
FIGURE 4.
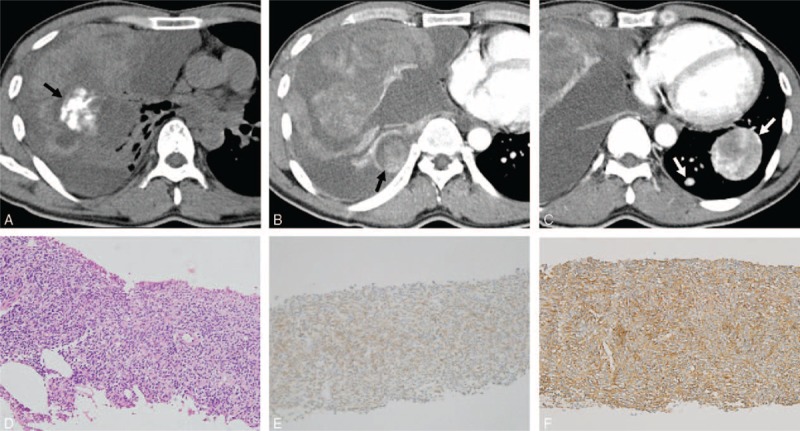
Computed tomography (CT) images obtained in a 35-year-old man with monophasic primary pulmonary synovial sarcoma. (A) Nonenhanced conventional transverse mediastinal CT image (3-mm thick) obtained at the level of the bronchus intermedius. The CT image shows amorphous calcification (black arrow in A) in the right middle lobe. (B and C) Contrast-enhanced conventional transverse mediastinal CT images (3-mm thick) obtained at the level of left atrial roof and at the level of inferior vena cava. The CT images reveal a 13.2-cm heterogenously enhancing mass with an internally cystic or necrotic portion, and an intratumoral vessel. Note the enhancing pleural-based nodule in the right lower hemithorax (black arrow in B), suggestive of ipsilateral pleural metastasis, and the tumor rupture with fluid effusion with high attenuation in the pleural space, indicating hemothorax. The CT image shows a heterogenously enhancing mass with an intratumoral vessel in the left lower lobe, and another small enhancing nodule (white arrows in C), suggestive of contralateral lung metastases. FDG PET shows an FDG-avid lung mass with a maxSUV of 3.7 (not shown). (D) Pathology after core-needle biopsy shows a cellular mass with spindle-shaped cells with hyperchromatic nuclei (hematoxylin–eosin stain, original magnification ×200). (E) The tumor cells are weakly diffusely positive for Bcl-2 by immunohistochemistry, supporting the diagnosis of synovial sarcoma (original magnification ×200). (F) The tumor cells are positive for CD99 by immunohistochemistry, supporting the diagnosis of synovial sarcoma (original magnification ×200). Bcl-2 = B-cell lymphoma-2, FDG PET = 18F-fluorodeoxyglucose positron emission tomography, maxSUV = maximum standardized uptake value.