

Abstract
Purpose
This study evaluated the relationship between parenting style, sociodemographic data, caries status, and child’s behavior during the first dental visit.
Methods
Parents/legal guardians of new patients aged three to six years presenting to Nationwide Children’s Hospital dental clinic for an initial examination/hygiene appointment completed the Parenting Styles and Dimensions Questionnaire (PSDQ) to assess parenting style and a 15-question demographic survey. Blinded and calibrated expanded function dental auxiliaries or dental hygienists (EFDA/DH) performed a prophylaxis and assessed child behavior using the Frankl scale (inter-rater reliability was 92 percent). A blinded and calibrated dentist performed an oral examination.
Results
132 parent/child dyads participated. Children with authoritative parents exhibited more positive behavior (P<.001) and less caries (P<.001) compared to children with authoritarian and permissive parents. Children attending daycare exhibited more positive behavior compared to children who did not (P<.001). Patients with private dental insurance exhibited more positive behavior (P>.04) and less caries (P>.024) compared to children with Medicaid or no dental insurance.
Conclusions
Authoritative parenting and having private dental insurance were associated with less caries and better behavior during the first dental visit. Attending daycare was associated with better behavior during the first dental visit.
Keywords: PARENTING STYLES, CARIES, CHILD BEHAVIOR
A child’s behavior can make it challenging to provide effective dental treatment. Children vary in their responses to the dental experience, which are influenced by health, culture, parenting styles, age, cognitive level, anxiety and fear, reaction to strangers, pathology, social expectations, and the temperament.1–9 Parents play a large role in how a child behaves at the dental appointment, especially when they have had negative experiences with dentists themselves. An anxious or fearful parent can negatively affect the child’s behavior in the dental office.4,10
Parenting styles have been viewed with extreme interest recently. Parents, as primary caregivers, exert a significant influence on the development of their child’s present and future emotional health, personality, character,11 well-being, social and cognitive development, and academic performance.12–18 Parenting style is an essential determinant of children’s coping styles, and a child’s behavior toward adults varies according to different parenting styles. This transfers to the dental office, affecting the interaction with the dentist. Parenting style also influences how a child copes with stresses and stimuli, including those in the dental setting.19
Baumrind defined three specific parenting styles: (1) authoritative; (2) authoritarian; and (3) permissive (Table 1).18,20 The authoritarian (high control, low warmth) parenting style is defined by harsh parenting practices, including physical punishment, yelling, and commands.21 Children in authoritarian homes are often withdrawn and distrustful.18 The authoritative (high warmth, high control) parent exhibits firm limit-setting, yet shows compassion and warmth, and these households have bidirectional communication.21 The permissive (high warmth, low control) parent provides few to no commands or limits to behavior, and often spoils and coddles the child.21 Children in a permissive household are “co-owners” of the house as far as rules go but have no responsibility.18
Table 1.
DESCRIPTION OF PARENTING STYLES
| Parenting style | Description |
|---|---|
| Authoritative | High parental responsiveness and high parental demand; warmth and involvement, reasoning/induction, demographic participation |
| Authoritarian | Low parental responsiveness but high parental demand; clear parental authority, unquestioning obedience and punitive strategies |
| Permissive | High parental responsiveness but low parental demand; tolerance, general acceptance of child’s decisions and tendencies to ignore child’s misbehavior |
| Neglecting | Low parental responsiveness and low parental demand |
Lamborn describes another type of parenting style: neglectful. The neglectful style is defined by low warmth and low control, and describes emotionally detached parents.14 These parents are typically not responsive and are uninvolved in their children’s lives. They do not volunteer to be studied, so minimal research exists on this parenting style. Because of the limited data on these families, the current study did not address the neglectful parenting style.
The Diplomates of the American Board of Pediatric Dentistry agreed in 2002 that, during their years of practicing dentistry, parenting styles had changed. Ninety-two percent felt these changes were bad, and 85 percent felt these resulted in worse patient behaviors.22 This evolution of parenting styles is documented in the current literature, specifically noting an increase in indulgent parenting.15,23 These shifts have contributed to an increased potential for dental disease, limited capacity of children to behave, and decreased parental control over their child’s behavior.15 Specific behaviors can prolong the time in the dental chair or create a need to use more advanced methods of behavior management, such as general anesthesia. Poor behavior can delay necessary dental treatment, thus allowing further progression of disease.
Parents today want to prevent their children from experiencing any pain or discomfort. Sheller suggests this is a step away from the ‘traditional’ parenting techniques of setting limits and saying ‘no’.23 Many parents are less accountable for behavior of their children and provide less discipline, relying more on medical or psychological methods of management.23 Parenting styles are changing, and pediatric dentists should be aware of these changes to be prepared to treat each patient in the most efficient and effective manner.
Parenting styles influence the health of children. Childhood obesity and sugar consumption are on the rise for children,24,25 and this is a concern for the oral and overall health of children. Less obesigenic environments are associated with authoritative parenting.26 Another study indicates that obesity is most likely associated with authoritarian parenting, and that children from indulgent homes have twice the risk of being obese than children from authoritative homes.27 Parenting affects the child’s consumption of a sugary diet,28 and authoritative parents have healthier food choices for their children.29
Evidence supports a potential relationship between parenting styles, child behavior, and dental caries, but limited research investigates this topic. The most relevant and closely related publication is by Aminabadi et al., which showed a correlation between parenting styles and the child’s behavior during a restorative dental visit.30 Aminabadi et al. gave preliminary evidence that a child’s reaction to “restorative dental procedures is influenced by the nature of the caregiver’s parenting style.”30 This publication also suggests that permissive and authoritarian parenting styles are associated with much worse behavior than the authoritative style.30 The limited literature on parenting styles suggests that little is known about the effects of parenting on dental behaviors.
The purpose of this study was to investigate the relationship between parenting styles, the child’s behavior in the dental setting, and caries status of the child.
Methods
Sample
This study was approved by the Human Subjects Committee of Nationwide Children’s Hospital, Columbus, Ohio (IRB13-00266). The sample was drawn from patients presenting to Nationwide Children’s Hospital for their first dental visit. Selection criteria for inclusion were: three-to six-year-old patients; English-speaking; no known medical conditions limiting the child’s cognitive development; no diagnosed chronic medical conditions; no history of dental procedures elsewhere; no history of phobias related to the dental or medical setting; no history of pain secondary to pulpitis; and no diagnosed behavior disorders.
Procedure
Patients were prescreened from the electronic health record (EHR) at Nationwide Children’s Hospital upon scheduling in order to assess qualification for the study. They were prescreened by a second-year dental student from The Ohio State University, Columbus, who had no interaction with the parent/child dyad and was not involved in data collection. Normal procedure for the first dental visit was followed: the expanded function dental auxiliary or dental hygienist (EFDA/ DH) completed the dental cleaning and assessed behavior, and a calibrated pediatric dentist or resident, who had no other interaction with the parent/child dyad, performed the comprehensive examination and assessed caries status. Caries status was then indicated as either ‘positive’, meaning caries was present, or ‘negative’, meaning caries was not present. The operators were blind to parenting style. The parents of qualified patients were then given a description of the study by two of the principal investigators. If parents agreed to participate and inclusion criteria were confirmed, these same investigators obtained informed consent, and the parent filled out the Parenting Styles and Dimensions Questionnaire (PSDQ) and an additional questionnaire. Questionnaires were collected prior to the parent leaving. Two prospective study parents declined to participate in the study because they had brought other young children. Data from the questionnaires and EHR were transferred to a secure spreadsheet (Excel, Microsoft Corp., Redmond, Wash., USA).
Instruments
The PSDQ31 contains 32 statements regarding different parent reactions to child behavior. This shortened, validated, and reliable version was used in this study for convenience and time considerations. This questionnaire assesses the parenting style based on Baumrind’s primary parenting types: authoritarian; authoritative; and permissive.18 For example, ‘we spoil our child’ correlates to the permissive parenting style, while ‘we give our child reasons why rules should be obeyed’ correlates to the authoritative parenting style. Each parent was asked to rank each statement on a Likert scale of 1 to 5 (1 equals never, 2 equals once in a while, 3 equals half the time, 4 equals very often, and 5 equals always) as to how often they and their spouse/significant other (if applicable) exhibited each behavior. “The internal consistency-reliability of each question in the PSDQ is good to excellent, and both mothers and fathers of school-age children can complete this questionnaire.”31
The scoring key of the PSDQ was used to classify parents into one of the three specific parenting styles.20,31 For the authoritative parenting style, there are 15 items with a potential range of scores from zero to 75. The authoritarian style includes 12 items with a potential range of zero to 60. The permissive style includes five items with a potential range of zero to 25. An overall mean score in each parenting style category was calculated, and this score determined the parent’s particular style; the highest mean score placed the parent in the proper parenting category. This was used as the primary behavior rating scale.
The second part of the questionnaire involved individual data about the child and the family, including: household income; educational level; marital status; health information; number of children; daycare status; and social information.
A reliable and common behavior scale used in dentistry and research is the Frankl scale,2,32,33 which has four potential rankings for the child’s behavior, including definitely negative, negative, positive, and definitely positive.
Calibration procedures
A panel of four pediatric dental experts reviewed and validated a series of five videos showing different young children’s behavior during dental visits. Before viewing the videos, the dentists were trained and calibrated on the Frankl scale. Then, they reviewed the videos independently and rated the behavior shown on each video. The reliability between doctors’ ratings was assessed by intraclass correlation coefficient and was equal to 1 (95 percent confidence interval [CI], P<.001), thus validating the videos. Once these videos were validated, the EFDA/DHs participating in the study were trained and calibrated on the Frankl scale. The EFDA/DHs viewed the series of videos individually and rated the shown behavior. The process was repeated for the EFDA/DHs a month later to determine their intrarater reliability. Spearman’s correlation coefficient determined that the inter-rater reliability was 92 percent (95 percent CI, P<.001) and intrarater reliability was 91 percent (95 percent CI, P>.03).
Examining dentists used clinical and radiographic criteria to assess caries and were not calibrated beyond clinical calibration. This exam was performed following the cleaning and X-rays, consistent with procedures for a new patient exam.
Results
Data collection was completed for 132 parent/child dyads. The mean patient age was 4.25 years (±0.63 years). Eighty-seven parents (66 percent) exhibited authoritative parenting, 33 (25 percent) exhibited permissive parenting, 11 (eight percent) exhibited authoritarian parenting, and one (one percent) exhibited permissive/authoritative parenting. The data set for the single authoritative/permissive household was not included in the statistical analysis to maintain discrete cohorts; hence, the sample for the analysis was 131. For 124 patients, the mother was the respondent; for seven, the father was the respondent. Table 2 illustrates the sociodemographic distribution gathered. Race was largely divided into Caucasian and African American, so the other races (Somali, European, Asian, Hispanic, and Indian) were combined into an ‘other’ category. For statistical analysis, behavior was dichotomized into positive and negative by combining the two negative ratings into a single negative rating and then doing the same with the two positive categories. Chi-squared analysis was used to assess statistical significance.
Table 2.
SOCIODEMOGRAPHIC DISTRIBUTION
| Subject’s gender | N | % | Parent’s gender | N | % |
|---|---|---|---|---|---|
| Male | 72 | 55 | Male | 7 | 5 |
| Female | 59 | 45 | Female | 124 | 95 |
|
| |||||
| Attended daycare | Parent’s race | ||||
|
| |||||
| No | 88 | 67 | African American | 48 | 37 |
| Yes | 43 | 33 | Caucasian | 69 | 53 |
|
| |||||
| Caries status | Other | 14 | 10 | ||
|
| |||||
| No | 72 | 55 | Parent’s education | ||
| Yes | 59 | 45 | Less than high school diploma | 23 | 18 |
|
| |||||
| Parenting style | High school diploma | 39 | 30 | ||
|
| |||||
| Authoritative | 87 | 66 | ≥1 y college | 69 | 52 |
| Permissive | 33 | 25 | Insurance type | ||
| Authoritarian | 11 | 9 | Private | 16 | 12 |
| Medicaid or no insurance | 115 | 88 | |||
|
| |||||
| Total | 131 | 100 | 131 | 100 | |
Parenting style and behavior
Authoritative parenting style accounted for 81 children (93 percent) with positive behavior and six children (seven percent) with negative behavior. Permissive parenting accounted for 19 children (58 percent) with positive behavior and 14 children (42 percent) with negative behavior. Authoritarian parenting accounted for five children (45 percent) with positive behavior and six children (55 percent) with negative behavior. Children with authoritative parents exhibited significantly more positive behavior (P<.001) versus children with authoritarian and permissive parents (Figure 1).
Figure 1.
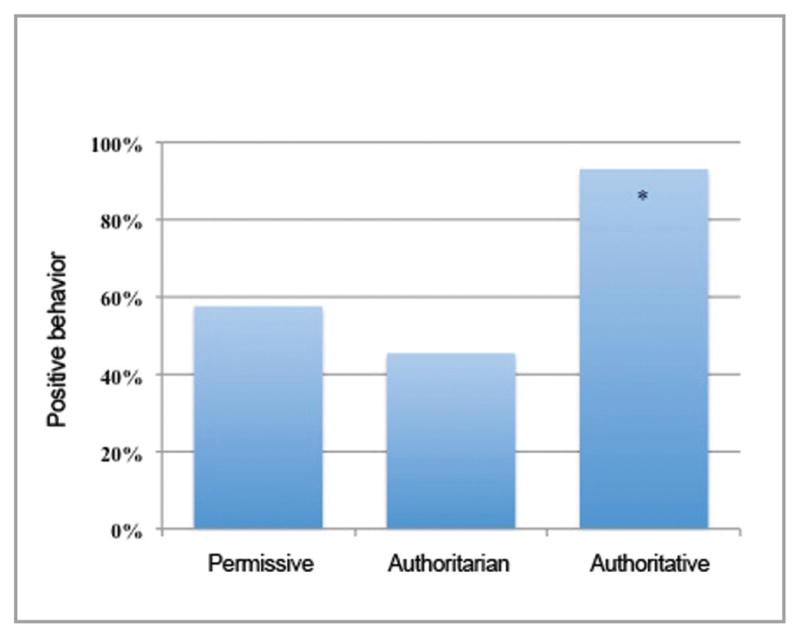
Percentage of children with positive behavior by parenting style
* Significant difference (P<.0001).
We were concerned that the age of the child could be a factor involved in this significant difference. Figure 2 shows the distribution of child behavior with the mean age listed for each behavior category. The prevalence of negative behavior was higher among three-to four-year-olds (25 percent negative behavior) compared to five-to six-year-olds (19 percent negative behavior), but the correlation between age and behavior was not statistically significant (P=.51).
Figure 2.

Behavior distribution with mean age and N value listed by category
* No significant difference (P=.51).
Parenting style and caries
Authoritative parenting accounted for 17 children (20 percent) with caries and 70 children (80 percent) without caries. Permissive parenting accounted for 32 children (97 percent) with caries and one child (three percent) without caries. Authoritarian parenting accounted for 10 children (91 percent) with caries and one child (nine percent) without caries. Children with authoritative parents had less caries (P<.001) compared to those with authoritarian and permissive parents.
Daycare, insurance, caries, and behavior
Forty-one children (98 percent) who attended daycare showed positive behavior at the dental office, while one child (one percent) did not. Of the children who did not attend daycare, 64 (72 percent) showed positive behavior while 25 (28 percent) showed negative behavior. Children who attended daycare exhibited more positive behavior compared to those children who did not (P<.001).
All children with private insurance (16 total) showed positive behavior, while none showed negative behavior. Eighty-nine children (77 percent) with Medicaid or no insurance showed positive behavior, while 26 (23 percent) showed negative behavior. Children with private dental insurance exhibited more positive behavior (P>.04) than those with Medicaid or no dental insurance.
Three children (19 percent) with private insurance had caries, while 13 children (81 percent) did not. Fifty-six children (49 percent) with Medicaid or no insurance had caries, while 59 children (51 percent) did not. Children with private dental insurance exhibited less caries (P>.02) versus those with Medicaid or no dental insurance.
Discussion
While anecdotal and popular press accounts relate parenting to behavior, this is one of the first studies to examine the correlation between parenting styles and the child’s behavior and caries in the dental office. A child’s personality and behavior are affected by numerous factors, and the immediate family environment seems to have the greatest impact on the child’s personality, development, and behavior.1–8,34 Current literature indicates that authoritative parenting has the most consistently positive impact on children. The current study found that authoritative parenting was associated with more desirable child behavior and less dental caries compared to the other two parenting styles. This is consistent with psychological research, which suggests that children in authoritative households have happier dispositions, greater emotional control and regulation, and improved social skills,18 all of which would suggest they would behave better at the dental office. This is also consistent with Aminabadi et al.’s finding that authoritative parenting was associated with improved child behavior compared to authoritarian and permissive parenting.30
We found that permissive parenting was associated with worse behavior and increased caries. This is consistent with current research, specifically Aminabadi’s finding that permissive parenting resulted in worse child behavior in the dental chair during a restorative dental visit.30 Permissive parents let a child make decisions, and the caregiver tries to keep the child happy, often with bribery.18 When put into the dental setting, the child can choose to misbehave, and the parent provides comfort without consequence or punishment. The increased caries in permissive households could be attributed to the fact that the child may be able to eat and drink cariogenic foods unabatedly and can also choose whether or not to brush teeth at home without expectation of discipline/enforcement.15,23
Our research indicated an association between authoritarian parenting and increased caries and less cooperative patient behavior in the dental office. This is consistent with Aminabadi et al., who found that authoritarian parenting results in less cooperative behavior during a restorative dental visit.30 Children in authoritarian homes often have difficulty in social situations and act fearful or shy around others, which could explain the poor behavior in the dental office.18 The increased caries in this group seems to contradict what would be suggested by typical authoritarian homes (i.e., strict rules). If strict rules were created to get children to brush teeth and adhere to a specific diet, then these children would abide by these rules. Our findings could suggest that oral health is not a priority for these families. Another possible explanation may be that oral hygiene and diet measures are not reinforced due to the low parental responsiveness exhibited in these households. The number of authoritarian households was limited in this study compared to authoritative and permissive households, and an increased sample size in a future study could help clarify these findings.
Our study also showed that private insurance was associated with better behavior and less dental caries compared to Medicaid. These results are consistent with the current literature, which reports increased caries prevalence35 and increased behavior problems in children with low socioeconomic status.36,37 It would have been interesting to assess parental history of caries to compare to socioeconomic status and child caries; it has been shown that parental history of caries is associated with early childhood caries.38
An interesting finding in our research was that daycare attendance was associated with better behavior. This contradicts current research, which suggests that increased time in daycare is negatively associated with social development, thus causing worse child behavior.39 For many preschool children, meeting new people (especially adults) may be difficult. This would be increasingly difficult if they were not used to interacting with people outside their family on a regular basis. Our findings suggest that early interaction with other children and adults at daycare may have a positive effect on their behavior at the dentist, perhaps because of an acquired ability to interact with strangers and adults.
A limitation of the study was that subjects represented a convenience sample of patients presenting to the dental clinic at Nationwide Children’s Hospital. Also, since the sample was small, only three main parenting styles were used to categorize the parenting. This led to exclusion of other potential styles conceptualized by psychologists, including neglectful. Another limitation was the potential selection bias: there were mostly authoritative parents (Table 2). However, this could be a normal distribution for our population; the studies similar to the present study do report a higher prevalence of the authoritative parenting style, but there is no study reporting a clear indication of the prevalence of each parenting style in the U.S.A.15 The high percentage of authoritative parents could be explained by the possibility that mostly authoritative parents bring their children to the dentist compared to the other parenting styles.
This would be an interesting topic to research further, correlating with other sociodemographic information. Approximately 80 percent of the children behaved positively at the first dental visit (Figure 2). This could be explained by the fact that this study used a noninvasive dental appointment. Older children showed a higher prevalence of positive behavior, which is consistent with previous research and intuition.1,40 An interesting future topic to research would be to note if there are differences in parenting styles, social data, and caries status of patients who arrive as walk-in emergencies versus those in the present study, who presented without pain for a routine first examination and cleaning.
Future research is needed to further investigate the relationship between parenting styles, child behavior, and caries in the pediatric dental setting. A large sample size from different populations would be beneficial to confirm this study’s results. Future research could complement the current study to develop a model for predictors of certain child behavior and oral health.
Conclusions
Based on this study’s results, the following conclusions can be made:
Authoritative parenting and private dental insurance were associated with less caries and better behavior during the first dental visit.
Attending daycare was associated with better behavior during the first dental visit
Acknowledgments
The project described was supported by Award Number Grant UL1TR001070 from the National Center For Advancing Transitional Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Advancing Transitional Sciences or the National Institutes of Health.
References
- 1.Allen KD, Hutfless S, Larzelere R. Evaluation of two predictors of child disruptive behavior during restorative dental treatment. J Dent Child. 2003;70:221–5. [PubMed] [Google Scholar]
- 2.American Academy on Pediatric Dentistry Clinical Affairs Committee. . Guideline on behavior guidance for the pediatric dental patient. Pediatr Dent. 2008;30(suppl):125–33. [PubMed] [Google Scholar]
- 3.Arnrup K, Broberg AG, Berggren U, Bodin L. Lack of cooperation in pediatric dentistry: the role of child personality characteristics. Pediatr Dent. 2002;24:119–28. [PubMed] [Google Scholar]
- 4.Baier K, Milgrom P, Russell S, Mancl L, Yoshida T. Children’s fear and behavior in private pediatric dentistry practices. Pediatr Dent. 2004;26:316–21. [PubMed] [Google Scholar]
- 5.Brill WA. The effect of restorative treatment on children’s behavior at the first recall visit in a private pediatric dental practice. J Clin Pediatr Dent. 2002;26:389–93. doi: 10.17796/jcpd.26.4.r1543673rx055355. [DOI] [PubMed] [Google Scholar]
- 6.Carey WB. Teaching parents about infant temperament. Pediatrics. 1998;102(suppl E):1311–6. [PubMed] [Google Scholar]
- 7.Klingberg G, Broberg AG. Temperament and child dental fear. Pediatr Dent. 1998;20:237–43. [PubMed] [Google Scholar]
- 8.Rud B, Kisling E. The influence of mental development on children’s acceptance of dental treatment. Scand J Dent Res. 1973;81:343–52. doi: 10.1111/j.1600-0722.1973.tb00337.x. [DOI] [PubMed] [Google Scholar]
- 9.Gustafsson A, Broberg A, Bodin L, Berggren U, Arnrup K. Dental behaviour management problems: the role of child personal characteristics. Int J Paediatr Dent. 2010;20:242–53. doi: 10.1111/j.1365-263X.2010.01046.x. [DOI] [PubMed] [Google Scholar]
- 10.Klingberg G, Berggren U. Dental problem behaviors in children of parents with severe dental fear. Swed Dent J. 1992;16:27–32. [PubMed] [Google Scholar]
- 11.Baumrind D. Parental disciplinary patterns and social competence in children. Youth Soc. 1978;9:239–251. [Google Scholar]
- 12.DeVore ER, Ginsburg KR. The protective effects of good parenting on adolescents. Curr Opin Pediatr. 2005;17:460–5. doi: 10.1097/01.mop.0000170514.27649.c9. [DOI] [PubMed] [Google Scholar]
- 13.Dornbusch SM, Ritter PL, Leiderman PH, Roberts DF, Fraleigh MJ. The relation of parenting style to adolescent school performance. Child Dev. 1987;58:1244–57. doi: 10.1111/j.1467-8624.1987.tb01455.x. [DOI] [PubMed] [Google Scholar]
- 14.Lamborn S, Mounts N, Steinberg L, Dornbusch S. Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Dev. 1991;62:17. doi: 10.1111/j.1467-8624.1991.tb01588.x. [DOI] [PubMed] [Google Scholar]
- 15.Law CS. The impact of changing parenting styles on the advancement of pediatric oral health. J Calif Dent Assoc. 2007;35:192–7. [PubMed] [Google Scholar]
- 16.Rytkonen K, Aunola K, Nurmi J. Parents’ causal attributions concerning their children’s school achievement: a longitudinal study. Merrill-Palmer Q. 2005;51:20. [Google Scholar]
- 17.Cohen DA, Rice J. Parenting styles, adolescent substance abuse, and academic achievement. J Drug Educ. 1997;27:199–211. doi: 10.2190/QPQQ-6Q1G-UF7D-5UTJ. [DOI] [PubMed] [Google Scholar]
- 18.Baumrind D. Current patterns of parental authority. Dev Psychol Monogr. 1971;4:1–103. [Google Scholar]
- 19.Bailey PM, Talbot A, Taylor PP. A comparison of maternal anxiety levels with anxiety levels manifested in the child dental patient. J Dent Child. 1973;40:277–84. [PubMed] [Google Scholar]
- 20.Robinson C, Mandleco B, Olsen SF, Hart CH. The parenting styles and dimensions questionnaire (PSDQ) Handb Fam Meas Tech. 2001;3:319–21. [Google Scholar]
- 21.Querido JG, Warner TD, Eyberg SM. Parenting styles and child behavior in African American families of preschool children. J Clin Child Adolesc Psychol. 2002;31:272–7. doi: 10.1207/S15374424JCCP3102_12. [DOI] [PubMed] [Google Scholar]
- 22.Casamassimo PS, Wilson S, Gross L. Effects of changing U.S. parenting styles on dental practice: perceptions of diplomates of the American Board of Pediatric Dentistry. Pediatr Dent. 2002;24:18–22. [PubMed] [Google Scholar]
- 23.Sheller B. Challenges of managing child behavior in the 21st century dental setting. Pediatr Dent. 2004;26:111–3. [PubMed] [Google Scholar]
- 24.O’Connor TM, Yang SJ, Nicklas TA. Beverage intake among preschool children and its effect on weight status. Pediatrics. 2006;118:e1010–e1018. doi: 10.1542/peds.2005-2348. [DOI] [PubMed] [Google Scholar]
- 25.Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–55. doi: 10.1001/jama.295.13.1549. [DOI] [PubMed] [Google Scholar]
- 26.Johnson R, Welk G, Saint-Maurice PF, Ihmels M. Parenting styles and home obesogenic environments. Int J Environ Res Public Health. 2012;9:1411–26. doi: 10.3390/ijerph9041411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Decaluwe V, Braet C, Moens E, Van Vlierberghe L. The association of parental characteristics and psychological problems in obese youngsters. Int J Obes (Lond) 2006;30:1766–74. doi: 10.1038/sj.ijo.0803336. [DOI] [PubMed] [Google Scholar]
- 28.Lopez NV, Ayala GX, Corder K, et al. Parent support and parent-mediated behaviors are associated with children’s sugary beverage consumption. J Acad Nutr Diet. 2012;112:541–7. doi: 10.1016/j.jand.2011.11.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Golan M, Crow S. Parents are key players in the prevention and treatment of weight-related problems. Nutr Rev. 2004;62:39–50. doi: 10.1111/j.1753-4887.2004.tb00005.x. [DOI] [PubMed] [Google Scholar]
- 30.Aminabadi NA, Farahani RM. Correlation of parenting style and pediatric behavior guidance strategies in the dental setting: preliminary findings. Acta Odontol Scand. 2008;66:99–104. doi: 10.1080/00016350802001322. [DOI] [PubMed] [Google Scholar]
- 31.Robinson C, Mandleco B. Authoritative, authoritarian, and permissive parenting practices: development of a new measure. Psychol Rep. 1995;77:1. [Google Scholar]
- 32.Klingberg G, Broberg AG. Dental fear/anxiety and dental behaviour management problems in children and adolescents: a review of prevalence and concomitant psychological factors. Int J Paediatr Dent. 2007;17:391–406. doi: 10.1111/j.1365-263X.2007.00872.x. [DOI] [PubMed] [Google Scholar]
- 33.Wright GZ, Stigers JI. McDonald and Avery’s Dentistry for the Child and Adolescent. 9. Maryland Heights, Mo: Mosby-Elsevier; 2011. Nonpharmacologic management of children’s behavior; pp. 27–40. [Google Scholar]
- 34.Darling N, Steinberg L. Parenting style as context: an integrative model. Psychol Bull. 1993;113:487–96. [Google Scholar]
- 35.Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988–1994. J Am Dent Assoc. 1998;129:1229–38. doi: 10.14219/jada.archive.1998.0420. [DOI] [PubMed] [Google Scholar]
- 36.Molnar BE, Cerda M, Roberts AL, Buka SL. Effects of neighborhood resources on aggressive and delinquent behaviors among urban youths. Am J Public Health. 2008;98:1086–93. doi: 10.2105/AJPH.2006.098913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Spencer N, Thanh TM, Seguin L. Low income/socioeconomic status in early childhood and physical health in later childhood/adolescence: a systematc reviw. Maten Child Health J. 2013;17(3):424–31. doi: 10.1007/s10995-012-1010-2. [DOI] [PubMed] [Google Scholar]
- 38.Thitasomakul S, Piwat S, Thearmontree A, Chankanka O, Pithpornchaiyakul W, Madyusoh S. Risks for early childhood caries analyzed by negative binomial models. J Dent Res. 2009;88:137–41. doi: 10.1177/0022034508328629. [DOI] [PubMed] [Google Scholar]
- 39.Belsky J, Vandell DL, Burchinal M, et al. Are there long-term effects of early child care? Child Dev. 2007;78:681–701. doi: 10.1111/j.1467-8624.2007.01021.x. [DOI] [PubMed] [Google Scholar]
- 40.Brill WA. Child behavior in a private pediatric dental practice associated with types of visits, age and socioeconomic factors. J Clin Pediatr Dent. 2000;25:1–7. doi: 10.17796/jcpd.25.1.545025p1g72x730q. [DOI] [PubMed] [Google Scholar]