoproterenol or epinephrine), methylated xanthines (aminophylline or caffeine), or awakening the patient on the table may provoke PVCs. Rapid atrial or ventricular pacing causes an increase in triggered PVCs. In some instances, high-frequency electrical stimulation (50 ms train) in the proximal main or left pulmonary artery can induce outflow tract PVCs.41,42 On the other hand, atrial or ventricular extrastimulation may provoke reentrant PVCs.
Procedural Imaging
As opposed to sustained VT, entrainment of single PVCs is not possible, and mapping of both focal and reentrant PVCs is largely dependent on activation mapping. Electroanatomic mapping systems can be helpful, especially when multiple chambers need to be mapped and compared. Fluoroscopy is the mainstay to visualize catheters, and a biplane system with orthogonal left anterior oblique and right anterior oblique views is ideal. Contrast evaluation of the venous system, pericardial space, and coronary arteries may assist in understanding the regional anatomy. Intracardiac echocardiography (ICE) can be valuable in assessing catheter contact and lesion formation during energy delivery, especially when ablating around valves or endocavitary structures, and it also allows prevention and early identification of complications like pericardial effusion, valvular injury, or thrombus formation.
Activation Mapping
Similar to ECG localization, the goal of PVC activation mapping is to identify the earliest site of activation, albeit with a more precise and accurate localization using the mapping catheter. Activation mapping is ideal for focal PVCs and is done with point-by-point mapping if PVC frequency is adequate (Figure 2).13 Alternatively, with a multielectrode catheter, multiple points can be acquired in a single beat when the PVC is very infrequent (e.g., PentaRay® NAV Catheter, Biosense-Webster, Diamond Bar, CA, or noncontact EnSite Array™, St. Jude Medical, St. Paul, MN). Timing at each site is usually correlated in reference to a fiducial point on the surface ECG that can be reliably observed. To maximize success, care is needed to ensure only the relevant PVC morphology is being mapped and to exclude fused beats (for example, PVC fusing with a conducted sinus beat), different morphologies, or catheter ectopy. A few points are taken to exclude any early sites in distant parts of the chamber. The main region of interest can then be focused upon with a high-density map. Careful attention is needed to prevent a mechanical bump to the PVC focus that will suppress PVCs. In case of a bump, empiric ablation at this location may be considered. Confirming catheter contact and integrating information from the bipolar signal between the tip and ring electrode and the unipolar tip recording can facilitate correct annotation of the activation timing at the tip electrode. The PVC focus will have the earliest local timing and a QS complex on unipolar electrogram in case of radial spread away from the focus. As opposed to focal PVCs, activation mapping to find the ideal ablation target site can be challenging for reentrant PVCs as there is no true “early focus” of origin. Instead, there is continuation of activation from the preceding QRS through areas of prolonged conduction (e.g., involving the tissue surrounding the valve annuli or fascicular/myocardial interface) prior to breakout to the global ventricular myocardium. Activation mapping guided ablation of the breakout site might simply shift the exit to some contiguous or noncontiguous ventricular tissue. Ablation of potentially spatially disparate tissue but with late diastolic activation preceding the surface QRS by even quite long and beat-to-beat variable intervals might be successful.
Figure 2.
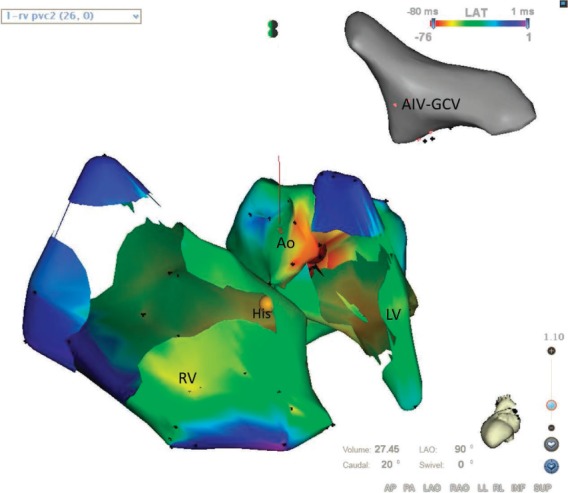
Three-dimensional electroanatomic activation maps obtained using point-by-point mapping in the right ventricle (RV), left ventricle (LV) and aortic valve cusps. Red represents the earliest site of activation at the left coronary cusp-right coronary cusp (LCC-RCC) commissure, and ablation at this site eliminated PVCs. No sites in the RV preceded the surface QRS by significant duration. The yellow dot represents site of His bundle. The anatomic location of the great cardiac vein/anterior interventricular vein (GCV-AIV) junction is shown.
Pace Mapping
Pace mapping relies on the principle that pace stimulation of the PVC site of origin would result in the surface QRS complex that exactly matches the target PVC morphology on all 12 surface ECG leads. Pace mapping can supplement activation mapping and can be particularly useful when activation mapping is not possible due to suppression of clinical PVCs.13 When PVCs are infrequent, pace mapping can exclude faraway sites and help shift the focus to the relevant chamber and site. The stimulus-to-surface QRS interval can further provide complementary information. Capture of arrhythmogenic tissue separated from ventricular myocardium by zones of slow conduction (e.g., above the aortic and pulmonary annuli) may result in long stimulus-to-QRS intervals (Figure 3). Pace mapping is not as specific as activation mapping in localizing the arrhythmogenic tissue, and the limitations of pace mapping need to be considered. When the focus of triggered PVC is surrounded by relatively healthy myocardium (e.g., in the posterior RVOT), pace mapping from a reasonably large surrounding area may result in an exact pace map.43 In such cases, the stimulus-to-QRS interval will be short. Tissue stimulation at threshold output (to capture only the tissue under the tip electrode) and at high output can produce different QRS morphologies (Figure 3). Even when pacing at the arrhythmogenic site, QRS morphology may be different due to capture of the surrounding myocardium or tissue on both sides of electrical boundaries (e.g., at fibrous valve annuli or insulation around Purkinje fibers). Far-field capture including anodal or virtual electrode capture may be unavoidable, especially at higher outputs. Pace mapping with pure capture of the critical isthmus for reentry can exit to the bulk of ventricular myocardium using not only orthodromic but also antidromic wavefront and thus not match the PVC morphology proceeding orthodromically44—for example, PVCs in the aortic valve cusps, aortomitral continuity, and the corresponding epicardial locations. However, the stimulus-to-QRS interval is usually long. Conversely, pacing at relatively distant sites in these locations may result in an exact match on all 12 ECG leads when distant tissues share a common exit to the bulk of ventricular myocardium.
Figure 3.
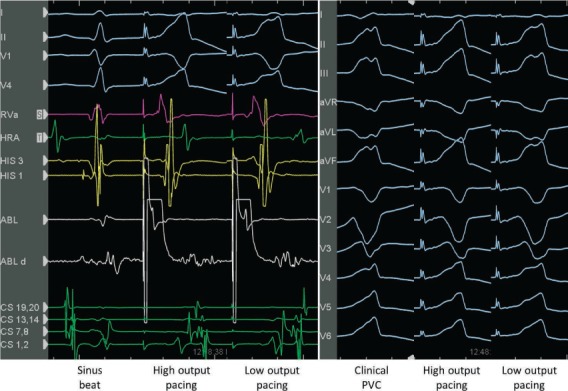
Pacing above the pulmonary valve at high and low output. Intracardiac electrograms and surface ECG are shown. At high output pacing there is a shorter stimulus-to-QRS duration likely due to far field capture of myocardium below the valve. At low output pacing with local muscle sleeve capture, there is a longer stimulus-to-QRS duration and QRS morphology similar to clinical premature ventricular complexes.
Outflow Tract PVCs
The goal of activation mapping is to find earliest sites ≳ 30 ms ahead of surface QRS onset.13 If no appreciably early sites are found, contiguous structures like the LVOT, coronary cusps,15 coronary veins,45,46 or epicardial space should be mapped, especially if ablation at the earliest site does not eliminate PVCs (Figure 2).47 Any sites with presystolic potentials that reliably precede the earliest activation during PVCs are potential targets.13,14 Any near-field potential that is late during sinus rhythm but jumps ahead during PVCs suggests reversal of activation and is potentially of interest. Such prepotentials can often be found across areas of fibrosis, for example, above the pulmonary valve or in the aortic sinuses of Valsalva.16,17,48 Additionally, any areas with fragmented low-amplitude signals or diastolic activity during sinus rhythm suggest abnormal substrate that might warrant ablation. Pace mapping can be unreliable in the semilunar valve cusps, and it may be impossible to capture the local myocardial extensions without directly capturing the myocardium below the valve.43 Of note, most RVOT PVCs are mapped and ablated at or above the level of the pulmonic valve leaflet attachments. Pacing with a long stimulus-to-QRS, even with an imperfect match, may suggest capture of arrhythmogenic substrate of reentrant PVCs, as the paced beat can exit to the ventricular myocardium differently (for example, through the antidromic rather than orthodromic wavefront).
Fascicular PVCs
The His-Purkinje (fascicular) tissue can give rise to focal (likely triggered automaticity) PVCs or ventricular tachycardia or serve as circuits for reentry. The fascicular tissue is covered with insulation that prevents activation spread to the contiguous myocardium. Thus, PVCs originating within the fascicular system exit to the ventricular myocardium at multiple distant “breakout” sites, and multiple similarly early distant ventricular sites may be mapped. Pace match may not be optimal at any site due to multiple exits through the fascicular system, and even an excellent surface QRS match at best can identify only the breakout site. Paced morphology at the arrhythmogenic focus is different than the clinical PVC because local myocardium is captured before the fascicular tissue. Due to these limitations, classic mapping maneuvers like entrainment, pace mapping, and activation mapping are of limited utility, and sorting out ablation target sites can be challenging (Table 4).18,19,49 In such cases, early high-frequency fascicular signals are of particular interest, and their activation needs to be annotated either in the same or a separate activation map. Relative timing of the early local fascicular signal-to-surface QRS complex during sinus rhythm and PVCs can identify the “focal” arrhythmogenic site. The most proximal site with a constant fascicular electrogram-to-surface QRS timing during PVCs and sinus beats is a good target. Further proximal sites will have a shorter electrogram-to-QRS time during PVCs when compared to sinus rhythm, because activation from a distal focus simultaneously activates the retrograde fascicular system and travels anterogradely to break out to the myocardium and generate the surface QRS complex (Figure 4).50 Fragmented pre-Purkinje potentials with reversal of sequence during sinus beats are associated with small reentrant circuits involving the fascicular tissue and are potential targets of ablation.18,19 It is worth pointing out that arrhythmogenesis of such fascicular PVCs may involve prolonged conduction zones close to the fascicular system interfacing with the adjacent myocardium, and the local fascicular signal may or may not participate in the PVC mechanism. In such cases, both the fascicular signals and any adjacent fragmented myocardial signals might be potential targets of ablation.19,51 However, earliest pre-Purkinje potentials may be recorded quite proximally in the His-Purkinje system with a high risk of AV block with ablation at such sites, and it may be prudent to initially target more distal prepotentials.18,19 Ablation targeting the fascicular signals in the posteroseptal region may lead to exit of the PVCs using other fascicles and change in QRS axis.52 Successful ablation of fascicular PVCs may require empiric ablation of Purkinje (and pre-Purkinje) signals and adjacent ventricular myocardium in the region of interest (e.g., at the left midventricular posteroseptal region). If mapping and targeted ablation of left posterior fascicular PVCs is not possible or is unsuccessful, an empiric linear ablation transversely in the posteroseptal region, halfway between base and apex, has been described as an effective technique.53 This usually transects the arrhythmogenic substrate and eliminates PVCs. Radiofrequency ablation of the fascicular tissue can elicit automaticity and induce refractory ventricular fibrillation.18,20
Table 4.
Challenges in application of mapping maneuvers to identify arrhythmogenic sites for ablation of fascicular premature ventricular complexes.

Figure 4.
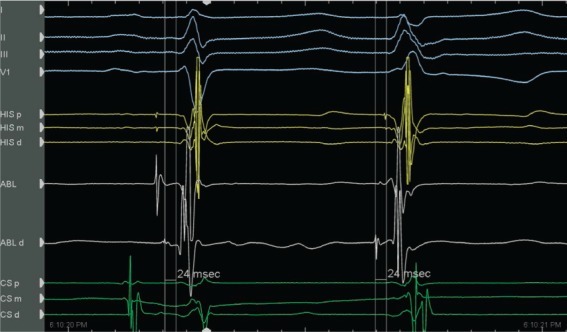
Mapping the left anterior fascicular focus of PVC. The first beat is a sinus beat with proximal to distal activation of the fascicular system preceding the QRS complex. The second beat is the PVC with reversal of fascicular activation from the distal to the proximal bipole of the quadripolar-mapping catheter. The conduction time from the focus (sharp fascicular signal on ABL d) to the surface QRS is constant during sinus rhythm and PVC (24 ms). At more proximal sites (ABL, His), the fascicular signal to QRS time becomes shorter with PVC beat.
PVCs from Intracavitary Structures
Intracavitary structures such as papillary muscles (Figure 5), false tendons, and the moderator band carry fascicular tissue and can be the arrhythmogenic substrate in apparently normal as well as diseased hearts.5 The pathogenesis of PVCs from intracavitary structures overlaps with fascicular PVCs. The papillary muscles have a dense fascicular network, and often both the fascicular tissue and the myocardium, especially the interfaces between the two, are integral to the mechanism of PVCs. The same patient may have different PVC morphologies as the ectopy exits out either the fascicular system or the local papillary muscle myocardium. It is important to recognize signals from such sites during electroanatomic mapping and not exclude these as “poor contact” points. Intracardiac echocardiography is indispensable for detailed mapping of intracavitary structures because stable catheter contact is otherwise difficult, and effective energy delivery may not be possible. Isolation of the entire structure is often required—for example, circumferential ablation around the base of the papillary muscle or at both attachments of false tendons or moderator band—due to extensive arrhythmogenic substrate with multiple possible exits and difficulty in catheter stability.
Figure 5.
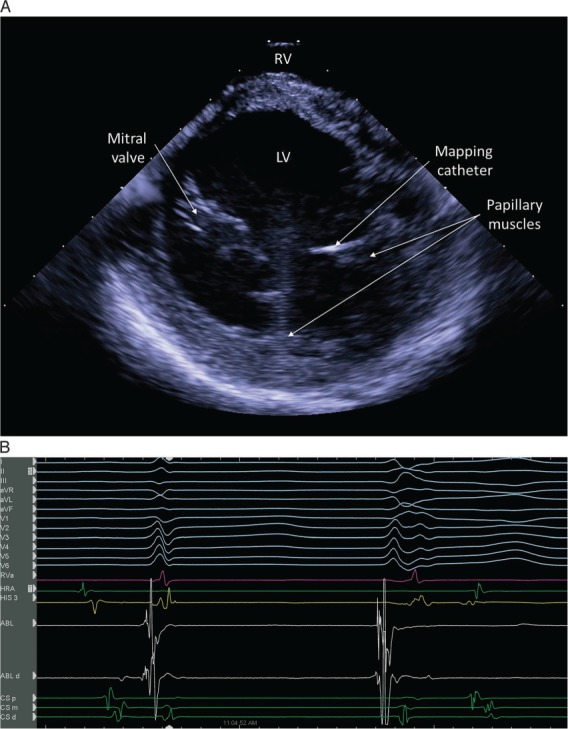
(A) Intracardiac echocardiography (ICE) image obtained from the right ventricular (RV) outflow tract showing mapping catheter on the left ventricular (LV) anterior papillary muscle. (B) A sharp fascicular signal is seen after onset of ventricular activation during sinus beat (on the left); the fascicular signal jumps ahead of ventricular activation during premature ventricular complexes (PVCs) (on the right). Pace mapping from the papillary muscle with ICE guidance showed multiple morphologies. Extensive ablation around the base of the papillary muscle eliminated the papillary muscle PVCs.
Scar-Related PVCs
PVCs related to myocardial scar stem from a slowly conducting protected isthmus within the scar that can cause reentrant beats following unidirectional block. Pace mapping can help identify the exit sites of such slow-conduction channels. Sites further within the protected isthmus will have a long stimulus-to-surface QRS on pacing but may lack a good match due to capture of far-field electrograms or propagation of the antidromic wavefront out through the entrance site. Mapping will identify diastolic activity with fragmented, low-voltage, split, or late potentials during sinus rhythm as potential diastolic channels, and such activity precedes the onset of clinical PVCs. All such abnormal sites within the scar are potentially arrhythmogenic and may be targeted with ablation.
Outcomes
Ablation of outflow tract or fascicular PVCs is reportedly successful in 80% to 100% of cases.13,33 In two-thirds of the patients undergoing PVC ablation due to PVC-mediated cardiomyopathy, LV function improves to normal within 4 months, although in some cases it takes more than a year.33,38,39 Recurrence after successful ablation is possible due to remodeling of the arrhythmogenic substrate or reconnection to exit sites.
The risk of collateral injury with ablation to PVCs originating close to critical structures needs to be considered.4,13 Coronary arterial injury can occur when ablating in the coronary veins (Figure 6), epicardial space, above the coronary cusps close to coronary ostia, and the posterior RVOT near the pulmonary valve, close to the course of the left main coronary artery. Cryoablation has been suggested to be safe only 3 mm away from the coronary artery, while radiofrequency ablation within 1 cm of the coronary artery or the conduction system might lead to irreversible damage. Cryomapping can be used when ablating close to the conduction system. Ablation in the mid-septum below the mitral valve leaflet, even in the absence of a large atrial electrogram, might cause damage to the AV node due to the basal displacement of the mitral valve compared to the tricuspid valve. Ablation of PVCs in the aortic cusps is generally safe, although AV block can occur if the catheter inadvertently slips to the septum below the valve. Phrenic nerve injury is possible during epicardial ablation, and pacing should be done to exclude phrenic nerve capture prior to ablation in the posterolateral LV region. Apart from proximity to critical structures, ablation may not be possible if the arrhythmia originates from inaccessible areas such as the LV summit46,54 (Figure 7) or tissue protected by surgical sutures (for example, tissue in the prosthetic valve sowing ring). Infrequent PVCs might make mapping impossible, and the procedure might have to be repeated on a different day.
Figure 6.
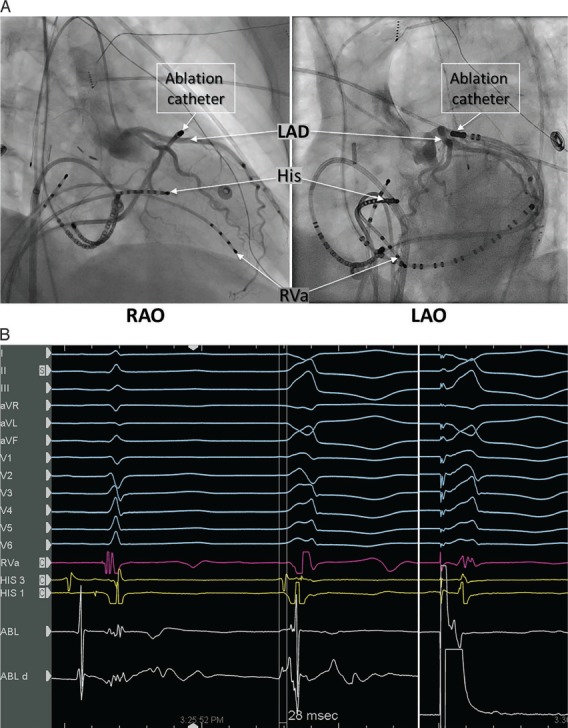
(A) Left coronary angiography showing the close relation of the left anterior descending (LAD) artery with the ablation catheter at the great cardiac vein/anterior interventricular vein (GCV-AIV) junction. (B) This site at the GCV-AIV junction was the earliest activation during PVC, with a prepotential 28 ms ahead of the surface QRS (middle beat); pacing from this site generated a slightly different QRS complex (right beat) compared to clinical PVC. Due to proximity to the LAD, ablation was not performed. RAO: right anterior oblique; LAO: left anterior oblique; RVa: right ventricular apex.
Figure 7.
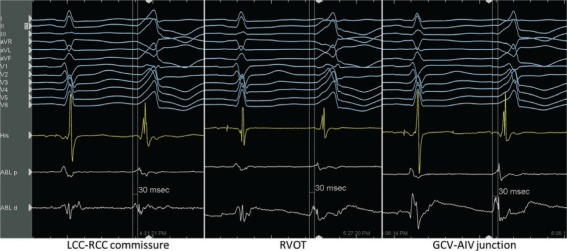
Premature ventricular complexes (PVCs) originating from region of left ventricular (LV) summit. Far-field activation was equally early (30 ms ahead of surface QRS) in regions of the left coronary cusp-right coronary cusp (LCC-RCC), right ventricular outflow tract (RVOT), and epicardially in great cardiac vein-anterior interventricular vein (GCV-AIV). Ablation from all these sites in this case was able to block all exits from the focus and eliminate PVCs.
Catheter entrapment in the chordal apparatus is rare but can occur, especially with circular and multipronged catheters, and may require surgical correction. Aortic valve perforation is possible if ablation is performed with the catheter tip poking into the cusp rather than apposed to the vessel wall, and inadvertent ablation within the coronary ostium can occur. Retrograde aortic entry into the ventricle should be performed with the catheter tip pointing backwards to prevent valve perforation or engagement of the coronary artery. Thromboembolic complications can be minimized with therapeutic heparin anticoagulation during the procedure. With extensive left heart ablation, 8 to 12 weeks of therapeutic postprocedural anticoagulation is recommended. Strategies to reduce radiation exposure should be employed to minimize adverse radiation effects for patients and operators.
Conclusion
Premature ventricular complexes are generally considered to be benign and are only occasionally symptomatic. However, the physician should be mindful that in certain cases PVCs result in congestive heart failure or sudden cardiac death. For asymptomatic patients with preserved cardiac function and no high-risk features for sudden cardiac death, careful follow-up will suffice. In patients showing a clear association between PVCs and symptoms, PVC-induced ventricular tachyarrhythmia, or PVC-mediated cardiomyopathy, the risks and benefits of various drug options and catheter ablation should be considered in the context of the patient and PVC characteristics.
Conflict of Interest Disclosure: Dr. Asirvatham has industry relationships with Abiomed, AtriCure, Inc., Biotronik, Biosense Webster Inc., Boston Scientific Corporation, Medtronic, Inc., Spectranetics, St. Jude Medical, Inc., Sanofi-Aventis, Wolters Kluwer, Elsevier, and is a co-patent holder of Aegis Sciences Corp., Access Point Technologies, Nevro Corp., Sanovas Inc., and Sorin Group.
Footnotes
ECG, electrocardiogram; PVC, premature ventricular complex; LBBB, left bundle branch block; RBBB, right bundle branch block
ECG, electrocardiogram; RBBB, right bundle branch block
References
- 1.Kennedy HL, Whitlock JA, Sprague MK, Kennedy LJ, Buckingham TA, Goldberg RJ. Long-term follow-up of asymptomatic healthy subjects with frequent and complex ventricular ectopy. The New England journal of medicine. 1985;312(4):193–197. doi: 10.1056/NEJM198501243120401. [DOI] [PubMed] [Google Scholar]
- 2.Agarwal SK, Heiss G, Rautaharju PM, Shahar E, Massing MW, Simpson RJ., Jr. Premature ventricular complexes and the risk of incident stroke: the Atherosclerosis Risk In Communities (ARIC) Study. Stroke; a journal of cerebral circulation. 2010;41(4):588–593. doi: 10.1161/STROKEAHA.109.567800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ataklte F, Erqou S, Laukkanen J, Kaptoge S. Meta-analysis of ventricular premature complexes and their relation to cardiac mortality in general populations. The American journal of cardiology. 2013;112(8):1263–1270. doi: 10.1016/j.amjcard.2013.05.065. [DOI] [PubMed] [Google Scholar]
- 4.Asirvatham SJ. Correlative anatomy for the invasive electrophysiologist: outflow tract and supravalvar arrhythmia. J Cardiovasc Electrophysiol. 2009;20(8):955–968. doi: 10.1111/j.1540-8167.2009.01472.x. [DOI] [PubMed] [Google Scholar]
- 5.Syed FF, Hai JJ, Lachman N, DeSimone CV, Asirvatham SJ. The infrahisian conduction system and endocavitary cardiac structures: relevance for the invasive electrophysiologist. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2014;39(1):45–56. doi: 10.1007/s10840-013-9858-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tada H, Ito S, Naito S et al. Idiopathic ventricular arrhythmia arising from the mitral annulus: a distinct subgroup of idiopathic ventricular arrhythmias. J Am Coll Cardiol. 2005;45(6):877–886. doi: 10.1016/j.jacc.2004.12.025. [DOI] [PubMed] [Google Scholar]
- 7.Tada H, Tadokoro K, Ito S et al. Idiopathic ventricular arrhythmias originating from the tricuspid annulus: Prevalence, electrocardiographic characteristics, and results of radiofrequency catheter ablation. Heart Rhythm : the official journal of the Heart Rhythm Society. 2007;4(1):7–16. doi: 10.1016/j.hrthm.2006.09.025. [DOI] [PubMed] [Google Scholar]
- 8.Bogun F, Crawford T, Chalfoun N et al. Relationship of frequent postinfarction premature ventricular complexes to the reentry circuit of scar-related ventricular tachycardia. Heart Rhythm. 2008;5(3):367–374. doi: 10.1016/j.hrthm.2007.11.026. [DOI] [PubMed] [Google Scholar]
- 9.Sriram CS, Syed FF, Ferguson ME et al. Malignant bileaflet mitral valve prolapse syndrome in patients with otherwise idiopathic out-of-hospital cardiac arrest. J Am Coll Cardiol. 2013;62(3):222–230. doi: 10.1016/j.jacc.2013.02.060. [DOI] [PubMed] [Google Scholar]
- 10.Jongbloed MR, Mahtab EA, Blom NA, Schalij MJ, Gittenberger-de Groot AC. Development of the cardiac conduction system and the possible relation to predilection sites of arrhythmogenesis. TheScientificWorldJournal. 2008;8:239–269. doi: 10.1100/tsw.2008.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hasdemir C, Alp A, Simsek E, Kose N, Aydin M, Payzin S. Spontaneous atrioventricular nodal reentrant tachycardia in patients with idiopathic ventricular arrhythmias: the incidence, clinical, and electrophysiologic characteristics. J Cardiovasc Electrophysiol. 2013;24(12):1370–1374. doi: 10.1111/jce.12249. [DOI] [PubMed] [Google Scholar]
- 12.Lerman BB, Belardinelli L, West GA, Berne RM, DiMarco JP. Adenosine-sensitive ventricular tachycardia: evidence suggesting cyclic AMP-mediated triggered activity. Circulation. 1986;74(2):270–280. doi: 10.1161/01.cir.74.2.270. [DOI] [PubMed] [Google Scholar]
- 13.Adams JC, Srivathsan K, Shen WK. Advances in management of premature ventricular contractions. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2012;35(2):137–149. doi: 10.1007/s10840-012-9698-x. [DOI] [PubMed] [Google Scholar]
- 14.Liu XY, Zhao YJ, Wang LX et al. The electrophysiological characteristics of isolated diastolic potentials in idiopathic ventricular arrhythmias arising from the right ventricular outflow tract. Acta cardiologica. 2014;69(1):29–38. doi: 10.1080/ac.69.1.3011342. [DOI] [PubMed] [Google Scholar]
- 15.Suleiman M, Asirvatham SJ. Ablation above the semilunar valves: when, why, and how? Part I. Heart Rhythm : the official journal of the Heart Rhythm Society. 2008;5(10):1485–1492. doi: 10.1016/j.hrthm.2008.04.019. [DOI] [PubMed] [Google Scholar]
- 16.Gami AS, Noheria A, Lachman N et al. Anatomical correlates relevant to ablation above the semilunar valves for the cardiac electrophysiologist: a study of 603 hearts. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2011;30(1):5–15. doi: 10.1007/s10840-010-9523-3. [DOI] [PubMed] [Google Scholar]
- 17.Tabatabaei N, Asirvatham SJ. Supravalvular arrhythmia: identifying and ablating the substrate. Circ Arrhythm Electrophysiol. 2009;2(3):316–326. doi: 10.1161/CIRCEP.108.847962. [DOI] [PubMed] [Google Scholar]
- 18.Nogami A. Purkinje-related arrhythmias part I: monomorphic ventricular tachycardias. Pacing and clinical electrophysiology : PACE. 2011;34(5):624–650. doi: 10.1111/j.1540-8159.2011.03044.x. [DOI] [PubMed] [Google Scholar]
- 19.Nogami A, Naito S, Tada H et al. Demonstration of diastolic and presystolic Purkinje potentials as critical potentials in a macroreentry circuit of verapamil-sensitive idiopathic left ventricular tachycardia. J Am Coll Cardiol. 2000;36(3):811–823. doi: 10.1016/s0735-1097(00)00780-4. [DOI] [PubMed] [Google Scholar]
- 20.Scheinman MM. Role of the His-Purkinje system in the genesis of cardiac arrhythmia. Heart Rhythm. 2009;6(7):1050–1058. doi: 10.1016/j.hrthm.2009.03.011. [DOI] [PubMed] [Google Scholar]
- 21.Ouyang F, Fotuhi P, Ho SY et al. Repetitive monomorphic ventricular tachycardia originating from the aortic sinus cusp: electrocardiographic characterization for guiding catheter ablation. J Am Coll Cardiol. 2002;39(3):500–508. doi: 10.1016/s0735-1097(01)01767-3. [DOI] [PubMed] [Google Scholar]
- 22.Berruezo A, Mont L, Nava S, Chueca E, Bartholomay E, Brugada J. Electrocardiographic recognition of the epicardial origin of ventricular tachycardias. Circulation. 2004;109(15):1842–1847. doi: 10.1161/01.CIR.0000125525.04081.4B. [DOI] [PubMed] [Google Scholar]
- 23.Daniels DV, Lu Y-Y, Morton JB et al. Idiopathic epicardial left ventricular tachycardia originating remote from the sinus of Valsalva: electrophysiological characteristics, catheter ablation, and identification from the 12-lead electrocardiogram. Circulation. 2006;Vol 113:1659–1666. doi: 10.1161/CIRCULATIONAHA.105.611640. [DOI] [PubMed] [Google Scholar]
- 24.Yamada T, Doppalapudi H, McElderry HT et al. Idiopathic ventricular arrhythmias originating from the papillary muscles in the left ventricle: prevalence, electrocardiographic and electrophysiological characteristics, and results of the radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 2010;21(1):62–69. doi: 10.1111/j.1540-8167.2009.01594.x. [DOI] [PubMed] [Google Scholar]
- 25.Good E, Desjardins B, Jongnarangsin K et al. Ventricular arrhythmias originating from a papillary muscle in patients without prior infarction: a comparison with fascicular arrhythmias. Heart Rhythm. 2008;5(11):1530–1537. doi: 10.1016/j.hrthm.2008.08.032. [DOI] [PubMed] [Google Scholar]
- 26.Bradfield JS, Homsi M, Shivkumar K, Miller JM. Coupling interval variability differentiates ventricular ectopic complexes arising in the aortic sinus of valsalva and great cardiac vein from other sources: mechanistic and arrhythmic risk implications. J Am Coll Cardiol. 2014;63(20):2151–2158. doi: 10.1016/j.jacc.2014.02.551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Noda T, Shimizu W, Taguchi A et al. Malignant entity of idiopathic ventricular fibrillation and polymorphic ventricular tachycardia initiated by premature extrasystoles originating from the right ventricular outflow tract. J Am Coll Cardiol. 2005;46(7):1288–1294. doi: 10.1016/j.jacc.2005.05.077. [DOI] [PubMed] [Google Scholar]
- 28.Santoro F, Biase LD, Hranitzky P et al. Ventricular Fibrillation Triggered by PVCs from Papillary Muscles: Clinical Features and Ablation. J Cardiovasc Electrophysiol. 2014 doi: 10.1111/jce.12478. [DOI] [PubMed] [Google Scholar]
- 29.Kim RJ, Iwai S, Markowitz SM, Shah BK, Stein KM, Lerman BB. Clinical and electrophysiological spectrum of idiopathic ventricular outflow tract arrhythmias. J Am Coll Cardiol. 2007;49(20):2035–2043. doi: 10.1016/j.jacc.2007.01.085. [DOI] [PubMed] [Google Scholar]
- 30.Kawamura M, Badhwar N, Vedantham V et al. Coupling interval dispersion and body mass index are independent predictors of idiopathic premature ventricular complex-induced cardiomyopathy. J Cardiovasc Electrophysiol. 2014;25(7):756–762. doi: 10.1111/jce.12391. [DOI] [PubMed] [Google Scholar]
- 31.Yokokawa M, Kim HM, Good E et al. Relation of symptoms and symptom duration to premature ventricular complex-induced cardiomyopathy. Heart Rhythm. 2012;9(1):92–95. doi: 10.1016/j.hrthm.2011.08.015. [DOI] [PubMed] [Google Scholar]
- 32.Olgun H, Yokokawa M, Baman T et al. The role of interpolation in PVC-induced cardiomyopathy. Heart Rhythm : the official journal of the Heart Rhythm Society. 2011;8(7):1046–1049. doi: 10.1016/j.hrthm.2011.02.034. [DOI] [PubMed] [Google Scholar]
- 33.Cha Y-M, Lee GK, Klarich KW, Grogan M. Premature ventricular contraction-induced cardiomyopathy: a treatable condition. Circ Arrhythm Electrophysiol. 2012;5(1):229–236. doi: 10.1161/CIRCEP.111.963348. [DOI] [PubMed] [Google Scholar]
- 34.Del Carpio Munoz F, Syed FF, Noheria A et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol. 2011;22(7):791–798. doi: 10.1111/j.1540-8167.2011.02021.x. [DOI] [PubMed] [Google Scholar]
- 35.Huizar JF, Kaszala K, Potfay J et al. Left ventricular systolic dysfunction induced by ventricular ectopy: a novel model for premature ventricular contraction-induced cardiomyopathy. Circ Arrhythm Electrophysiol. 2011;4(4):543–549. doi: 10.1161/CIRCEP.111.962381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wang Y, Eltit JM, Kaszala K et al. Cellular mechanism of premature ventricular contraction-induced cardiomyopathy. Heart Rhythm. 2014;11(11):2064–2072. doi: 10.1016/j.hrthm.2014.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lakkireddy D, Di Biase L, Ryschon K et al. Radiofrequency Ablation of Premature Ventricular Ectopy Improves the Efficacy of Cardiac Resynchronization Therapy in Nonresponders. J Am Coll Cardiol. 2012;60(16):1531–1539. doi: 10.1016/j.jacc.2012.06.035. [DOI] [PubMed] [Google Scholar]
- 38.Zhong L, Lee YH, Huang XM et al. Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: a single-center retrospective study. Heart Rhythm. 2014;11(2):187–193. doi: 10.1016/j.hrthm.2013.10.033. [DOI] [PubMed] [Google Scholar]
- 39.Ling Z, Liu Z, Su L et al. Radiofrequency ablation versus antiarrhythmic medication for treatment of ventricular premature beats from the right ventricular outflow tract: prospective randomized study. Circ Arrhythm Electrophysiol. 2014;7(2):237–243. doi: 10.1161/CIRCEP.113.000805. [DOI] [PubMed] [Google Scholar]
- 40.Zipes DP, Camm AJ, Borggrefe M et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114(10):e385–484. doi: 10.1161/CIRCULATIONAHA.106.178233. [DOI] [PubMed] [Google Scholar]
- 41.Hasdemir C, Alp A, Aydin M, Can LH. Human model simulating right ventricular outflow tract tachycardia by high-frequency stimulation in the left pulmonary artery: autonomics and idiopathic ventricular arrhythmias. J Cardiovasc Electrophysiol. 2009;20(7):759–763. doi: 10.1111/j.1540-8167.2009.01442.x. [DOI] [PubMed] [Google Scholar]
- 42.Jesuraj ML, Rao BH, Sharada K, Narasimhan C. Idiopathic right ventricular tract outflow tachycardia induced by high-frequency stimulation. J Cardiovasc Electrophysiol. 2013;24(2):221–223. doi: 10.1111/j.1540-8167.2012.02386.x. [DOI] [PubMed] [Google Scholar]
- 43.Bogun F, Taj M, Ting M et al. Spatial resolution of pace mapping of idiopathic ventricular tachycardia/ectopy originating in the right ventricular outflow tract. Heart Rhythm. 2008;5(3):339–344. doi: 10.1016/j.hrthm.2007.11.011. [DOI] [PubMed] [Google Scholar]
- 44.Brunckhorst CB, Delacretaz E, Soejima K, Maisel WH, Friedman PL, Stevenson WG. Identification of the ventricular tachycardia isthmus after infarction by pace mapping. Circulation. 2004;110(6):652–659. doi: 10.1161/01.CIR.0000138107.11518.AF. [DOI] [PubMed] [Google Scholar]
- 45.Baman TS, Ilg KJ, Gupta SK et al. Mapping and ablation of epicardial idiopathic ventricular arrhythmias from within the coronary venous system. Circ Arrhythm Electrophysiol. 2010;3(3):274–279. doi: 10.1161/CIRCEP.109.910802. [DOI] [PubMed] [Google Scholar]
- 46.Jauregui Abularach ME, Campos B, Park K-M et al. Ablation of ventricular arrhythmias arising near the anterior epicardial veins from the left sinus of Valsalva region: ECG features, anatomic distance, and outcome. Heart Rhythm : the official journal of the Heart Rhythm Society. 2012;9(6):865–873. doi: 10.1016/j.hrthm.2012.01.022. [DOI] [PubMed] [Google Scholar]
- 47.Yokokawa M, Good E, Crawford T et al. Reasons for failed ablation for idiopathic right ventricular outflow tract-like ventricular arrhythmias. Heart Rhythm. 2013;10(8):1101–1108. doi: 10.1016/j.hrthm.2013.05.011. [DOI] [PubMed] [Google Scholar]
- 48.Kamakura S, Shimizu W, Matsuo K et al. Localization of optimal ablation site of idiopathic ventricular tachycardia from right and left ventricular outflow tract by body surface ECG. Circulation. 1998;98(15):1525–1533. doi: 10.1161/01.cir.98.15.1525. [DOI] [PubMed] [Google Scholar]
- 49.Stevenson WG, Friedman PL, Sager PT et al. Exploring postinfarction reentrant ventricular tachycardia with entrainment mapping. J Am Coll Cardiol. 1997;29(6):1180–1189. doi: 10.1016/s0735-1097(97)00065-x. [DOI] [PubMed] [Google Scholar]
- 50.Ma W, Wang X, Cingolani E et al. Mapping and ablation of ventricular tachycardia from the left upper fascicle: how to make the most of the fascicular potential? Circ Arrhythm Electrophysiol. 2013;6(4):e47–51. doi: 10.1161/CIRCEP.113.000249. [DOI] [PubMed] [Google Scholar]
- 51.Arya A, Haghjoo M, Emkanjoo Z et al. Comparison of presystolic purkinje and late diastolic potentials for selection of ablation site in idiopathic verapamil sensitive left ventricular tachycardia. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2004;11(2):135–141. doi: 10.1023/B:JICE.0000042352.86366.fa. [DOI] [PubMed] [Google Scholar]
- 52.Sung RK, Kim AM, Tseng ZH et al. Diagnosis and ablation of multiform fascicular tachycardia. J Cardiovasc Electrophysiol. 2013;24(3):297–304. doi: 10.1111/jce.12020. [DOI] [PubMed] [Google Scholar]
- 53.Lin D, Hsia HH, Gerstenfeld EP et al. Idiopathic fascicular left ventricular tachycardia: linear ablation lesion strategy for noninducible or nonsustained tachycardia. Heart Rhythm. 2005;2(9):934–939. doi: 10.1016/j.hrthm.2005.06.009. [DOI] [PubMed] [Google Scholar]
- 54.Yamada T, McElderry HT, Doppalapudi H et al. Idiopathic ventricular arrhythmias originating from the left ventricular summit: anatomic concepts relevant to ablation. Circ Arrhythm Electrophysiol. 2010;3(6):616–623. doi: 10.1161/CIRCEP.110.939744. [DOI] [PubMed] [Google Scholar]