

Abstract
Background:
Complete triceps tendon ruptures are relatively rare in the general population but slightly more prevalent in professional football. One prior study found 11 complete ruptures over a 6-season period.
Hypothesis:
Triceps ruptures occur more commonly in football linemen due to forced elbow flexion during an eccentric contraction and may occur more commonly with the increasing size and speed of professional players. Surgical repair allows full return to sports, but with a lengthy recovery time.
Study Design:
Case series; Level of evidence, 4.
Methods:
A search of the National Football League Injury Surveillance System (NFLISS) found a total of 37 triceps tendon ruptures requiring surgical repair from the years 2000 to 2009. Data were obtained for setting of injury, player position, activity causing injury, play type, time of game when injury occurred, height, weight, body mass index (BMI), and number of days lost from football.
Results:
There were 37 players requiring surgical repair for triceps tendon ruptures over the 10-season period. The average height, weight, and BMI of the players were 75 inches, 292 pounds, and 36.5 kg/m2, respectively. The majority of players were linemen (86%): 16 defensive, 15 offensive, and 1 tight end. The injury took place while blocking or being blocked in 29 players (78%) and while tackling or being tackled in 5 players (14%). Players missed an average of 165 days (range, 49-318 days) from football as a result of their injury and surgery.
Conclusion:
Triceps tendon tears requiring surgical repair are more common in professional football players than in the general population and are occurring more commonly than previously reported. Surgical repair allows return to play.
Clinical Relevance:
Our study identifies the rate of triceps tendon tears requiring repair in the NFL according to position, identifying which players may be most at risk for this injury.
Keywords: triceps, tendon, sports medicine, football
The triceps brachii consists of the long, lateral, and medial heads and is the primary extensor muscle for the elbow. The 3 heads arise from different points but converge toward insertion points on the olecranon. The long head arises from the infraglenoid tubercle of the scapula, while the medial head originates from the posterior surface of the distal humerus. The lateral head originates from the intermuscular septum and the lateral and posterior surface of the proximal humerus.
Injuries to the distal triceps tendon are extremely rare in the general population, with 1 study reporting that only 0.8% of 1104 tendon injuries reviewed involved the triceps.1,2 In the National Football League (NFL), however, these injuries are more common. Mair et al10 reported that between 1991 and 1996, 21 ruptures of the triceps tendon were reported in the NFL; 11 of these were complete ruptures, and 15 required surgical repair.
While muscle belly tears have been reported, a rupture of the distal triceps tendon at the insertion into the olecranon process is the most commonly reported pathology.4,14,16 Figure 1 shows a magnetic resonance image (MRI) of a triceps rupture. The insertional anatomy of the brachii tendon has been recorded in cadaveric and radiologic studies to improve surgical repair and prevent triceps insufficiency as a postsurgical complication.7,9,15 In a cadaveric study of 36 elbows, Keener et al7 found that the lateral expansion of the insertion had a mean width of 16.8 mm, while the mean width of the triceps tendon proper was 23.7 mm at the olecranon tip. The lateral expansion was found to insert distally into the radial aspect of the proximal ulna and was continuous with the antebrachial fascia and the fascia of the anconeus muscle. The medial head inserts along the ulnar crest and into the medial aspect of the olecranon without expansion.
Figure 1.
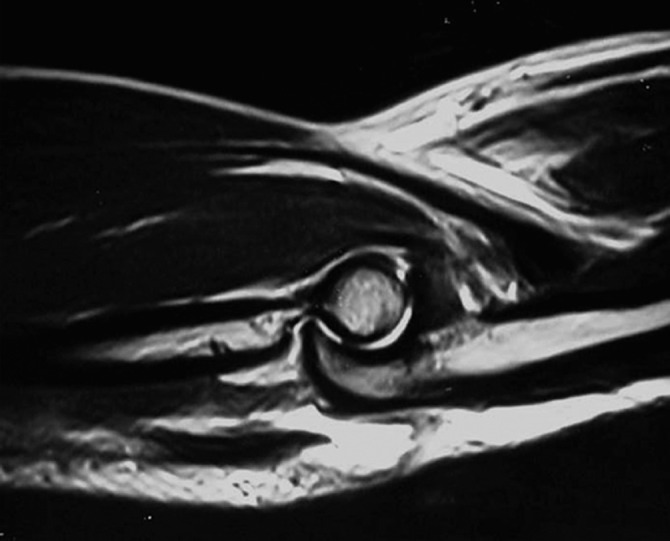
Sagittal magnetic resonance image of triceps rupture. Image reprinted with permission from Stucken and Ciccotti.14
Anabolic steroids, local corticosteroid injections, renal dialysis, systemic lupus erythematosus, and hyperparathyroidism have all been described as risk factors for tendon rupture.8,11,12 Other previously described mechanisms for triceps tendon rupture include a direct blow to the posterior aspect of the elbow and weight lifting.3,12,13
Our hypothesis is that triceps tendon ruptures occur more commonly in NFL players than in the general population because of the prevalence of actions that could cause forced elbow flexion during an eccentric contraction. We further hypothesize that triceps tendon rupture may occur more commonly in these NFL athletes due to their increased size and speed. The purpose of this study was to report epidemiological characteristics of players who suffered triceps ruptures requiring surgical repair and to assess whether surgical repair of triceps ruptures allows athletes to return to their previous level of play in the NFL.
Methods
Approval from the NFL was obtained prior to a query of the National Football League Injury Surveillance System (NFLISS). A search of the NFLISS was carried out by identifying players who were treated surgically for triceps tendon injuries. A total of 37 triceps tendon ruptures requiring surgical repair were identified over a 10-season period from 2000 to 2009. Data were obtained for setting of injury, player position, activity causing injury, play type, time of game when injury occurred, height, weight, body mass index (BMI), and number of days lost from football. A descriptive analysis of these data was then carried out. Players with nonoperative treatment of triceps tendon injuries were excluded from the study.
Results
Thirty-seven NFL players required surgical repair for triceps tendon ruptures over the 10-season period (Table 1). The average height, weight, and BMI of the players were 75 inches, 292 pounds, and 36.5 kg/m2, respectively.
TABLE 1.
All Reported Repaired Triceps Injuries in the NFL 2000-2009a
| Season | Session | Position | Player Activity | Team Activity | Quarter | Days Lost | BMI, kg/m2 |
|---|---|---|---|---|---|---|---|
| 2000 | Practice | Defensive line | Tackling | Rushing | Third | 183 | 36.6 |
| Game | Running back | Tackled | Passing | First | 64 | 31.9 | |
| Practice | Defensive line | Tackling | Rushing | Third | 183 | 36.6 | |
| 2001 | Practice | Defensive line | Blocked | Practice conditions | Fourth | 242 | 33.5 |
| 2002 | Game | Defensive line | Blocked | Passing | Third | 205 | 32.9 |
| Game | Offensive line | Blocking | Passing | Third | 73 | 40.0 | |
| 2003 | Practice | Offensive line | Blocking | Practice conditions | First | 318 | 40.1 |
| Practice | Special teams | Other, noncontact | Practice conditions | NR | 105 | 33.2 | |
| Game | Running back | Tackled | Passing | Second | 49 | 30.4 | |
| 2004 | Practice | Defensive line | Blocked | Practice conditions | Second | 234 | 31.7 |
| Game | Defensive line | Collision, other | Game conditions | First | 162 | 40.8 | |
| Game | Linebacker | Blocked | Rushing | Fourth | 157 | 31.4 | |
| Game | Offensive line | Blocking | Passing | First | 156 | 41.2 | |
| Game | Offensive line | Blocking | Passing | Fourth | 133 | 40.2 | |
| 2005 | Practice | Offensive line | Blocking | Practice conditions | Fourth | 189 | 30.8 |
| Practice | Defensive line | Blocked | Rushing | Fourth | 168 | 34.7 | |
| Game | Defensive line | Blocked | Game conditions | First | 158 | 39.1 | |
| 2006 | Game | Offensive line | Blocking | Game conditions | Second | 256 | 45.0 |
| Game | Offensive line | Blocking | Passing | Second | 183 | 37.6 | |
| Game | Offensive line | Blocking | Rushing | Fourth | 181 | 41.2 | |
| Game | Defensive line | Blocked | Passing | Third | 176 | 31.2 | |
| 2007 | Practice | Offensive line | Blocking | Practice conditions | Fourth | 205 | 38.2 |
| Game | Offensive line | Blocking | Not specified | First | 196 | 37.5 | |
| Game | Defensive line | Blocked | Passing | Fourth | 184 | 31.2 | |
| Game | Defensive line | Other | Not specified | First | 148 | 34.0 | |
| Game | Tight end | Blocking | Passing | Second | 133 | 30.9 | |
| Game | Defensive line | Blocked | Passing | Third | 120 | 40.7 | |
| 2008 | Game | Offensive line | Blocking | Rushing | Fourth | 211 | 35.3 |
| Game | Offensive line | Blocking | Not specified | Fourth | 144 | 38.9 | |
| Game | Defensive line | Blocked | Passing | Third | 125 | 35.2 | |
| Practice | Defensive line | Blocked | Passing | Second | 116 | 46.8 | |
| 2009 | Practice | Offensive line | Blocking | Practice conditions | First | 238 | 38.7 |
| Game | Offensive line | Blocking | Passing | Second | 181 | 38.2 | |
| Practice | Linebacker | Blocked | Rushing | Second | 176 | 31.2 | |
| Game | Defensive line | Tackling | Rushing | Fourth | 139 | 38.1 | |
| Game | Offensive line | Blocking | Game conditions | Second | 133 | 37.5 | |
| Game | Defensive line | Blocked | Passing | Second | 99 | 35.2 |
aBMI, body mass index; NFL, National Football League; NR, not reported.
Injury occurred during the game in 25 of 37 players (68%). The majority of the players were linemen (86%): 16 defensive, 15 offensive, and 1 tight end. Of the 5 nonlinemen, there were 2 linebackers, 2 running backs, and 1 special teams player. The injury took place while blocking or being blocked in 29 players (78%) and while tackling or being tackled in 5 players (14%).
During games, 13 injuries occurred in the first half (first quarter, 6; second quarter, 7) and 12 occurred in the second half (third quarter, 5; fourth quarter, 7). Players missed an average of 165 days (range, 49-318 days) from football as a result of their injury, subsequent surgery, and postoperative rehabilitation. All players returned to professional play in the NFL.
Discussion
Historically, triceps tendon ruptures have been reported as a rare occurrence.2 Triceps tendon ruptures usually occur because of forced elbow flexion during an eccentric contraction.3,10,12,13 These ruptures may occur more commonly in NFL athletes than in the general population because this mechanism is ubiquitous in football. Mair et al10 identified NFL lineman as an at-risk population.
In our review of triceps tendon ruptures over a 10-season period, 37 players required surgical repair, supporting our hypothesis that triceps tendon ruptures are not only common in football linemen but also found in various other positions in the NFL. These positions include running back, linebacker, tight end, and special teams. The majority of injuries occurred during blocking or being blocked, indicating that any player who engages in this type of action may be at increased risk for triceps injury.
The average height, weight, and BMI of the players were 75 inches, 292 pounds, and 36.5 kg/m2, respectively. The increased size of the NFL players, as seen in our study, compared with the average athlete may be indicative of a trend toward increased risk of triceps tendon ruptures in larger athletes. Presumably, players with increased speed and mass generate more eccentric force, which may result in an increased rate of triceps rupture. We cannot definitively correlate increased BMI with risk for triceps rupture since these players are already at risk because of their position on the team. The results of our study, however, warrant further investigation into the relationship between increased size and risk of triceps injury.
Surgical repairs aim to reinsert the distal tendon into the olecranon process. Our study cannot report the type of repair for these players, but the current gold standard for triceps tendon repair and the preferred surgical technique among our authors is the transosseous cruciate repair. In this type of repair, sutures are placed in the tendon through cruciate drill holes that cross within the olecranon. The sutures are then tied over the outside of the bone (Figures 2 and 3). While research on triceps tendon repair is limited due to the rarity of the injury, several studies have reported favorable outcomes with this technique. Few studies have examined clinical outcome after triceps repair with validated scores, but 1 case study of 5 patients undergoing triceps tendon repair with suture anchors showed excellent elbow function based on multiple validated scores.4
Figure 2.
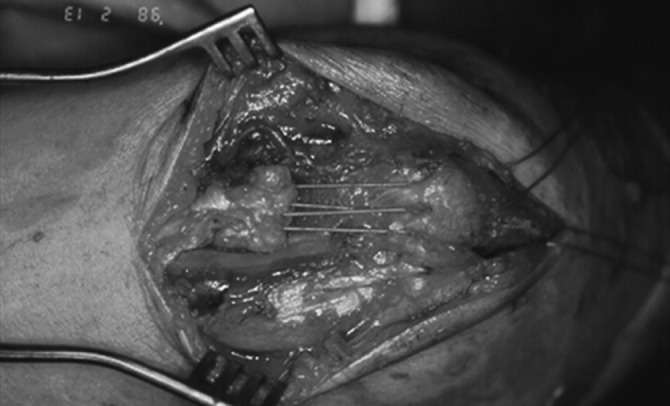
Sutures passed from stump of triceps tendon through olecranon tunnels. Image reprinted with permission from Stucken and Ciccotti.14
Figure 3.

Completed triceps repair. Image reprinted with permission from Stucken and Ciccotti.14
New surgical techniques have focused on re-creating the anatomic footprint of the triceps tendon insertion and using suture anchors or double-row techniques to increase the strength of the repaired tendon. In a recent cadaveric study comparing biomechanical results, Clark et al6 found that knotless anatomic footprint repair (using 1 suture anchor) resulted in less displacement and higher load and cycle to failure than transosseous cruciate repair. Further research is warranted to compare different surgical techniques.
While surgical repair allows return to the NFL, the injury likely requires the player to miss the current season for an in-season injury and potentially an additional season. These results are consistent with Mair et al,10 who did not report specific days of football lost, but 10 of 11 players who underwent early surgical repair missed the remainder of the season, and 1 player returned to play 7 weeks postoperatively. Players in our study missed an average of 165 days (range, 49-318 days) from football as a result of their injury and surgery. All players in the study by Mair et al10 with surgically repaired triceps tendon ruptures returned to play for at least 1 season of professional football, with the exception of 1 player who retired. Our study results further show that players are able to return to professional football, as all players in our study group returned to their preinjury level of sport.
Our study has some limitations. Because of protected health information, we were not able to discern the players’ ages or years of professional experience prior to injury. Also, we were not able to personally review the MRIs or operative reports of the involved players since our study was a retrospective review of the NFL database. The surgical procedures were performed by multiple physicians. Our review illustrates that there was a high rate of successful return after triceps repair in this population. We were not able to review functional scores after surgery or assess whether each player returned to the same degree of preoperative performance.
Furthermore, our study was unable to identify whether NFL players who experienced triceps ruptures had a local corticosteroid injection, which has been widely reported to be a risk factor.5,12,13 Stannard and Bucknell13 described a power-lifting soldier who had a triceps tendon rupture after being treated with multiple corticosteroid injections for olecranon bursitis. Sollender et al12 reported a case study of 4 weightlifters who suffered triceps tendon ruptures; 2 of the 4 received local steroid injections for pain in the triceps, and all 4 had taken oral anabolic steroids before injury.
Clayton and Thirupathi5 suggested that patients with chronic olecranon bursitis may be at risk for triceps tendon rupture. The NFL database does not include the number of players with a previous injection prior to triceps rupture. Therefore, no relationship between prior corticosteroid injection and triceps injury could be determined in our study. We believe, however, that identification of the incidence rate of triceps ruptures and the fact that almost all of these injuries occurred while blocking or being blocked in players with increased BMI is a valuable finding despite this limitation.
The strength of our study is that it represents the largest and longest review of NFL players with operative treatment of triceps tears. Our review, which included 37 triceps tendon ruptures requiring surgical repair, was conducted over a 10-year time period from 2000 to 2009, as compared with the study by Mair et al,10 which included 15 surgical cases over a 6-year time period conducted from 1991 to 1996. Our study shows a higher rate of these injuries than previously reported. Furthermore, our focus on increased BMI and the activity of blocking indicates that players other than linemen may be at risk during particular activities.
Conclusion
Triceps tendon tears requiring repair are more prevalent in professional football players than previously reported and are more common than in the general population.2,10 Our analysis included information on the action during which injury occurred and suggests that other positions besides linemen in which the players have higher BMIs and engage in frequent blocking may also be at increased risk. Surgical repair allows return to play; however, the injury likely requires the player to miss the current and potentially an additional season.
Footnotes
Declaration of Conflicting Interests: The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Anderson RL. Traumatic rupture of the triceps tendon. J Trauma. 1979;19:134. [DOI] [PubMed] [Google Scholar]
- 2. Anzel SH, Covey KW, Weiner AD, Lipscomb PR. Disruption of muscles and tendons; an analysis of 1,014 cases. Surgery. 1959;45:406–414. [PubMed] [Google Scholar]
- 3. Bach BR, Jr, Warren RF, Wickiewicz TL. Triceps rupture. A case report and literature review. Am J Sports Med. 1987;15:285–289. [DOI] [PubMed] [Google Scholar]
- 4. Bava ED, Barber FA, Lund ER. Clinical outcome after suture anchor repair for complete traumatic rupture of the distal triceps tendon. Arthroscopy. 2012;28:1058–1063. [DOI] [PubMed] [Google Scholar]
- 5. Clayton ML, Thirupathi RG. Rupture of the triceps tendon with olecranon bursitis. A case report with a new method of repair. Clin Orthop Relat Res. 1984;184:183–185. [PubMed] [Google Scholar]
- 6. Clark J, Obopilwe E, Rizzi A, et al. Distal triceps knotless anatomic footprint repair is superior to transosseous cruciate repair: a biomechanical comparison. Arthroscopy. 2014;30:1254–1260. [DOI] [PubMed] [Google Scholar]
- 7. Keener JD, Chafik D, Kim HM, Galatz LM, Yamaguchi K. Insertional anatomy of the triceps brachii tendon. J Shoulder Elbow Surg. 2010;19:399–405. [DOI] [PubMed] [Google Scholar]
- 8. Lambert MI, St Clair Gibson A, Noakes TD. Rupture of the triceps tendon associated with steroid injections. Am J Sports Med. 1995;23:778. [DOI] [PubMed] [Google Scholar]
- 9. Madsen M, Marx RG, Millett PJ, Rodeo SA, Sperling JW, Warren RF. Surgical anatomy of the triceps brachii tendon: anatomical study and clinical correlation. Am J Sports Med. 2006;34:1839–1843. [DOI] [PubMed] [Google Scholar]
- 10. Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med. 2004;32:431–434. [DOI] [PubMed] [Google Scholar]
- 11. Preston FS, Adicoff A. Hyperparathyroidism with avulsion of three major tendons. Report of a case. N Engl J Med. 1962;266:968–971. [DOI] [PubMed] [Google Scholar]
- 12. Sollender JL, Rayan GM, Barden GA. Triceps tendon rupture in weight lifters. J Shoulder Elbow Surg. 1998;7:151–153. [DOI] [PubMed] [Google Scholar]
- 13. Stannard JP, Bucknell AL. Rupture of the triceps tendon associated with steroid injections. Am J Sports Med. 1993;21:482–485. [DOI] [PubMed] [Google Scholar]
- 14. Stucken C, Ciccotti M. Distal biceps and triceps injuries in athlete. Sports Med Arthrosc Rev. 2014;22:153–163. [DOI] [PubMed] [Google Scholar]
- 15. Tagliafico A, Gandolfo N, Michaud J, Perez MM, Palmieri F, Martinoli C. Ultrasound demonstration of distal triceps tendon tears. Eur J Radiol. 2011;81:1207–1210. [DOI] [PubMed] [Google Scholar]
- 16. van Riet RP, Morrey BF, Ho E, O’Driscoll SW. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am. 2003;85:1961–1967. [DOI] [PubMed] [Google Scholar]