

Abstract
Every material that gastrointestinal system cannot digest will make a bezoar. Trichobezoar is the result of hair ingestion whether self-hair or from others and is not a common disorder in humans. It is a hairball, which mostly has been seen in females at teenage, or adolescence. It usually locates in stomach but in rare conditions, it will pass through the intestine, and make the Rapunzel syndrome. Herein we present a 13-year-old girl suffering from gastric trichobezoar presenting with failure to thrive.
Keywords: Rapunzel syndrome, Trichobezoar, Trichophagia
Introduction
Chewing or eating not anything that gastrointestinal tract can digest will make bezoar. Bezoars are balls that contain different foreign materials like vegetables, hair or any other fibers (1, 2). Trichobezoar is a hairball found mostly in the stomach and duodenum (3, 4). It mostly occurs in females under 30 years of age and is usually associated with trichotillomania (5, 6). Ingestion of the pulled hair can result in trichobezoar formation and subsequent anemia, abdominal pain, hematemesis, nausea and/or vomiting, bowel obstruction and perforation, gastrointestinal (GI) bleeding, pancreatitis, and obstructive jaundice. The Most common presentation of trichobezoar is small bowel obstruction (SBO) but a rare and sometimes bizarre presentation is reported worldwide (7, 8).
Gastric trichobezoar is a very rare entity. If it is diagnosed early and treated successfully, causes no significant complication. In some settings, despite different workups, the presence of partial bowel or generally GI obstruction misleads physicians to look for other causes in order to explain the patient’s sign and symptoms. Although trichobezoars mostly involve the stomach, in rare condition trichobezoar can extends to other parts of the intestine like, duodenum, jejunum and colon. This condition is called the Rapunzel syndrome first described in 1968 (1, 9–11).
Here, we present a patient suffering from gastric trichobezoar presenting with failure to thrive.
Case Presentation
On 2014, a 13-year-old girl presented in our pediatric surgery ward at Namazi Hospital, Shiraz, Iran, with the complaints of epigastric fullness and mass sensation. In physical examination, she was pale, dehydrated with sunken eyes, total body weight (TBW) was 21 kg, and she had stable hemodynamics except tachycardia.
She had a scaphoid abdomen with bulged epigastric region and sensation of fullness in palpation of that area without any tenderness or rebound.
There was no lymphadenopathy and her neurologic examination was normal. She had a history of poor weight gain, poor appetite and iron deficiency anemia. She also mentioned postprandial vomiting and occasional abdominal pain and was admitted previously elsewhere without any definite diagnosis. Tests was required include complete blood count with mean corpuscular volume of erythrocyte was 78 and hemoglobin was 12 in laboratory data. In further work ups, Hb electrophoresis was normal, serum ferritin was 7.2 at lower limit of normal (normal range :7–140), thyroid function tests were normal, growth hormone was 2.4 and it was in normal range, liver function tests were normal, urine analysis and stool exam were normal, too.
Because of her epigastric mass, she was referred to a pediatric gastroenterologist. Upper endoscopy showed a hairy mass in the stomach (gastric trichobezoar). This mass was not extractable by an endoscope, so an open operation was planned for the patient. In the operating room after general anesthesia, gastrostomy was performed via vertical midline laparotomy incision.
The trichobezoar, which weighed about 800 gr and fulfilled the whole stomach and duodenum, was evacuated and it was shaped like gastroduodenal curvature (Fig. 1, 2). The postoperative period was complaint free.
Fig. 1:
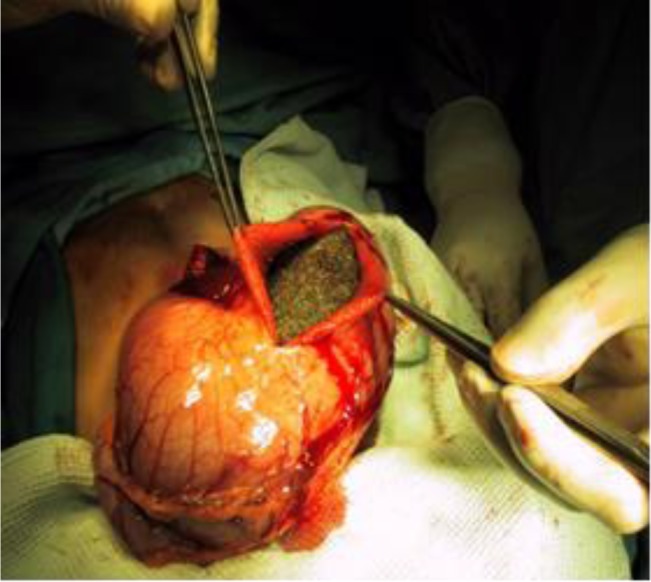
Enterotomy and removing the trichobezoar
Fig. 2:

Stomach-shaped trichobezoar
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Discussion
Although trichobezoar is a rare condition, but it is one of the important differential diagnoses that every physician especially gastroenterologists and surgeons should keep in mind in patients with obstructive GI problems which is the most common presentations of this disease. As aforementioned, it is more common in young females with concordant psychological problems such as trichotillomania or subtypes of pica disorder.
Trichotillomania results in highly variable patterns of hair loss, ranging from small undetectable patches of hair loss to total baldness and because of ingested hair accumulation, it may present with different kinds of GI problems (9, 12–14). Not all cases of trichotillomania have trichophagia, also all of patients with trichophagia will not have trichobezoars (15).
The complications of trichobezoar are including bowel obstruction, nausea and vomiting, sensation of mass and fullness, loss of appetite and in severe cases perforation and bleeding have been reported (9, 16). According to the complications of the trichobezoar, we should keep this diagnose in mind to avoid severity in this condition such as, bleeding or obstruction and perforation, especially in patients with mental retardation or any psychological problem (16).
In this patient, the uncommon presentation was failure to thrive, which happened because of late diagnosis. As the trichobezoar grows, recurrent bouts of nausea, vomiting, epigastric pain, and occasionally hematemesis can occur because of intermittent gastric outlet obstruction. However, in this patient the symptoms did not lead the physicians to the exact diagnose and they missed it because of the poor history taking or the wide differential diagnosis of gastric obstruction.
Another rare complication of gastric trichobezoar is gastric perforation due to intragastric high pressure known as Rapunzel’s syndrome (9, 16–19). The diagnosis can often be made based on history, physical findings, conventional radiography and barium study of the gastrointestinal tract.
Treatment for symptomatic gastrobezoar is usually surgical intervention but some advocate primary non-surgical attempts such as transendoscopic fragmentation and extraction or transendoscopic lytic enzyme administration although the success of these methods depends on the size of trichobezoar and its duration of formation. Older trichobezoar is much harder to treat with transendoscopic lytic enzyme administration.
Generally, even surgical treatment of gastric trichobezoar is not very challenging when diagnosis is made. The most important step in this disease is primary diagnosis and post treatment prophylaxis against further bezoar formation by the patient. The latter mentioned issue needs complete teamwork of psychiatrist, gastroenterologist and surgeon. Moreover, good referral system after each step should be taken into account. Understanding about trichobezoars will help physicians to deal with these patients in correct way and diagnose this condition at early stage (9, 16, 20, 21).
Ethical considerations
Ethical issues (including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Acknowledgements
The authors declare that there is no conflict of interests.
References
- 1. Gonuguntla V, Joshi DD. ( 2009). Rapunzel syndrome: a comprehensive review of an unusual case of trichobezoar. Clin Med Res, 7: 99– 102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Palanivelu C, Rangarajan M, Senthilkumar R, Madankumar MV. ( 2007). Trichobezoars in the stomach and ileum and their laparoscopy-assisted removal: a bizarre case. Singapore Med J, 48: e37– 9. [PubMed] [Google Scholar]
- 3. Larbi N, Kaabi S, Ben Salah K. ( 2003). [Gastric and intestinal bezoars]. Tunis Med, 81: 949– 55. [PubMed] [Google Scholar]
- 4. Bouwer C, Stein DJ. ( 1998). Trichobezoars in trichotillomania: case report and literature overview. Psychosom Med, 60: 658– 60. [DOI] [PubMed] [Google Scholar]
- 5. Christenson GA, Pyle RL, Mitchell JE. ( 1991). Estimated lifetime prevalence of trichotillomania in college students. J Clin Psychiatr, 52: 415– 7. [PubMed] [Google Scholar]
- 6. Sehgal VN, Srivastava G. ( 2006). Trichotillomania +/− trichobezoar: revisited. J Eur Acad Dermatol Venereol, 20: 911– 5. [DOI] [PubMed] [Google Scholar]
- 7. Ousadden A, Mazaz K, Mellouki I, Taleb KA. ( 2004). [Gastric trichobezoar: one case report]. Ann Chir, 129: 237– 40. [DOI] [PubMed] [Google Scholar]
- 8. Cohen LJ, Stein DJ, Simeon D, Spadaccini E, Rosen J, Aronowitz B, Hollander E. ( 1995). Clinical profile, comorbidity, and treatment history in 123 hair pullers: a survey study. J Clin Psychiatr, 56: 319– 26. [PubMed] [Google Scholar]
- 9. Gorter RR, Kneepkens CM, Mattens EC, Aronson DC, Heij HA. ( 2010). Management of trichobezoar: case report and literature review. Pediatr Surg Int, 26: 457– 63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Naik S, Gupta V, Naik S, Rangole A, Chaudhary AK, Jain P, Sharma AK. ( 2007). Rapunzel syndrome reviewed and redefined. Dig Surg, 24: 157– 61. [DOI] [PubMed] [Google Scholar]
- 11. Vaughan ED, Jr., Sawyers JL, Scott HW., Jr. ( 1968). The Rapunzel syndrome. An unusual complication of intestinal bezoar. Surgery, 63: 339– 43. [PubMed] [Google Scholar]
- 12. Nuss MA, Carlisle D, Hall M, Yerneni SC, Kovach R. ( 2003). Trichotillomania: a review and case report. Cutis, 72: 191– 6. [PubMed] [Google Scholar]
- 13. Reeve EA, Bernstein GA, Christenson GA. ( 1992). Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatr, 31: 132– 8. [DOI] [PubMed] [Google Scholar]
- 14. Kleiner O, Finaly R, Cohen Z. ( 2002). Giant gastric trichobezoar presenting as abdominal mass in a child. Acta Paediatr, 91: 1273– 4. [PubMed] [Google Scholar]
- 15. Salaam K, Carr J, Grewal H, Sholevar E, Baron D. ( 2005). Untreated trichotillomania and trichophagia: surgical emergency in a teenage girl. Psychosomatics, 46: 362– 6. [DOI] [PubMed] [Google Scholar]
- 16. Avissar E, Goldberg M, Lernau O. ( 1994). Bezoar-induced ulceration and perforation of the upper gastrointestinal tract in mentally retarded patients. Pediatr Surg Int, 9: 279– 280. [Google Scholar]
- 17. Zamir N, Akhtar J, Ahmed S. ( 2011). Delayed presentation of trichobezoar with small bowel obstruction. APSP J Case Rep, 2: 6. [PMC free article] [PubMed] [Google Scholar]
- 18. Zamir D, Goldblum C, Linova L, Polychuck I, Reitblat T, Yoffe B. ( 2004). Phytobezoars and trichobezoars: a 10-year experience. J Clin Gastroenterol, 38: 873– 6. [DOI] [PubMed] [Google Scholar]
- 19. Wadlington WB, Rose M, Holcomb GW., Jr. ( 1992). Complications of trichobezoars: a 30-year experience. South Med J, 85: 1020– 2. [DOI] [PubMed] [Google Scholar]
- 20. Reisfeld R, Dammert W, Simpson JS. ( 1978). Trichobezoar: an uncommon pediatric problem. Can J Surg, 21: 251– 2. [PubMed] [Google Scholar]
- 21. Gayer G, Jonas T, Apter S, Zissin R, Katz M, Katz R, Amitai M, Hertz M. ( 1999). Bezoars in the stomach and small bowel--CT appearance. Clin Radiol, 54: 228– 32. [DOI] [PubMed] [Google Scholar]