

Abstract
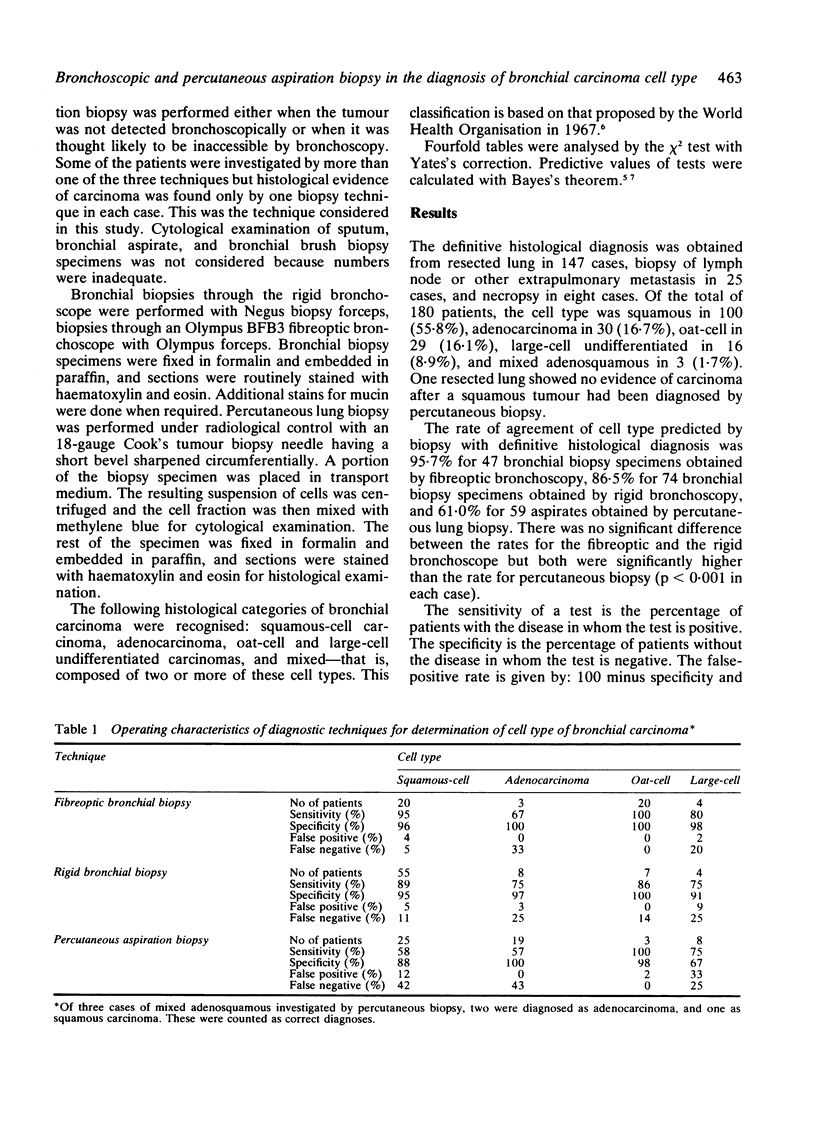
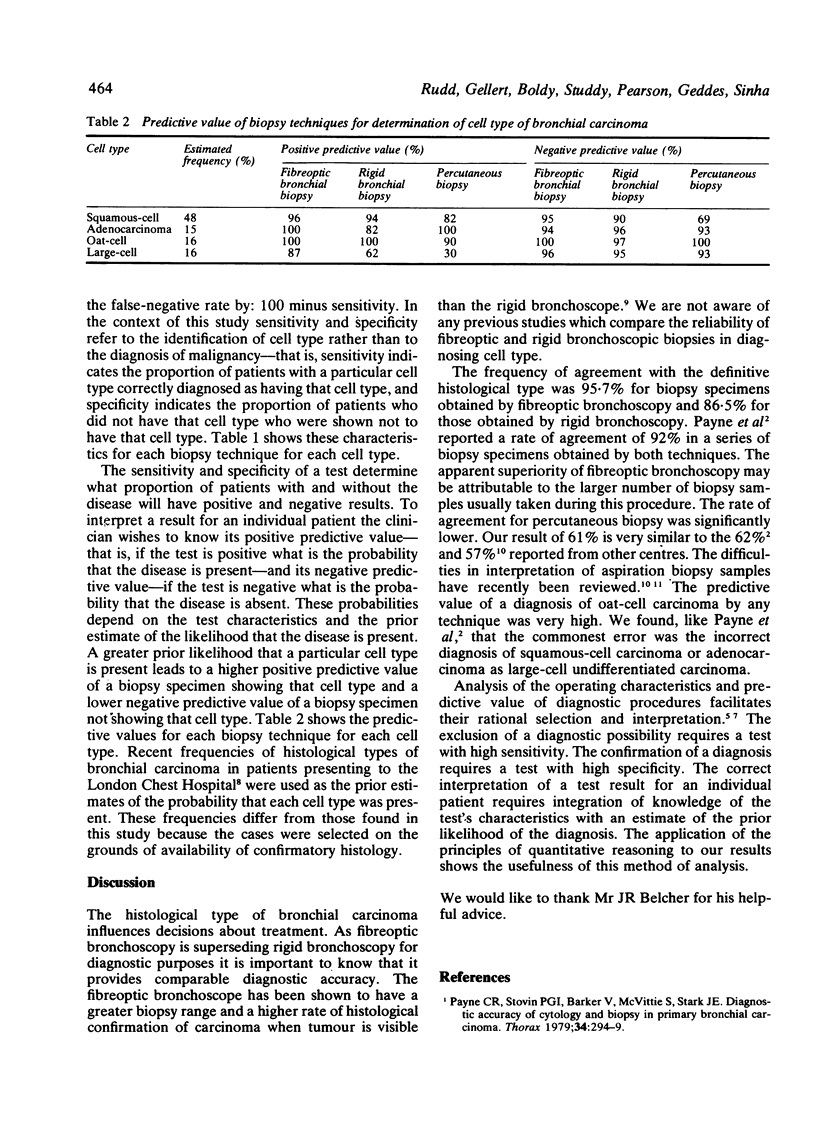
The cell type of bronchial carcinoma predicted from the results of bronchial biopsy at fibreoptic or rigid bronchoscopy or of percutaneous aspiration lung biopsy was compared with the type determined by histological examination of specimens obtained by thoracotomy, biopsy of an extrapulmonary metastasis, or necropsy in 180 cases. The rates of agreement with the final diagnosis were 95.7% for bronchial biopsy through the fibreoptic bronchoscope and 86.5% through the rigid bronchoscope. For percutaneous biopsy, which was usually carried out on tumours inaccessible to the bronchoscope, the rate of agreement was 61%, significantly lower than by the other methods (p less than 0.001). The diagnosis of oat-cell carcinoma by any technique was very reliable. Bronchial biopsy was more reliable than was percutaneous biopsy in diagnosing squamous-cell carcinoma. With any technique the commonest error was the incorrect diagnosis of squamous-cell carcinoma or adenocarcinoma as large-cell undifferentiated carcinoma.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Flower C. D., Verney G. I. Percutaneous needle biopsy of thoracic lesions--an evaluation of 300 biopsies. Clin Radiol. 1979 Mar;30(2):215–218. doi: 10.1016/s0009-9260(79)80166-x. [DOI] [PubMed] [Google Scholar]
- Greco F. A., Richardson R. L., Schulman S. F., Stroup S., Oldham R. K. Treatment of oat cell carcinoma of the lung: complete remissions, acceptable complications, and improved survival. Br Med J. 1978 Jul 1;2(6129):10–11. doi: 10.1136/bmj.2.6129.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNeil B. J., Keller E., Adelstein S. J. Primer on certain elements of medical decision making. N Engl J Med. 1975 Jul 31;293(5):211–215. doi: 10.1056/NEJM197507312930501. [DOI] [PubMed] [Google Scholar]
- Mountain C. F. Clinical biology of small cell carcinoma: relationship to surgical therapy. Semin Oncol. 1978 Sep;5(3):272–279. [PubMed] [Google Scholar]
- Payne C. R., Hadfield J. W., Stovin P. G., Barker V., Heard B. E., Stark J. E. Diagnostic accuracy of cytology and biopsy in primary bronchial carcinoma. J Clin Pathol. 1981 Jul;34(7):773–778. doi: 10.1136/jcp.34.7.773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Payne C. R., Stovin P. G., Barker V., McVittie S., Stark J. E. Diagnostic accuracy of cytology and biopsy in primary bronchial carcinoma. Thorax. 1979 Jun;34(3):294–299. doi: 10.1136/thx.34.3.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tao L. C., Pearson F. G., Delarue N. C., Langer B., Sanders D. E. Percutaneous fine-needle aspiration biopsy. I. Its value to clinical practice. Cancer. 1980 Mar 15;45(6):1480–1485. doi: 10.1002/1097-0142(19800315)45:6<1480::aid-cncr2820450630>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- Webb J., Clarke S. W. A comparison of biopsy results using rigid and fibreoptic bronchoscopes. Br J Dis Chest. 1980 Jan;74(1):81–83. [PubMed] [Google Scholar]