
Fig. 1.
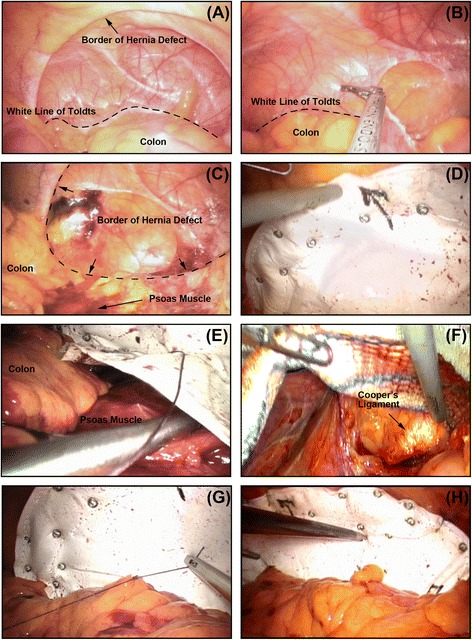
Keynotes for TAPE technique. a The operative field was overviewed: the white line of Toldt (dotted line) and the hernia defect was recognized; (b) the colon was mobilized by opening the peritoneal reflection above the white line of Toldt (dotted line); (c) After the colon was retracted, the extra-peritoneal space was dissected and exposed posteriorly until the psoas muscle, while the posterior border of the defect were also recognized; (d) A expanded polytetrafluoroethylene mesh large enough to overlap 4–5 cm onto the normal fascia was implanted and “partial-double-crown” technique was enrolled; (e) After overlapped with the psoas muscle, the posterior edge of the mesh was extra-peritoneally overlapped and fixed to the psoas muscle by interrupted sutures; (f) The dissection was extended and the mesh was fixed to the Cooper’s ligament when the inferior margin of the defect was beyond the iliac crest; (g) Through interrupted sutures, the colon can be restored to natural anatomical position; (h) An overview when finishing repair: the mesh was implanted posteriorly into extra-peritoneal space and anteriorly into peritoneal cavity, i.e., partial extra-peritoneal position