
FIGURE 2.
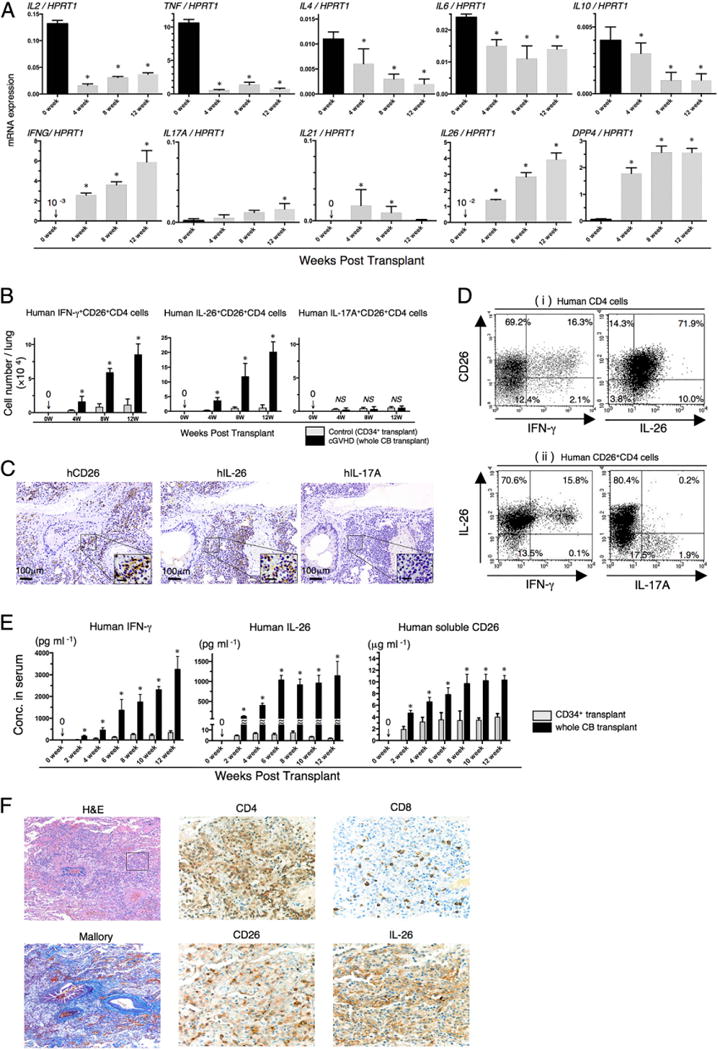
Predominant infiltration of IL-26+CD26+CD4 T cells in the lung of obliterative bronchiolitis. (A) Whole CB transplant mice were sacrificed at 4, 8, and 12 wk posttransplantation, and the lungs were removed, followed by isolation of human CD4+ cells. mRNA expression of human cytokines or CD26/DPP4 was quantified by real-time RT-PCR. Each expression was normalized to HPRT1. Data at 0 wk were obtained using freshly isolated HuCB CD4 T cells of three different donors. Data are cumulative results from three independent experiments (n = 10 at 4 wk, n = 8 at 8 wk, and n = 3 at 12 wk). *p < 0.0001 versus each at 0 wk. (B) Absolute cell numbers of human IFN-γ+CD26+CD4, IL-26+CD26+CD4, or IL-17A+CD26+CD4 cells in the lung of CD34+ transplant or whole CB transplant mice were quantified by flow cytometry. Data are cumulative results from three independent experiments (for each, n = 10 in CD34+ transplant group, and n = 10 at 4 wk, n = 8 at 8 wk, and n = 3 at 12 wk in whole CB transplant group). *p < 0.0001 versus corresponding CD34+ transplant group. (C) Anti-human CD26, IL-26, or IL-17A immunohistochemical staining of sequential sections of the lung from whole CB transplant mice (8 wk posttransplantation). The lung of whole CB transplant mice was clearly infiltrated with human CD26 or IL-26 (brown stained cells), but not with IL-17A–positive cells. Representative histology is shown from three independent experiments (n = 10). Original magnification ×100 or ×400 (inset in each panel). Scale bars in the inset, 20 μm. (D) Representative two-dimensional dot plots of human CD26 and IFN-γ or IL-26 cells by gating for human CD4+ cells (Di), and of human IFN-γ or IL-17A among IL-26+ cells by gating for human CD26+CD4+ cells (Dii). Single-suspension cells isolated from the lung of whole CB transplant mice (8 wk posttransplantation) were sorted by human CD45+ cells and then analyzed using flow cytometry. Numbers indicate relative percentages per quadrant. Similar results were observed in independent experiments (n = 10). (E) Sera of CD34+ transplant or whole CB transplant mice were collected at the indicated week posttransplantation, and serum levels of human IFN-γ, IL-26, and soluble CD26/DPP4 were quantified. Data are cumulative results from three independent experiments (for each, n = 10 in CD34+ transplant group, and n = 10 at 0–6 wk, n = 8 at 8 wk, n = 7 at 10 wk, and n = 3 at 12 wk in whole CB transplant group). *p < 0.0001 versus corresponding CD34+ transplant group. (F) H&E, Azan-Mallory, anti-human CD4, CD8, CD26, or IL-26 immunohistochemical staining of sequential sections of the lung from a patient undergoing alloPBSCT for ALL. After having acute skin GVHD on day +33 posttransplant, the patient experienced dyspnea with ground glass opacity detected on the chest X-ray examination on day +95. The lung specimen was obtained by transbronchial lung biopsy on day +101, showing perivascular and subepithelial inflammation and narrowing of the bronchiole (H&E staining). Peribronchiolar and perivascular collagen deposition was detected by Azan-Mallory staining. The lung was clearly infiltrated with CD4-, CD26-, or IL-26–positive cells (brown stained cells), with CD8-positive cells found at a very low level. The histology shown in immunohistochemical staining is focused in the inset of the H&E staining panel. Original magnification ×100 (H&E and Azan-Mallory) or ×400 (anti-CD4, CD8, CD26, and IL-26 staining).