
Figure 4.
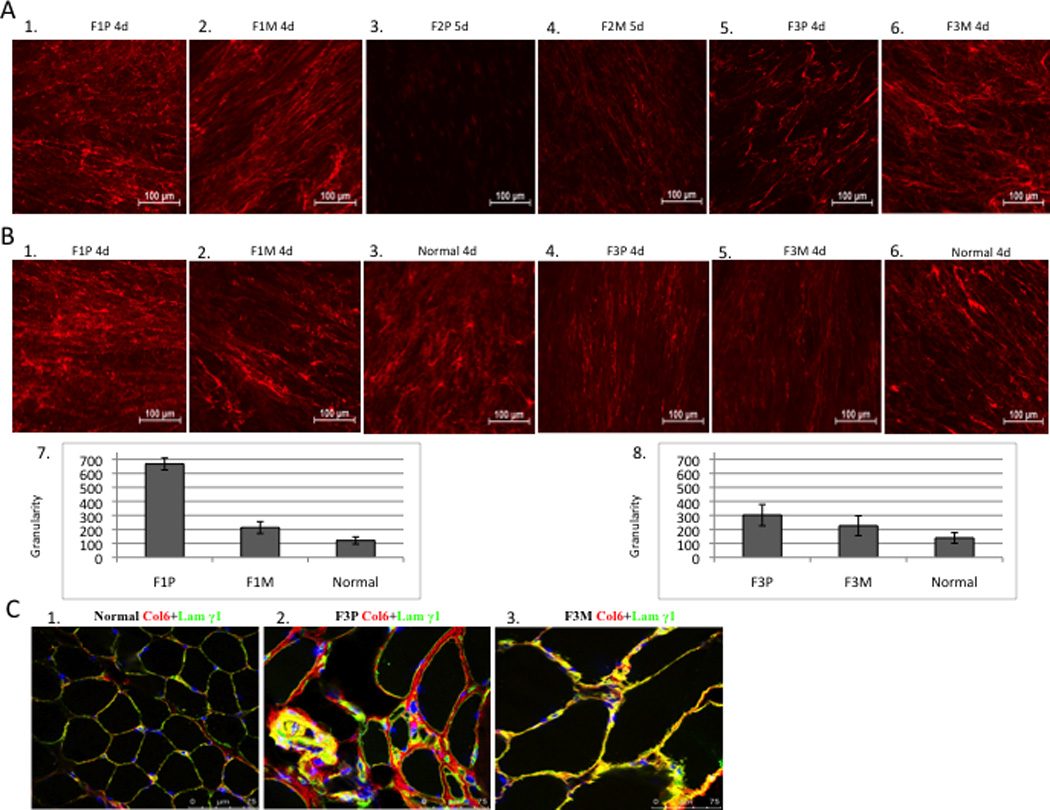
(A) Comparison of collagen VI immunoactivity in dermal fibroblast. (20x). Dermal fibroblasts were grown in the presence of 50ug/ml of L-ascorbic acid for 4-5 days after 80% confluency. Collagen VI specific monoclonal antibody was used (red). Collagen VI was detected in the extracellular matrix of mosaic parent and has a “knotted” and “speckled” pattern in the patient F1P (A1, A2), immunoreactivity is absent in patient F2P (A3, A4) and is reduced in patient F3P (A5, A6). (B) Granularity (quantitation of speckles) of the matrix deposited by fibroblasts was measured and normalized to the mean fluorescence intensity for Family 1 and 3, and normal controls processed concomitantly. Each bar graph represents the average of five images from independent fields of the same experiment. (C) Immunofluorescent staining of collagen VI in skeletal muscle (63x). Normal control muscle showed normal amount of collagen VI (red) with co-localization of basement membrane protein, laminin γ1 (green) resulting in yellow signal (C1); considerable amount of collagen VI in the matrix with partial co-localization of basement membrane protein in the patient’s muscle (see yellow), significant increased connective tissue (C2); mild increased connective tissue with normal amount of collagen VI and co-localization of basement membrane in the mosaic parent (C3).