
Fig. 1.
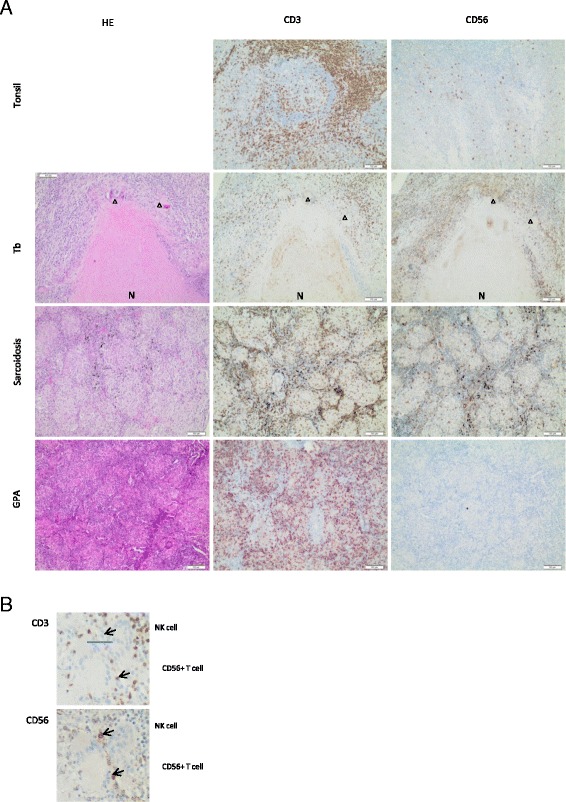
CD56+ cells are not detectable in granulomatosis with polyangiitis (GPA) but are present in granulomas of classical granulomatous diseases. Patient material was derived from and processed in the Heidelberg tissue bank for inflammatory diseases. Sequential paraffin-embedded sections were stained with hematoxylin and eosin (HE) (left column), anti-CD3 antibody (middle column), and anti-CD56 antibody (right column). a Normal tonsil tissue served as a positive control for CD3 and CD56 staining (top row). Representative tissue sections of granulomas from tuberculosis (Tb) (n = 5; second row), sarcoidosis (n = 5; third row), and GPA (n = 13; bottom row) patients. Healthy lung tissue at the border of GPA granulomas contained scattered CD56+ cells (not shown). Arrowheads point to giant cells. N necrosis. Measurement bars indicate 100µm. b Enlarged cutout from the sequential Tb sections shown in (a). Upper arrows, CD3−CD56+ natural killer (NK) cells; lower arrows, CD3+CD56+ T cells