

Abstract
Background
Radiofrequency ablation (RFA) is an established but expensive treatment alternative for many forms supraventricular tachycardia (SVT). Currently no studies exist on the cost-effectiveness of RFA compared to medical treatment (MT) in adult Latin American population.
Methods
Between 2007 and 2012, we identified 103 adults who underwent RFA for SVT in the National Unit of Cardiovascular Surgery (UNICAR) in Guatemala. A decision tree was developed with all clinical outcome parameter estimates obtained from the Adult Electrophysiology Clinic. Costs were obtained from UNICAR's administration. A cost-effectiveness analysis was conducted which evaluated costs and quality adjusted life years (QALYs) to compare interventions in terms of their incremental cost-effectiveness ratios (ICERs).
Results
The first RFA had 83% success and cumulative 94% success was achieved with a second one. The cost of the RFA procedure itself was $5,411. RFA gains 1.46 QALYs and saves $ 7,993 compared to of MT for patients with SVT. This demonstrates that in Guatemala, RFA dominates MT in the management of SVT. Using assumptions based largely on the outcomes in UNICAR, we found that the RFA is highly cost-effective. This is a consistent finding, even after varying assumptions about efficacy, complication rates and quality of life.
Conclusions
RFA dominates MT by improving quality of life and reducing expenditures when used to treat severely symptomatic patients with SVT in Guatemala. The robustness of these finding to variations in parameter assumptions, suggests these findings may hold in other similar settings.
Keywords: Cost-effectiveness, cost-utility, supraventricular tachycardia, radiofrequency ablation
1. Introduction
Supraventricular tachycardias (SVT) are a group of common rhythm disturbances. They represent the most common class of heart rhythm disorders requiring medical attention. Radiofrequency ablation (RFA) is an established but expensive treatment alternative for many forms of SVT.[1] Most cases of SVT are not life-threatening (with the exception of tachycardias for accessory pathway like Wolf-Parkinson-White[WPW]).[2] However, severely symptomatic patients have multiple episodes per year that require urgent medical intervention to terminate the arrhythmia; these episodes substantially diminish quality of life, therefore the goal of therapy is to improve the patient's quality of life.[3]
Calculated costs for RFA in pediatric population in Guatemala in 2005 were established to be US$ 1,405 for a first ablation and $1,668 for a second one, in case of recurrence. The estimated cost of these ablations was demonstrated to be equal to that of continued MT after 5.1 years and 3.4 times less than MT after 20 years.[4] Nevertheless, currently no studies exist on an adult Latin American population.
Guatemala is a lower-middle income country with a gross domestic product per capita of $3478 in 2013 [5]. UNICAR (National Unit of Cardiovascular Surgery, by its acronym in Spanish) is the only public center with access to advance electrophysiology program in Guatemala, covering a population of 15,073,375 inhabitants.[6] Even though there is no published data about incidence of SVT in Guatemala, in an era where high-tech therapies are proliferating, it is necessary to examine whether these expenses are reasonable, especially in centers and countries with limited resources and different cultural acceptance.[4]
Previous studies [7,8] have used decision modeling to show that in patients with SVT who are highly symptomatic or have monthly episodes of arrhythmia, RFA is more effective and less expensive than long-term drug therapy. In addition, ablation improved quality adjusted expected life years (QALYs) by 3.1 years, and reduced expenses by US$ 27,900. However, these studies are several decades old and focused on the United States. Although highly effective, with success rates greater than 90% in some centers, this procedure has moderate risk of complications and is relatively expensive. [3,7,8]
A limitation of these analyses is that data were gathered from major centers of reference, with highly specialized success rates that often do not represent the less experienced centers, which may differ in various degrees. Furthermore, the analysis was carried out considering only one treatment drug, when in clinical practice physicians usually prescribe various drugs, with prices very different from each other [7,8].
Therefore, the objectives of this study are to demonstrate the effectiveness of RFA for SVT in an adult population in Guatemala, and analyze the cost-effectiveness when compared to conventional MT.
2. Methods
2.1 Local Health Outcomes for RFA
We performed a retrospective study, in which we reviewed the charts of adult patients (older than 18 year-old), with SVT who live in Guatemala and had undergone an electrophysiology study (EPS) and RFA from January 2007 to April 2012. Using the data collection instrument, we gathered socio demographic data, diagnosis, ablation performed, health outcomes of the procedure (success and complication rates), number of follow up visits a year, MT undertaken and recurrence of the arrhythmia at 5 months and a year after the procedure (Table 1).
Table 1. Characteristics and Outcomes of Patients undergoing RFA in UNICAR from 2007 to 2012.
| Characteristic | SD | % | |
|---|---|---|---|
| Average Age at ablation | 35.78 years | 14.51 | |
| Clinical indication | |||
| SVT | 48 patients | 46.60% | |
| WPW + SVT | 47 patients | 45.63% | |
| Preexitation | 5 patients | 4.85% | |
| Auricular flutter | 2 patients | 1.94% | |
| Unifocal Auricular Tachycardia | 1 patient | 0.97% | |
| Number of visits preRFA | 2.44 visits | 1.01 | |
| Medical Treatment preRFA | |||
| No treatment | 29 patients | 28.15% | |
| One drug | 63 patients | 61.20% | |
| Propafenone | 36 patients | 34.95% | |
| Beta blocker | 14 patients | 13.60% | |
| Amiodarone | 6 patients | 5.83% | |
| Verapamil | 5 patients | 4.85% | |
| Digoxin | 1 patient | 0.97% | |
| Sotalol | 1 patient | 0.97% | |
| Two drugs | 11 patients | 10.70% | |
| Propafenone + amiodarone | 4 patients | 3.88% | |
| Propafenone + Beta blocker | 4 patients | 3.88% | |
| Propafenone + digoxine | 1 patient | 0.97% | |
| Propafenone + magnesium | 1 patient | 0.97% | |
| Propafenone + Verapamil | 1 patient | 0.97% | |
| Average Hospital Stay | 3.24 days | 0.31 | |
| Patients who required ICUa | 5 patients | 4.85% | |
| Average ICU Stay | 2.6 days | 0.87 | |
| Post ablation Diagnosis | |||
| WPW | 45 patients | 43.69% | |
| Classic AVRNT | 23 patients | 22.33 | |
| Hidden accessory pathway | 11 patients | 10.68 | |
| Double physiology of AV node without tachycardia induction | 10 patients | 9.71 | |
| AVRNT + AFib | 3 patients | 2.91 | |
| Atypical AVRNT | 2 patients | 1.94 | |
| Atrial Flutter | 2 patients | 1.94 | |
| Preexitation Syndrome + AFib | 2 patients | 1.94 | |
| Epicardic accessory pathway | 2 patients | 1.94 | |
| AFib | 1 patient | 0.97 | |
| Left and Right Auricular reentry | 1 patient | 0.97 | |
| Auricular Tachycardia | 1 patient | 0.97 | |
| Outcomes | |||
| RFA initially successful | 86 patients | 83.50% | |
| RFA failed | 17 patients | 16.50% | |
| MT | 5 patients | 4.86% | |
| 2nd RFA | 12 patients | 11.64% | |
| Success after second ablation | 97 patients | 94.17% | |
| Complications | 2 patients | 1.94% | |
| Hemodynamic instability | 1 patients | 0.97% | |
| Major Bleeding | 0 patients | 0.00% | |
| Vascular Injury* | 1 patient | 0.97% | |
| Complete Heart Block | 0 patient | 0.00% | |
| Death | 0 patients | 0.00% | |
| Average visits post RFA | 2.26 visits | 1.08 | |
| Medical Treatment post RFA | |||
| No treatment | 41 patients | 39.81% | |
| Aspirin | 30 patients | 29.13% | |
| Propafenone | 17 patients | 15.60% | |
| Beta blocker | 6 patients | 5.80% | |
| Aspirin + clopidogrel | 2 patients | 1.94% | |
| Amiodarone | 2 patients | 1.94% | |
| Propafenone + Beta blocker | 2 patients | 1.94% | |
| Amiodarone + Beta blocker | 1 patient | 0.97% | |
| Sotalol | 1 patient | 0.97% | |
| Propafenone + digoxin | 1 patient | 0.97% | |
lesion to the internal jugular vein
Afib: atrial fibrillation. AVRNT: atrioventricular reentry nodal tachycardia. ICU: Intensive care Unit. MT: Medical Treatment. RFA: Radiofrequency ablation. SVT: supraventricular tachycardia. WPW: Wolf-Parkinson-White.
A total of 269 patients participating in EPS were identified (Figure 1). Of these patients, 137 were pediatric cases and additional 29 of the remaining 132 adult EPS were excluded. The final sample was 103 patients. The patient demographics are presented in Table 1.
Figure 1. Patient Population.
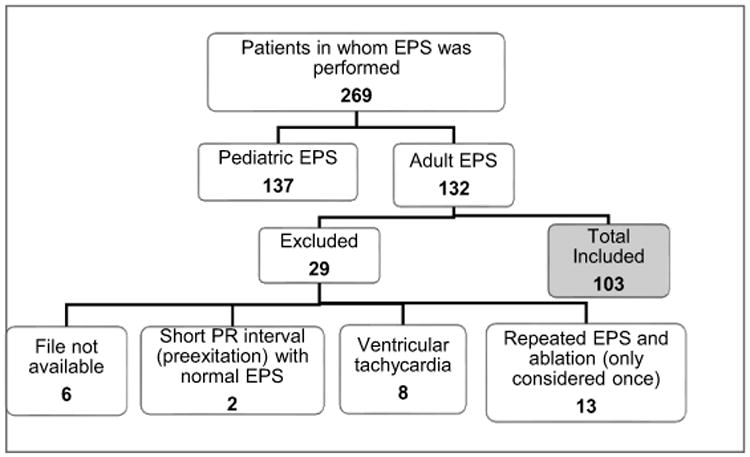
Distribution of study patients included in whom EPS was performed from August 2007 to April 2012. Follow up appointment and cardiac rhythm by EKG were evaluated until April 2013 to ensure no recurrence of the SVT. EPS= electrophysiological study
2.2 Decision Model Development
Using the available literature, outcomes and demographic data of the remaining 103 patients, we developed a decision tree using Microsoft Excel 2013. To create the model, we generated a hypothetical group of patients who underwent either MT or RFA. Patients entered a therapy-specific subtree that simulated the probability of success, recurrence of the SVT after the initial treatment and complication rates. The patients were considered to initiate in one arm of the tree, and move forward at the next appointment one year after. If the treatment was not successful, they would move to the next step on treatment (either adding new medication or undergoing RFA). By the end of the second year of the model, patients were considered stable in the treatment category they remained and the costs were calculated based on this (Figure 2).
Figure 2. Decision tree.

Patients entered a therapy-specific subtree that simulated the probability of success and recurrence of the SVT after the initial treatment. All the nonfatal complications were considered in patients with successful ablations. RFA: Radiofrequency ablation. SVT: supraventricular tachycardia.
We used the local data of the RFA procedure when possible, to include the probability of occurrence, complications, cost and quality of life associated with that outcome. If the probability for an event in the model was not observed in the local outcomes (for example, mortality), it was extrapolated from the published literature (Table 2), mainly from the studies of Hogenhuis [7], Carol [8], Calkins [13], Ikeda [15] and Bathina [16].
Table 2. Inputs used in the Decision Tree.
| Probabilities - Follow Up Events | Base Case | Utility [8,18] | Source - Reference | |
|---|---|---|---|---|
| Patients going on chronic MT | ||||
| Success with first drug (propafenone) | 60.00% | 0.833 | [7, 8, 10, 11, 15, 18] | |
| Success after second drug | 10.00% | 0.833 | Expert consensus, [15, 18] | |
| MT fails, goes to RFA | 29.00% | 0.983 | Expert consensus], [8,18] | |
| Patients entering RFA | ||||
| Success after first ablation | 83.48% | 0.983 | Outcomes in UNICAR, [8,15, 18] | |
| Recurrence after first ablation | 16.49% | Outcomes in UNICAR, [8, 18] | ||
| MT after recurrence | 4.85% | 0.833 | Outcomes in UNICAR, [8, 16, 18] | |
| Second ablation after recurrence | 11.64% | Outcomes in UNICAR | ||
| Success reached after 2nd ablation | 10.67% | 0.983 | Outcomes in UNICAR | |
| MT after 2nd ablation | 0.97% | 0.833 | Outcomes in UNICAR | |
|
| ||||
| Procedural complications | ||||
|
| ||||
| Death | 0.030% | 0 | UNICAR, [7, 13, 15, 19, 18] | |
| Nonfatal complications | 1.96% (0.015-3.0%) | UNICAR,[7, 13, 15,16,18] | ||
| Complete heart block | 0.49% | 0.776 | UNICAR, [7, 13, 15, 18] | |
| Hemodynamic Instability | 0.49% | 0.933 | UNICAR, [7, 13, 15, 18] | |
| Major Bleeding | 0.49% | 0.933 | UNICAR, [7, 13, 15, 18] | |
| Vascular injury | 0.49% | 0.933 | UNICAR, [7, 13, 15, 18] | |
|
| ||||
| Considerations | ||||
|
| ||||
| Patient appointments during the year of RFA | 2 | Outcomes in UNICAR | ||
| Patient outpatient appointments/year after RFA | 1 | Outcomes in UNICAR | ||
| Patient outpatient appointments/year after MT | 2 | Outcomes in UNICAR | ||
| Time horizon in years | 35 | |||
| Inflation Rate | 6% | |||
| Discount Rate | 12% | |||
| Days of ICU for Complete heart block | 1 | Outcomes in UNICAR | ||
| Days of ICU for Hemodynamic instability | 3 | Outcomes in UNICAR | ||
| Days of ICU for Major Bleeding | 2 | Outcomes in UNICAR | ||
| Days of ICU for Vascular Injury | 1 | Outcomes in UNICAR | ||
| Frequency of pacemaker replacement | 8 years | Outcomes in UNICAR | ||
|
| ||||
| Costs | ||||
|
| ||||
| Ablation Procedurea | $ 5,411.08 | UNICAR's administration | ||
| Floor Hospitalizationb | $ 340.22 | UNICAR's administration | ||
| Intensive Care Unit (ICU) day | $ 606.16 | UNICAR's administration | ||
| Bicameral Pacemaker placement | $ 2,355.85 | UNICAR's administration | ||
| Outpatient appointmentc | $ 44.46 | UNICAR's administration | ||
| Incremental cost of Procedural Complications | Complete Heart Blockd | $ 2,962.01 | UNICAR's administration | |
| Hemodynamic Instabilitye | $ 1818.48 | UNICAR's administration | ||
| Major Bleedingf | $ 1325.73 | UNICAR's administration | ||
| Vascular injuryg | $ 719.57 | UNICAR's administration | ||
| Yearly follow up on MT | Transport | $ 11.00 | ||
| Yearly treatment with propafenone | $ 992.31 | UNICAR's administration | ||
| Yearly propafenone + amiodarone | $ 1,249.23 | UNICAR's administration | ||
Basic cost includes ablation procedure
Includes floor bed (1 day), 1 EKG, analgesic post procedure, gastric protection with H2-blocker
Includes salaries of personnel and 1 EKG
Includes one day of ICU, placement of bicameral peacemaker, 2 appointments per year, exchange of device every 8 years.
Includes 3 days of ICU.
Includes 2 days of ICU care and 1 more day of floor stay.
Includes 1 more floor night and 1 ICU day
ICU: Intensive care unit. MT: Medical Treatment. RFA: Radiofrequency ablation.
The utilities were primarily extrapolated from the values used by Carol [8] and Larson [18] in their analysis. Larson obtained the utility retrospectively by evaluating highly symptomatic patients with SVT [18], so we considered that would be the best data for the utilities in our analysis. We assume the complications of hemodynamic instability, major bleeding and vascular injury were transient, and were considered resolved before the discharge. Patients who were assumed to get complete heart block had quality of life associated with pacemaker placement.
We considered a 35 years' timeframe because that is our sample average age subtracted from Guatemala's life expectancy.
2.2.1 Medical Treatment
Patients under drug therapy were assumed to receive a daily dose of propafenone. Although we recognized that more inexpensive drugs might be used in actual practice, our choice for the model was propafenone because is the drug that the majority of the patients use in UNICAR. Of every 100 patients in the MT arm, 60% would reduce symptoms with the MT,[7, 8, 9,10,11], 10% would need a second drug to be controlled and 30% would enter the ablation arm of the model. The episodic drug therapy (pill on the pocket strategy) was not included as it has been proven in previous studies to be inferior to long-term drug therapy for highly symptomatic patients [8]. The adverse effects of the medications reduced the life quality of life for the patients.
We did not include emergency department visits in neither strategy, because UNICAR does not offer that service.
2.2.2 Radiofrequency Ablation
We defined RFA as initially successful if the electrophysiologist could not induce an arrhythmia in the laboratory after the RFA. However, some patients in whom RFA is initially successful subsequently experience recurrent SVT, typically in the first few weeks after the procedure [8]. In the model, the patient visited the clinic 2 times the first year after the procedure, to assure that there was no recurrence. Patients were also switched to the MT arm if the arrhythmia was not ablatable or if the ablation was unsuccessful.
2.2.3 Efficacy and Complications
The efficacy and complication rate were extrapolated from the outcomes in UNICAR. Of the patients assigned to the RFA arm, 83.48% were presumed to have a successful ablation, 16.49% failed and 0.03% to have a fatal outcome. Regardless of the ablation success, 1.96% were estimated to have a nonfatal complication.
We assumed that patients in whom RFA was successful required no further antiarrhythmic medication. The incremental costs for each of the complications are described in the footnote of Table 2. A major bleeding episode was defined as an episode greater than type 3 bleeding in the definition proposed by Mehran and colleagues [12], including those that required blood transfusion, had at least a drop of hemoglobin of 3g/dl, cardiac tamponade, intracranial bleeding or fatal bleeding. Hemodynamic instability was defined as persistent hypotension despite fluid management.
If the probability for an event in the model was not observed in the local outcomes (for example, mortality), it was extrapolated from the published literature (Table 2).
In the case of a non-successful first ablation (16.49% of the RFA arm) 29.41% were estimated to enter MT (4.85% of the total fraction in the RFA arm) and the remainder had a second ablation. 91.67% of the second ablations were successful in leading to a total success rate of 94.15% after two ablations. We assumed the remainder who failed the second ablation had MT.
2.2.4 Costs
We calculated the all the costs based on the data in UNICAR's administration during 2012. The data was provided in the local currency (Quetzales), which had a conversion factor of 1US$ = 7.8Q in 2012. The basic cost of the RFA was $5,411.08 and the costs for each arm of the tree were calculated from this. To calculate the follow-up costs, we assumed two outpatient follow up visits in the first year, and then 1 outpatient appointments for patients in RFA arm (except for patients with complete heart block who get 2 yearly appointments) and 2 appointments for those in MT. The cost of each appointment was calculated with the salary of physicians and nurses, one EKG and the transport of the patient to UNICAR. We estimated a 6% annual inflation rate, using the average inflation rate in the last 20 years in Guatemala. The costs were discounted at a 12% nominal discount rate per year (6% real discount rate) because in the context of Guatemala that is a conservative rate. The discount and inflation rate were tested in sensitivity analysis.
2.3 Cost-effectiveness analysis
Therapies for non-life-threatening SVT by definition affect quality of life rather than length of life [8]. Because of this, we used quality adjusted life years (QALYs) to measure the effect of our model. In this methodology, different states of health can be associated with differences in quality of life (utilities). The utilities asses how patients value health states and typically range from 0 (representing death) to 1 (representing ideal health). Utilities differ from measures of functional status in that they assess how much health state bothers patients rather than describing the health state in terms of what patients can do. We assigned a “quality of life” for each state of health in the decision tree to reflect those utilities for each possible outcome [7,12]. Patients remaining in the well state for 1 year (utility of 1) were credited with 1 QALY, dead patients were credited with 0 and patients experiencing morbidity accumulate life-years at an intermediate rate.
2.3.1 Discounting
We considered that each patient entering the model would live additional 35 years which is the average life expectancy of Guatemalans minus the average age at ablation.
We calculated the expenses incurred in those 35 years of each arm of the model, and applied the concept of present value of future expenses. More details about discounting are presented in the Appendix.
2.3.2 Decision analysis, projections and sensitivity analysis
We calculated the expected costs and QALYs per patient treated medically or with RFA for SVT.
Then we calculated the incremental cost-effectiveness ratio (ICER) for RFA versus MT and calculated the net benefit of each intervention. The net benefit is a dollar value encompassing the financial and health value of the intervention (see details in the appendix). Finally, we performed one-way and probabilistic sensitivity analyses on the input parameters, to determine which variables had the largest impact on the results. The probabilistic sensitivity analysis was conducted with 10,000 iterations using input distributions presented in Appendix Table A.4.
3. Results
3.1 Local Outcomes in UNICAR
Table 1 presents the characteristics of study patients. There was an overall success of 83.48% with a first RFA and a cumulative 94.15% after a second RFA.
3.2 Costs
Based on data available at UNICAR, we calculated the basic cost of RFA at $ 5411.08. The details of expenses for each of the arms are explained in the footnote of Table 2. Because of long-term medications, the MT arm had $16,460 in discounted costs over 35 years. Although RFA had higher initial costs and some costs of complications, longer-term costs were lower because patients took fewer medications. The expected 35-year discounted costs of RFA were $8,467. Figure A.1 (Appendix) shows the cumulative average cost of RFA vs MT.
3.3 QALYs Calculation
Patients with successful RFA had improved quality-of-life. Table 3 shows expected outcomes under MT and RFA. Patients with MT had 13.49 expected discounted QALYs over 35 years, whereas RFA patients had 14.95 discounted QALYs over the same time period. There is a gain of 1.46 QALYs and a saving of $ 7,993 with the RFA treatment compared with MT, which represents a saving of $5480 per QALY gained. This demonstrates that RFA dominates MT in the management of SVT.
Table 3. Cost-Effectiveness Analysis.
| Total QALYs | Total Undiscounted Cost | Total Undiscounted QALYs | Discounted Costs | Discounted QALYs | ICER | Dominance | Net Benefit | Incremental Dollar Benefit of RFA vs. MT |
|---|---|---|---|---|---|---|---|---|
| Medical Treatment | $103,385.66 | 30.73 | $16,460.21 | 13.49 | Dominated | $ 30,469 | ||
| RFA | $19,658.33 | 34.05 | $8,466.76 | 14.95 | -$5,480.24 | Dominant | $ 43,536 | $13,066 |
ICER: Incremental cost-effectiveness ratio. MT: Medical Treatment. QALY: Quality Adjusted Life Years. RFA: Radiofrequency ablation.
We calculated the net benefit using the formula described in the appendix, to examine the dollar value of the therapy choice. This represents how much one might be willing to pay to have RFA instead of MT if one values QALYS at $3478 (per-capita GDP of Guatemala) over a 35-year timeframe. If QALYS are valued at that amount, then RFA provides $13,066 more in value than MT including the value of cost savings and health improvement.
We plotted the ICER per year to observe the trend of the cost-effectiveness in each year after the procedure (Figure A.2, Appendix).
3.4 Sensitivity Analysis
In addition to our base-case analyses, we performed one-way and probabilistic sensitivity analyses (Table A.4, Appendix) in which we systematically varied parameters between low and high values [8].
Figure 3 presents a tornado diagram displaying the results of key one-way sensitivity analyses on the net benefit for RFA compared with MT. The base-case incremental value of RFA over MT is $13,066.
Figure 3. Sensitivity Analysis.

Tornado diagram displaying the results of key one-way sensitivity analyses on the Change in Net Monetary Benefit of RFA over Medical Treatment. The vertical dotted line represents $13,066, the base-case incremental value of RFA over medical treatment. MT: Medical Treatment. RFA: Radiofrequency ablation.
Varying individual parameters within 20% (or extreme limits, if 20% was not possible), show the incremental value of RFA over MT in the horizontal bars. The net monetary value varies slightly, but RFA still always has a positive net monetary value over MT.
The probabilistic sensitivity analysis showed that RFA is highly likely to be cost-effective. There is a 78% chance of it being cost-saving and a 92% chance of having a cost-effectiveness ratio less than $3500 per QALY. Cost-effectiveness acceptability curves are shown in Figure A3.
4. Discussion
In the present study, we used a disease simulation model to project cost and quality-adjusted life expectancy for a population of 35-year-old patients with symptomatic SVT who were treated with either RFA or continued MT. Using assumptions based largely on the outcomes in UNICAR, we found that RFA is highly cost-effective, taking as a reference the guidelines of WHO-CHOICE (less than 1× GDP per capita) [14].
In Guatemala, the mean cost per RFA of SVT was $5,411.08, which is cheaper than that reported in other studies from developed nations, such as Australia, Japan, and the United States [4,7,14,15]. Even when including the costs of the second RFA (after an unsuccessful first attempt; 94.2% success rate), the cost still proved to be between 68.4 and 90.3% lower than reported in other countries [4,7,15,16]. This lower cost is due to the much lower salaries of medical, nursing, and technical personal in Guatemala. In addition, the use of resterilized material, such as ablation catheters, decreases the overall cost of the procedure by 66% [4]. When compared to the long-term costs of MT, RFA was almost $8000 less expensive. This indicates that our results are congruent with previous studies, including one from Guatemala in the pediatric population, showing that RFA dominates MT for the management of SVT, even in different contexts and with different assumptions. [3,4,7,8,9,16].
The model we developed predicts that in patients with SVT, RFA yields a quality-adjusted life expectancy greater than MT. Our findings support the usual international practice of initially performing RFA in patients with highly symptomatic SVT. This benefit overcomes the low risk of mortality or nonfatal complications during the procedure.
Our analysis confirms the financial benefits of RFA, particularly with long-term follow-up, due to the elimination of anti-arrhythmic medications and the avoidance of subsequent ICU and hospital stays for SVT recurrences.
According to our results, RFA proved effective for patients with drug refractory symptoms as well as frequent arrhythmic episodes requiring medical attention. Figure A.2. (Appendix) shows that RFA becomes cost-effective from the second year (ICER less than three times GDP), highly cost-effective from the fourth year (less than GDP), and cost saving from the seventh year. This is even considering a second ablation for those in whom it failed the first time, and those who develop any complication. RFA remained the dominant strategy after performing probabilistic and deterministic sensitivity analysis, even with a decrease in the cost of medications of 50%.
This suggests that RFA, especially in low-income countries, should be the most appropriate therapeutic choice, especially in young patients who would otherwise require lifelong MT[16]. RFA is either cost-saving or has a cost-effectiveness ratio comparable to many commonly accepted therapies for other diseases [7].
Our sensitivity analyses indicate that RFA is likely to be cost-saving or cost-effective under a wide range of assumptions. We made several assumptions to produce a tractable model. We used a long-term perspective to consider in more detail the cost and risk associated to the strategies. Prolonged drug therapy leads to both increased expenditures and an increased risk of side effects. We also explicitly modeled crossovers between therapies.
RFA is considered a safe procedure. No deaths were included in the second ablation because it has not been found in previous analysis [4] or it has been significantly lower (0.016% [7], 0.05% [16] and 0.001% [17]) that the 0.03% assumed for our model.
We acknowledge that resterilization is a suboptimal and unconventional procedure to lower costs, despite the fact that our experience shows no increase in complication rates [4].
The high interest rates in loans in the banking system and eventual currency devaluation make the 12% discount rate that we used a conservative rate. It is important to realize that most US studies have used a discount rate of 3%, because the more stable economic system in the US [8].
This model has several limitations. Since our institution does not possess the information needed to calculate the cost of every single medication used in the electrophysiology study, we included information provided by UNICAR using hypothetical patients who underwent catheter ablation and information about the most commonly prescribed drugs. Since this may not always be the case, costs might be underestimated (even though this would represent less than 5% of the total cost of the procedure). Another limitation relates to the fact that before patients were referred to our unit they were treated by a variety of cardiologists without a standard anti-arrhythmic protocol [4]. Furthermore, we are not including other comorbidities in the 35 years' timeframe that could have decreased the QALYs of a given patient.
The fact that we did not include emergency department treatment in our model because it is not offered in UNICAR does not necessarily mean that the patient did not require such treatment (and expenditure) in case of a recurrence of the arrhythmia. If MT patients were to require emergency department treatment, RFA would have an even larger decrease in expenditures.
5. Conclusions
Our study found that RFA dominates MT by improving quality of life and reducing expenditures when used to treat severely symptomatic patients. This is a constant finding, even after varying assumptions about efficacy, complication rates and quality of life of patients after RFA. Although this analysis used data from Guatemala, the robustness of the results to variations in parameter assumptions suggests that the insights from this study may also hold for other low-income countries with similar costs and procedures.
Given our findings, it may be cost-effective to allocate resources in low-income countries to develop facilities specialized in cardiac electrophysiology in order to treat effectively, definitively, and at lower cost the patients with SVT.
We recommend to continue testing the cost-effectiveness of high technology therapies in developing countries and different settings, as the different experience of the teams, cultural acceptance and lower costs, can provide different results than those in developed countries.
Supplementary Material
Key Points.
Already Known
RFA is an established but expensive treatment alternative for SVT.
In developed countries RFA has been proved to be cost-effective in the treatment of SVT.
No studies about this topic exist on an adult Latin American population.
Adding to existing knowledge
The basic cost of RFA in Guatemala is $ 5411, with a cumulative success rate of 94%.
In our model RFA dominates the MT by improving quality of life and reducing expenditures.
RFA continues to be highly cost-effective after performing sensitivity analyses.
Insights provided for informed health care decision making
RFA becomes highly cost-effective from the 4th year and cost-saving from the 7th year.
Especially in a low-income country, RFA should be the most appropriate therapeutic choice.
In low-income countries, it may be cost-effective to develop facilities specialized in RFA.
Acknowledgments
The authors thank Salvador Cruz, M.Sc., for his help with the cost analysis and model projections, Carl Mendoza-Montano, PhD and Brett Griffiths, PhD for editorial assistance and Maximiliano Guerra, MD for his help in data collection and database entry.
Funding Sources: The study design and data collection was funded by the National Unit of Cardiovascular Surgery, UNICAR. The interpretation of data and analysis reported in this publication was supported by the Fogarty International Center and National Institute of Aging of the National Institutes of Health under Award Number D43 TW009315. The content is solely the responsibility of the authors and does not necessarily represent the official views of UNICAR or the National Institutes of Health.
Abreviations
- EPS
electrophysiology study
- GDP
Gross Domestic Product
- ICER
Incremental cost-effectiveness ratio
- ICU
Intensive care Unit
- MT
Medical Treatment
- QALY
Quality Adjusted Life Years
- RFA
Radiofrequency ablation
- SVT
supraventricular tachycardia
- UNICAR
Unidad Nacional de Cirugía Cardiovascular (National Unit of Cardiovascular Surgery)
- WPW
Wolf-Parkinson-White
Footnotes
Disclosures: All authors have approved the final article. None of the authors report additional fees from UNICAR or any company per each RFA performed.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Link MS. Evaluation and Initial Treatment of Supraventricular Tachycardia. N Engl J Med. 2012 Oct 11;367(15):1438–48. doi: 10.1056/NEJMcp1111259. [DOI] [PubMed] [Google Scholar]
- 2.Orejarena LA, Vidaillet H, Jr, DeStefano F, Nordstrom DL, Vierkant RA, Smith PN, et al. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol. 1998;31:150–7. doi: 10.1016/s0735-1097(97)00422-1. [DOI] [PubMed] [Google Scholar]
- 3.Kay GN, Plumb VJ. The present role of radiofrequency catheter ablation in the management of cardiac arrhythmias. Am J Med. 1996;100:344–56. doi: 10.1016/S0002-9343(97)89495-8. [DOI] [PubMed] [Google Scholar]
- 4.Vida VL, Calvimontes GS, Macs MO, Aparicio P, Barnoya J, Castañeda AR. Radiofrequency catheter ablation of supraventricular tachycardia in children and adolescents: feasibility and cost-effectiveness in a low-income country. Pediatr Cardiol. 2006 Jul-Aug;27(4):434–9. doi: 10.1007/s00246-006-1220-8. Epub 2006 Jul 6. [DOI] [PubMed] [Google Scholar]
- 5.The World Bank. Principal Global Indicators. [accessed Mar 29, 2014];2014 available at http://data.worldbank.org/country/guatemala.
- 6.National Institute of Statistics of Guatemala. INE proyecciones 2008-2020. [accessed Mar 29, 2014];2013 available at http://www.ine.gob.gt/index.php/estadisticas/tema-indicadores.
- 7.Hogenhuis W, Stevens SK, Wang P, Wong JB, Manolis AS, Estes NA, 3rd, et al. Cost-effectiveness of radiofrequency ablation compared with other strategies in Wolff-Parkinson-White syndrome. Circulation. 1993;88:II437–46. [PubMed] [Google Scholar]
- 8.Cheng CH, Sanders GD, Hlatky MA, Heidenreich P, McDonald KM, Lee BK, et al. Cost-Effectiveness of Radiofrequency Ablation for Supraventricular Tachycardia. Ann Intern Med. 2000;133:864–876. doi: 10.7326/0003-4819-133-11-200012050-00010. [DOI] [PubMed] [Google Scholar]
- 9.Kalbfleisch SJ, Calkins H, Langberg JJ, el-Atassi R, Leon A, Borganelli M, et al. Comparison of the cost of radiofrequency catheter modification of the atrioventricular node and medical therapy for drug-refractory atrioventricular node reentrant tachycardia. J Am Coll Cardiol. 1992;19:1583–7. doi: 10.1016/0735-1097(92)90621-s. [DOI] [PubMed] [Google Scholar]
- 10.Anderson JL. Long-term safety and efficacy of flecainide in the treatment of supraventricular tachyarrhythmias: the United States experience. The Flecainide Supraventricular Tachyarrhythmia Investigators. Am J Cardiol. 1992;70:11A–17A. doi: 10.1016/0002-9149(92)91072-c. [DOI] [PubMed] [Google Scholar]
- 11.Clair WK, Wilkinson WE, McCarthy EA, Pritchett EL. Treatment of paroxysmal supraventricular tachycardia with oral diltiazem. Clin Pharmacol Ther. 1992;51:562–5. doi: 10.1038/clpt.1992.63. [DOI] [PubMed] [Google Scholar]
- 12.Meheran Roxana, MD, et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials AConsensus Report From the Bleeding Academic Research Consortium. Circulation. 2011;123:2736–2747. doi: 10.1161/CIRCULATIONAHA.110.009449. [DOI] [PubMed] [Google Scholar]
- 13.Calkins H, Bigger JT, Jr, Ackerman SJ, Duff SB, Wilber D, Kerr RA, Bar-Din M, Beusterien KM, Strauss MJ. Cost-effectiveness of catheter ablation in patients with ventricular tachycardia. Circulation. 2000 Jan 25;101(3):280–8. doi: 10.1161/01.CIR.101.3.280. [DOI] [PubMed] [Google Scholar]
- 14.WHO. Geneva: World Health Organization; 1998. [accessed Mar 29, 2014]. CHOosing Interventions that are Cost Effective (WHO-CHOICE) Available at http://www.who.int/choice/description/en/ [Google Scholar]
- 15.Ikeda T, Sugi K, Enjoji Y, et al. Cost effectiveness of radiofrequency catheter ablation versus medical treatment for paroxysmal supraventricular tachycardia in Japan. J Cardiol. 1994;24:461–468. [PubMed] [Google Scholar]
- 16.Bathina MN, Mickelsen S, Brooks C, et al. Radiofrequency catheter ablation versus medical therapy for initial treatment of supraventricular tachycardia and its impact on quality of life and healthcare costs. Am J Cardiol. 1998;82:589–593. doi: 10.1016/s0002-9149(98)00416-0. [DOI] [PubMed] [Google Scholar]
- 17.Reynolds MR, Zimetbaum P, Josephson ME, Ellis E, Danilov T, Cohen DJ. Cost-effectiveness of radiofrequency catheter ablation compared with antiarrhythmic drug therapy for paroxysmal atrial fibrillation. Circ Arrhythm Electrophysiol. 2009 Aug;2(4):362–9. doi: 10.1161/CIRCEP.108.837294.. Epub 2009 Apr 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Larson MS, McDonald K, Young C, Sung R, Hlatky MA. Quality of life before and after radiofrequency catheter ablation in patients with drug refractory atrioventricular nodal reentrant tachycardia. Am J Cardiol. 1999;84:471–3. doi: 10.1016/s0002-9149(99)00338-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.