

Abstract
Saphenous reflux interferes with the physiological decrease in pressure and induces ambulatory venous hypertension. Elimination of reflux is achieved by flush ligation at the incompetent saphenofemoral junction and stripping of the great saphenous vein, which is the basis of the conventional surgical therapy. Endovenous ablative methods substitute stripping by thermal of chemical destruction of the saphenous trunk; they usually refrain from saphenofemoral junction ligation. Short-term and medium-term results up to 5 years, achieved after endovenous ablation without high ligation, are comparable with those after conventional surgery, which questioned the necessity to ligate the incompetent saphenofemoral junction. Nevertheless, clinical symptoms caused by recurrent reflux occur as a rule not earlier than 8 to 10 years after efficient abolition of reflux. Consequently, randomized studies with long-term follow-ups exceeding 10 years are necessary for trustworthy assessment whether it is justified to abstain from saphenofemoral junction ligation.
Keywords: endovascular procedure, endovenous ablation, greater saphenous vein, lower extremity, radiofrequency ablation, varicose veins, vein reflux
Saphenous reflux is the most important hemodynamic phenomenon in varicose vein disease inducing ambulatory venous hypertension. Complete suppression of reflux in the great saphenous vein (GSV) can be achieved either by closing the incompetent saphenofemoral junction (SFJ) or by interrupting the incompetent saphenous trunk. Both measures are effective, as documented by the Trendelenburg test, venous pressure measurements, and plethysmography. The conventional surgical therapy includes crossectomy and stripping, that is, elimination of both preconditions enabling saphenous reflux. The following crucial questions arise: to achieve efficient and long-standing abolition of saphenous reflux and to prevent or at least delay the reappearance of reflux, is it necessary to eliminate both the factors, the source of reflux and the reflux-carrying channel? Or is it sufficient to exclude only one of these causal elements? The objectives of this review are to assess the following:
Is SFJ ligation (crossectomy) without stripping adequately effective?
Are ablative methods: stripping, endovenous laser ablation (EVLA), radiofrequency ablation (RFA), and ultrasound-guided foam sclerotherapy (UGFS) without ligation of incompetent SFJ effective enough?
Reports were gathered from the literature to deal with these issues.
Impact of the Refluxing SFJ and Incompetent GSV on the Hemodynamic Disturbance
Calf pump activity is the motive force inducing hemodynamic changes in the lower extremity. The hydrostatic pressure at the ankle amounts in the quiet standing position to approximately 80 to 100 mm Hg depending on body height; it decreases during calf pump activity to approximately 25 mm Hg. This phenomenon has been called physiological decrease in venous pressure; it comes up only in the lower leg and foot. In contrast to that, the pressure in the thigh veins (popliteal and femoral) does not decrease during calf pump activity; it shows systolic and diastolic pressure deviations but at the end of calf muscle contractions it keeps to the value of the hydrostatic pressure. This fact was documented by direct pressure measurements performed in the popliteal and posterior tibial vein by Höjensgard and Stürup1 as well as by Arnoldi.2 As a consequence, ambulatory pressure gradient of 37.4 ± 6.4 mm Hg arises between veins in the thigh and the lower leg during calf pump activity.3 This ambulatory pressure gradient is the motive force setting off saphenous reflux in varicose vein disease. When the saphenous reflux is interrupted , for example, by crossectomy, the venous blood is drained from the remaining incompetent superficial thigh veins into deep lower leg veins, and the lower pressure extends from deep lower leg veins into the superficial thigh veins; the boundary of the ambulatory pressure gradient, which in healthy persons separates thigh veins from lower leg veins, is relocated in varicose vein patients into the thigh, and separates now popliteal, femoral, and iliac veins from superficial thigh veins.4 This is the hemodynamic impulse triggering the chain of events leading to varicose vein recurrence.5 The process is induced by the fluid shear stress on the endothelium and accomplished by the vasoactive agent nitride oxide and vascular endothelial growth factor, which entails progressive dilatation of preexisting tiny communications between the femoral vein and the saphenous system in the thigh6 7 8 9; it has been called neovascularization, or more precisely, vascular remodeling.10 As a consequence, new incompetent connections develop between the femoral vein and incompetent superficial veins in the thigh and cause recurrent reflux. In this way, the tenacious tendency of varicose veins to recur after any therapeutic procedure can be explained. The pressure difference arising between deep and superficial veins in the thigh during calf pump activity is the characteristic feature of varicose vein disease. Because this hemodynamic stimulus is not present in people with healthy veins, neovascularization in the groin does not occur after harvesting of the GSV for bypass purposes.
Saphenous reflux streaming through incompetent SFJ is the most common cause of venous hemodynamic disorders and congestive symptoms; it interferes with the physiological decrease in pressure and causes ambulatory venous hypertension in the lower leg and foot. Ambulatory venous hypertension is the result of the interplay between the ejecting capability of the calf pump and the reflux intensity, which can be documented by plethysmography. When the expelled and refluxing volumes equal, no decrease in pressure occurs and the gravest form of ambulatory venous hypertension takes place.
Trendelenburg11 recognized at the turn of the 19th century that retrograde streaming in the GSV induced venous congestion in the lower leg in varicose vein patients and was responsible for the pathological condition inclusive of varicose ulcers. He documented this fact with his well-known test. In the pre-Trendelenburg era, the trunk of the GSV was regarded as an important drainage channel; according to the meaning at that time, ligation of the GSV trunk would have worsened the congestion in the varicose veins. The original Trendelenburg operation consisted of interruption of the GSV in the lower part of the thigh. The disease at that time was called varices cruris (varicose veins of the lower leg); thus, ligation above the knee was regarded as adequate to interrupt the saphenous reflux feeding varicose veins in the leg. Later on, Trendelenburg operation became converted to high ligation at the SFJ. The results of the Trendelenburg operation, as reported by Perthes,12 were very good. Many patients operated by Trendelenburg had leg ulcers that healed rapidly after the operation.
Because the term “venous reflux in the lower extremity” has not yet been precisely defined and is not properly understood, the definition of reflux is given here.
Venous reflux in the lower extremity is a centrifugal, pathological flow of blood within an incompetent venous channel connecting both poles of the pressure difference. The higher pole of the pressure difference lies in the popliteal, femoral or iliac vein, the lower pole in deep lower leg veins. Reflux is released by calf pump activity, takes place during relaxation of the calf musculature, exceeds the duration of the physiological centrifugal streaming lasting 200 to 300 milliseconds, and stops as soon as the pressure difference has been equalized. It can also be evoked by increased intra-abdominal pressure propagating into the iliac, femoral, and the popliteal vein. Reflux interferes with a physiological decrease in pressure arising during calf pump activity in deep and superficial veins of the lower leg and foot; it causes ambulatory venous hypertension, the degree of which depends on the intensity of the centrifugal flow expressed in mL/s.
The outward flow within calf perforators has been erroneously denoted reflux; regrettably, this opinion is still generally accepted. The systolic outward flow in calf perforators continues in the GSV as a centripetal flow toward the heart and does not cause any hemodynamic disturbance; it does not interfere with the physiological decrease in pressure nor causes ambulatory venous hypertension. Thus, it is harmless, in the physiological direction toward the heart oriented flow, evoked by the contraction of the “peripheral heart.” The hemodynamic disorder in the lower leg is caused by the centrifugal, refluxing, diastolic, within the calf perforators inward into deep lower leg veins directed flow; it is set off by the ambulatory pressure gradient. Thus, reflux within calf perforators is inward, not outward-oriented flow. The false assertion that the outward flow in calf perforators is a deleterious reflux should be definitely discarded. To point out once more the difference: venous reflux is a diastolic, centrifugal, pathological phenomenon; the outward flow within calf perforators is a systolic, centripetal, in the physiological direction toward the heart-oriented flow.
The effect of GSV reflux on the venous hemodynamics can be eliminated either by interruption of the source (the incompetent SFJ) or by suppression of the incompetent GSV trunk. Interruption of the feeding source of reflux removes the hemodynamic disturbance, as documented by plethysmography13 14 and demonstrated in Figs. 1 and 2. The same favorable hemodynamic effect is achieved by interruption of the reflux-carrying channel; Trendelenburg demonstrated this fact with his test. The effect of the Trendelenburg test was corroborated by venous pressure measurements (Figs. 3 and 4). Unfortunately, this excellent immediate hemodynamic effect deteriorates progressively during the follow-up because of the increasing intensity of recurrent reflux,15 as shown in Fig. 5.
Fig. 1.
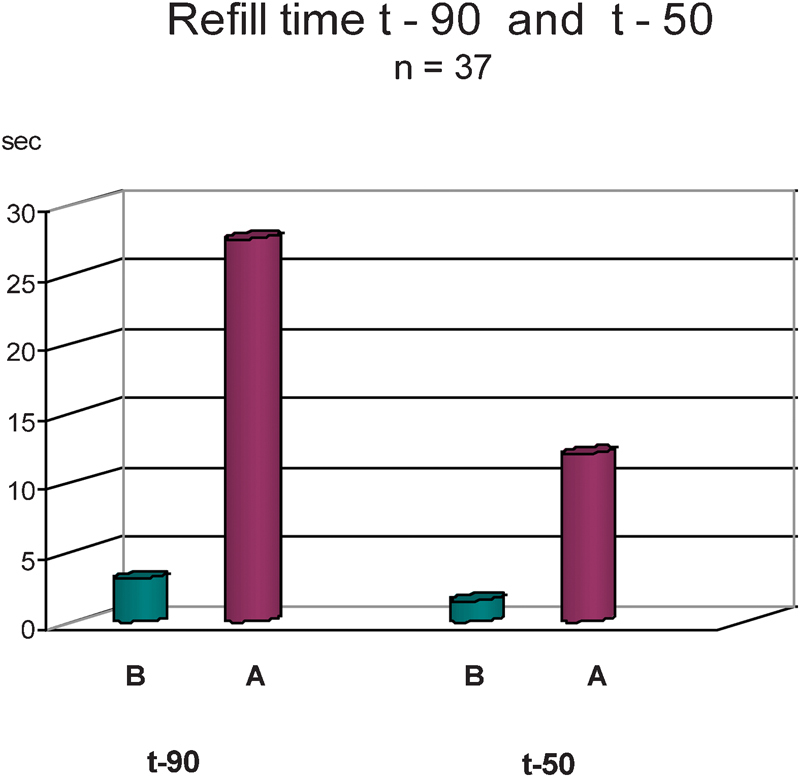
Impact of saphenous reflux on the hemodynamic disturbance documented by strain gauge plethysmographic parameters refill time t = 90 and t = 50. Green columns: before crossectomy, purple columns: 1 week after crossectomy. Abolition of saphenous reflux eliminated the gravest pretreatment hemodynamic disorder and reestablished physiological hemodynamic values.
Fig. 2.
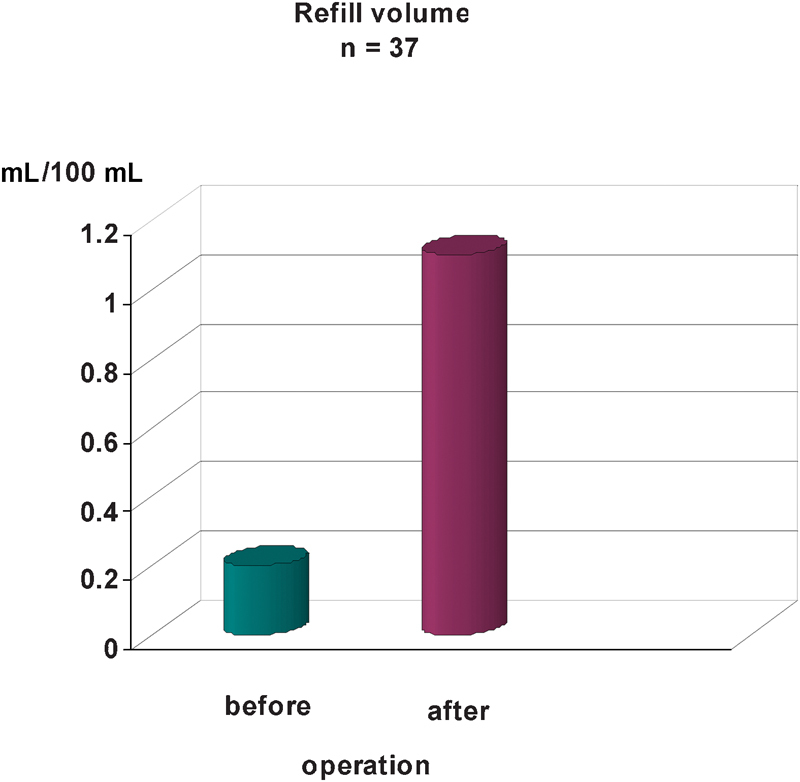
Impact of saphenous reflux on the hemodynamic disturbance evaluated by strain gauge plethysmographic parameter refill volume. Green column: before crossectomy, purple column: one week after crossectomy. Abolition of saphenous reflux eliminated the gravest pretreatment hemodynamic disorder and reestablished physiological hemodynamic values.
Fig. 3.
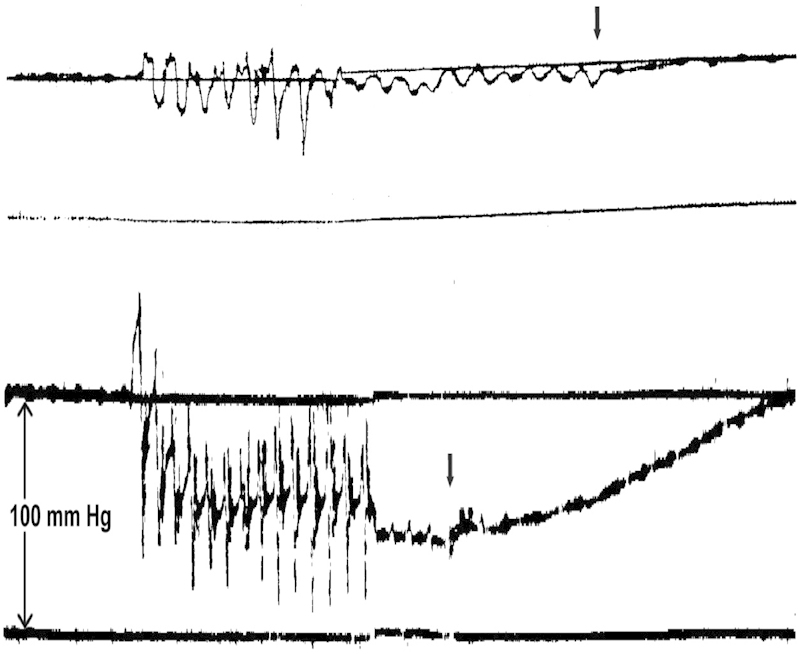
Top: Venous pressure recordings in the great saphenous vein above the ankle. There was as good as no decrease in venous pressure during calf pump activity documenting the gravest form of ambulatory venous hypertension in a patient with varicose ulcer and severe reflux in the great saphenous vein (factual pressure followed by damped pressure). Arrow marks the end of muscle contractions. Bottom: The same patient as above. Pronounced decrease in pressure during calf pump activity after interruption of saphenous reflux in the thigh; prolonged return to the starting level followed during the recovery period documenting restoration of physiological pressure conditions.
Fig. 4.
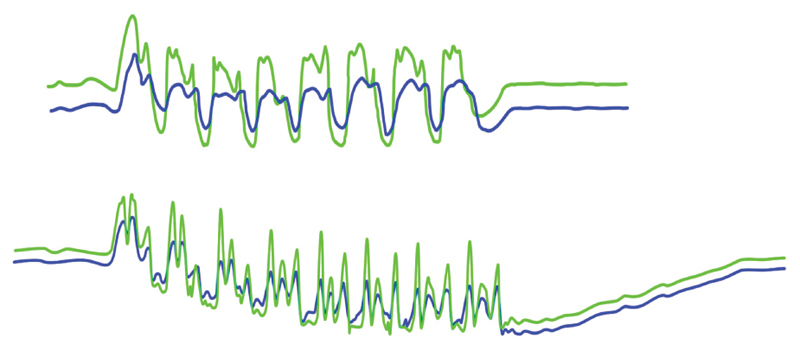
Simultaneous pressure recordings in the posterior tibial vein (green) and great saphenous vein (blue) in a patient before (above) and after (below) interruption of saphenous reflux in the thigh. No decrease in pressure in the great saphenous vein as well as in the posterior tibial vein under the influence of the strong saphenous reflux. After interruption of the saphenous reflux, the venous pressures in both veins returned to the physiological status.
Fig. 5.
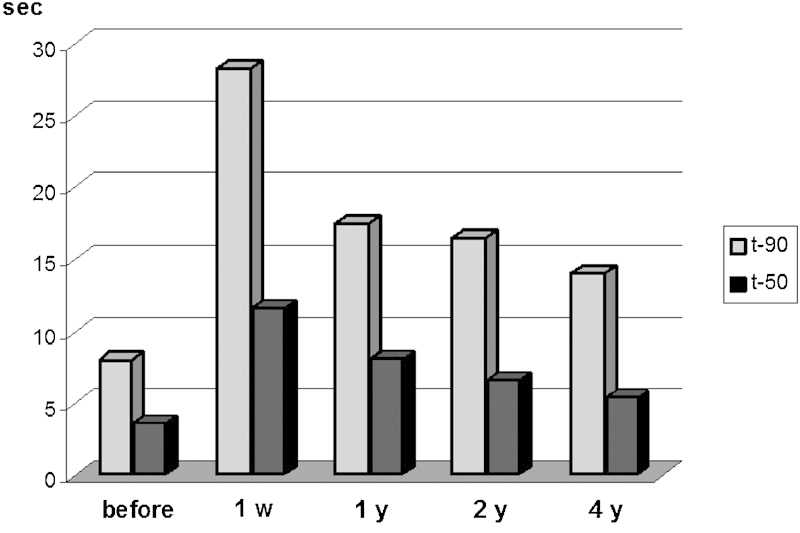
Progressive deterioration of the hemodynamic condition during follow-up illustrated by strain gauge plethysmographic parameters refill time t = 90 and t = 50; w = week, y = year(s). In comparison with the pretreatment status, the hemodynamic situation remained significantly improved 4 years after abolition of saphenous reflux in the groin in spite of the successive deterioration.
Hemodynamically significant reflux streaming through SFJ and GSV is fed from incompetent iliac veins; this condition is typical of varicose vein disease.11 16 Sufficient amount of blood is available for forceful GSV reflux in incompetent iliac veins and inferior vena cava to counteract the ambulatory pressure gradient and to equalize the decreased pressure in the lower leg veins. Any competent valve situated above the SFJ (in common femoral, iliac vein) reduces the blood volume necessary to counterbalance the decreased pressure in the lower leg veins. Blood volume contained between the competent valve in the common femoral/iliac vein and the SFJ is too small to equalize the pressure gradient, and is therefore, hemodynamically not fully effective or even of little importance.
Impact of the Refluxing SFJ and Incompetent GSV on the Development of Recurrent Reflux and Varicose Vein Recurrences
An international consensus meeting held on recurrent varices after surgery (REVAS) in Paris in 1998 agreed to adopt the following clinical definition17: “REVAS means the existence of varicose veins in the lower limb previously operated on for varicosities, with or without adjuvant therapies, which includes true recurrences, residual veins, and new varices as a result of disease progression.”
Recurrences after varicose vein surgery are common events with a wide range depending on the length of follow-up, the applied therapeutic procedure, the method to diagnose recurrence, and the comprehension of the venous reflux itself; the incidence reaches values up to 80%.10 18 19 20 21 22 23 24 The cause of recurrences has been ascribed mainly to the following situations:
Inadequate surgery leaving behind overlooked sources of reflux (incompetent saphenopopliteal junction, thigh perforators) or imperfectly removed sources of reflux (remnants of the GSV in the groin).23 25 26 27 28 29 30 31 32
Leaving behind incompetent reflux-carrying channels in the thigh.15 20 32 33 34 35 36
Neovascularization in cases with correctly performed surgery.21 22 37 38 39 40 41
Progression of the disease resulting in development of varices in previously normal veins.
Imperfectly Performed Crossectomy
Leaving behind incompetent SFJ and residual GSV stump with tributaries has been regarded in the past as the main cause of varicose vein recurrences; the incidence has been reported to range mostly between 51 and 83%23 25 26 27 28 29 30 31 32; refluxing residual GSV stumps with tributaries and incompetent SFJ were detected in 68.9,26 51.0,27 65.2,28 83.2,29 65.0,30 and 66.0%.32 New reflux-carrying channels in the groin were documented on venography and duplex ultrasonography (DUS). The number of evaluated limbs ranged from several dozens to several hundreds. These findings emphasize the importance of flush ligation of the SFJ and resection of the terminal GSV segment with its tributaries. Failure to accomplish these principles leaves behind a residual incompetent network of communications between the deep and superficial venous system and constitutes the origin of future recurrences.
Geier et al23 published a multicenter study involving seven centers and conducted among patients undergoing redosurgery for inguinal varicose vein recurrences. The initial operation was performed 13.6 years earlier. In patients with symptomatic groin recurrences, a long residual saphenofemoral stump was found in about two-thirds of cases; leaving a residual GSV stump in the groin was regarded as the most frequent cause for recurrent reflux. The first signs of varicose vein recurrence occurred mostly 7 to 8 years after the initial treatment. Most patients experienced a symptom-free interval after initial operation with a mean duration of 7.4 ± 5.5 years. In other studies, the mean time between the first procedure and reoperation was 17 years25 and 89.7 ± 31.2 months.31 These are important findings documenting that it takes at least 7 or more years for the symptomatic groin recurrence to develop after the initial operation; this must be taken into account when evaluating results after ablative methods performed without SFJ ligation. Egan et al29 presented duplex and operative findings in a consecutive series of 500 limbs undergoing surgery for recurrent varicose veins. Primary GSV surgery was incomplete in 83.2% of limbs; a completely intact GSV system was present in 17.4%. An incompetent thigh segment of saphenous vein was present in 44.2% of limbs; 16% had both a residual thigh segment of GSV and an incompetent stump with intact tributaries in the groin. Neovascularization was identified on duplex scanning in 8.2% of limbs. In only 1.4% of limbs were cross-groin or vulval veins thought to be the major source of recurrent reflux. Stonebridge et al32 found technically unsatisfactory surgery at the SFJ in 66%, and an intact GSV system in 13.2%; in only 1.4% cross-groin or vulval veins were thought to be responsible for recurrent reflux. Neovascularization was found in 3.1%.
Thus, these studies clearly documented that leaving behind incompetent SFJ and residual GSV stump with tributaries in the groin was associated with recurrent reflux and varicose vein recurrences.
Preservation of Incompetent Reflux-Carrying Veins in the Thigh
Several papers and a few randomized studies have shown crossectomy and stripping to be superior to crossectomy alone in terms of limiting varicose vein recurrence.20 28 29 33 34 35 36 42 43 44 In the randomized trial presented by Winterborn et al,20 stripping the GSV reduced the risk of reoperation after 11 years by 60%, although it did not reduce the rate of visible recurrent veins. Although not corroborated by plethysmographic measurements, it indicates that patients with SFJ ligation alone had obviously severer reflux intensity causing congestive symptoms than those with SFJ ligation and stripping. Sarin et al34 randomized 89 limbs to undergo either SFJ ligation and stripping or SFJ ligation alone. At a median of 21 months after surgery, photoplethysmographic refilling times were longer in the cohort where the GSV was stripped than after SFJ ligation alone (p < 0.01), documenting milder reflux intensity after SFJ ligation and stripping in comparison with SFJ ligation alone. More patients were recurrence free (65 vs. 17%) when the GSV was stripped. Dwerryhouse et al36 presented a randomized study of 110 limbs with 5-year follow-up. Stripping reduced the risk of reoperation by two-thirds. Neovascularization at the SFJ was the cause for recurrent saphenofemoral incompetence in 12 of 52 stripped veins versus 30 of 58 ligated SFJs, documenting that preservation of incompetent GSV in the thigh facilitates or accelerates the development of recurrent reflux. Rutgers and Kitslaar43 drew the same conclusion from their randomized study; clinical and Doppler ultrasound evidence of reverse flow in the GSV was significantly less after the stripping operation (p < 0.001). Cosmetic results were significantly better in the stripped limbs. In prospective (nonrandomized) studies, residual incompetent GSV in the thigh was present in 81.5,15 68.9,26 and 60%.32
Recurrences after Correctly Performed Crossectomy
Several studies have challenged the traditional view that recurrences can be prevented by adequately performed surgery. Newly created vessels occurred in the groin in spite of flush ligation at the SFJ and stripping, which was documented by duplex scanning and phlebography.18 22 37 39 40 The reported recurrences ranged between 10 and 60% during the follow-up of 2 to 34 years. Fischer et al18 assessed 125 limbs of 77 patients with recurrent varicose veins operated on 31 to 39 years ago with the mean follow-up interval of 34 years. The study discovered a 60% incidence of recurrent reflux in the groin, which developed through junctional or circumjunctional reconnections after correct ligation of the GSV and its related tributaries and stripping at the original operation. Sonographic findings detected newly created single lumen channels with a diameter of approximately 3 mm originating from the common femoral vein near the previous SFJ and connected to superficial thigh veins; they were hemodynamically important. The other common type of newly developed channels appeared as strands or tangle of veins originating from the former site of ligation. Only 27 reflux recurrences in the groin (21.6%) were symptomatic enough to warrant consideration of additional treatment; 25 of these 27 recurrences were caused by single lumen channels. In contrast to that, the strand-formed recurrences were of little hemodynamic significance.
The ultrasound findings presented by Fischer et al can be demonstrated on the retrograde phlebography performed in a patient with varicose vein recurrence after crossectomy (Fig. 6). Depicted is a single meandering newly developed communication originating from the incompetent common femoral vein and joining the GSV remnant in the thigh; it was responsible for the recurrent reflux. This tortuous channel is situated outside the original field of surgery and arose obviously because of vascular remodeling, that is, through dilatation of preformed tiny, previously nonfunctioning connecting vessels. In addition, a few filiform vessels originating at the former SFJ and oriented directly toward the GSV remnant are also depicted; they arose apparently because of neoangiogenesis and are undoubtedly without any hemodynamic significance. Tortuosity might be the distinctive feature of new veins developed because of vascular remodeling.
Fig. 6.
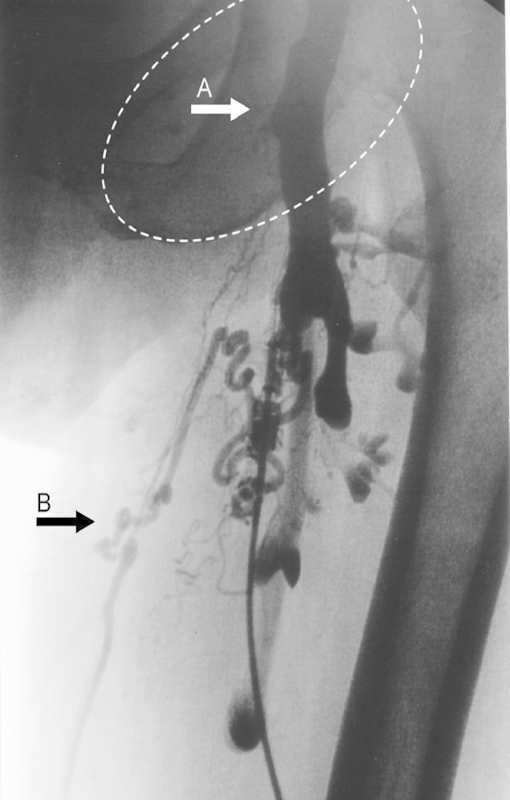
Retrograde phlebography: status post crossectomy. A new large meandering venous communication developed between the incompetent common femoral vein and the great saphenous vein remnant outside of the original field of surgery (marked by the oval line) and caused recurrent reflux. Arrow A indicates the site of the former saphenofemoral junction. The diameter of the great saphenous vein diminished after crossectomy and a valve became competent. Nevertheless, a newly created venous channel bypassed the competent valve and made the entire saphenous remnant incompetent (arrow B). This tortuous bypassing vein, which lies quite distant from the original field of surgery, as well as the large meandering vein arose obviously because of vascular remodeling, not because of neoangiogenesis. The development of both new venous channels was triggered by pressure difference arising during calf pump activity. In addition, strands of tiny nonmeandering vessels spreading between the original saphenofemoral junction and the saphenous remnant are depicted; these vessels are hemodynamically unimportant and arose apparently because of neoangiogenesis.
Randomized Study Comparing Stripping With and Without Crossectomy
Casoni et al45 presented a prospective study encompassing 120 patients (123 limbs) who underwent stripping and were randomly allocated to two groups with or without additional SFJ ligation. The patients were followed up at least 8 years after surgery. The DUS detected recurrence rate amounted to 32.2% in the group with SFJ ligation versus 11.4% in the group without SFJ ligation. The authors did not explain this spectacular result. They admitted that the sonographer who performed the follow-up examination was not blinded to the treatment assignment. In addition, 30 limbs with detected recurrences were treated with ultrasound-guided foam sclerotherapy during the follow-up; it was not specified how many patients with or without SFJ ligation underwent the foam sclerotherapy. This matter of fact casts doubt on the presented results.
Neovascularization
Neovascularization has been regarded as the most common cause of recurrent reflux and varicose vein recurrence in some articles.18 37 38 41 46 In contrast to that, other authors10 29 32 claimed that neovascularization occurred in a relatively small proportion of patients with recurrent varicose veins (in 3.1–8.3%), and that recurrences were mainly associated with inadequate primary surgery or progression of disease. Actually, these assertions are not contradictory. Neovascularization occurs after correctly performed surgery. On the other hand, incompetent SFJ with residual GSV stump and tributaries in the groin forms favorable preconditions for the development of recurrent reflux. When crossectomy is performed correctly, these preconditions do not exist, and new reflux carrying communications must be first created; this happens through neovascularization/vascular remodeling.
Incompetent remnants in the groin as well as incompetent veins in the thigh should not be understood as the cause of recurrences but as preconditions facilitating reappearance of reflux. The real cause is the hemodynamic predisposition to recurrent reflux, which is a component included in the substance of varicose vein disease.5 Residual incompetent saphenous stump with tributaries in the groin is the favorable point of origin; preserved remnants of incompetent saphenous system in the thigh are connector channels; the rest has to be accomplished by vascular remodeling. If residual branches or connector paths were removed, recurrent reflux carrying channels must be created in their entirety, which requires more time.
To be hemodynamically efficient, the recurrent reflux carrying channels must originate from incompetent deep veins; in most cases, they originate from the incompetent common femoral vein. The incompetence of the deep venous system proximal to the SFJ (common femoral vein and iliac veins) is typical of varicose vein disease.11 16
Refluxing veins in the groin are diagnosed predominantly by DUS; unfortunately, this diagnostic tool is not able to reliably discriminate neovascularization from remaining tributaries.10 29 40 47 Persistent venous tributaries to the GSV are being erroneously classified as neovascularization on ultrasonography.29 According to Blomgren et al47 incompetent veins in the groin were found on DUS in 57% of cases 6 to 10 years after SFJ ligation and stripping. It was difficult to distinguish neovascularization from GSV tributaries; it could not be established either with duplex examination or varicography or even at operation whether the tortuous veins in the groin were new vessels or tributaries that had enlarged because of flow changes postoperatively. Principally, this distinction is not necessary. Both phenomena, be it neovascularization or enlarged tributaries are triggered by the same mechanism, that is, by the pressure difference arising during calf pump activity between deep and superficial veins in the thigh in varicose vein patients, and both undergo the same change: vascular remodeling through progressive dilatation.
There are two types of vessels coming up in the groin in connection with neovascularization:
Created because of vascular remodeling, that is, resulting from dilatation of preexisting tiny communications between the femoral vein and incompetent superficial thigh veins; they are apparent as single tortuous channels, originate mostly from the incompetent common femoral vein, and are hemodynamically relevant.10 18
Arisen as a result of neoangiogenesis; these vessels originate from the previous SFJ and connect with the remnant of the GSV or its branches; they have the form of strands or tangle consisting of multiple minute vessels.18 The hemodynamic significance of these strand-like channels is contestable.
In the course of vascular remodeling, the preexisting tiny and hitherto functionless communicating channels that connect the common femoral vein with the saphenous system dilate progressively.10 As mentioned earlier, this process is provoked by the pressure difference of 37.4 ± 6.4 mm Hg arising in varicose veins patients between deep and superficial veins in the thigh during calf pump activity,3 5 and promoted by fluid shear stress and vasoactive agents.6 7 8 9 The tenacious propensity for recurrent reflux and varicose vein recurrence is apparently brought about by this phenomenon.5 No therapeutic method is able to convert all incompetent superficial thigh veins into competent ones and to preclude drainage of venous blood into deep lower leg veins. What CHIVA proponents call “cure hémodynamique” is in reality a deleterious phenomenon causing ambulatory venous hypertension. In view of these hemodynamic circumstances, no therapeutic procedure is capable to definitely heal varicose vein disease; it is just the matter of which therapeutic procedure creates better or worse preconditions for reflux recurrence. We must reconcile ourselves to the fact that recurrences are predestined to occur after any mode of therapy.
The surgical procedure itself has been supposed to trigger the process of neovascularization, as referred to in several papers. The truth of the matter is that the surgical procedure does not promote neovascularization and the development of recurrent reflux in the groin. Dissection techniques in the groin, such as sharp dissection with a knife, dissection with electrocoagulation, and dissection with ultrasound (Ultracision Harmonic Scalpel) did not influence the clinical and sonographic results at 3 months and at 7 years after surgery for recurrent varicose veins.48 Neovascularization does not occur after harvesting GSV for bypass purposes in nonvaricose vein patients because of lack of the hemodynamic prerequisites typical of varicose vein disease. The assertion that surgery in the groin promotes neovascularization is baseless.
Basically, following hemodynamic principles should be observed during the therapeutic procedure to make the preconditions for development of recurrent reflux more difficult:
To interrupt all sources of reflux.
To remove as much of incompetent reflux-carrying veins in the thigh as possible.
Under these conditions, new refluxing channels must first be created; if incompetent sources of reflux or incompetent venous channels in the thigh are left behind, the development of recurrent reflux is facilitated.
Clinical and Hemodynamic Significance of Recurrent Reflux
Many patients who were symptomatic before treatment remain symptomless or clinically improved after treatment in spite of evident recurrent varicose veins and recurrent reflux documented on DUS.15 18 21 23 Detection of recurrent reflux does not mean clinical relevance; recurrent reflux precedes clinical symptoms for several years. Hartmann et al21 found that recurrent symptoms requiring reoperation appeared in only 7% of limbs with recurrent varicosities 14 years after the primary operation. According to Fischer et al,18 only 21.6% of limbs with reflux recurrences in the groin were sufficiently symptomatic to warrant consideration of additional treatment 34 years after the primary surgery. The results depicted in Fig. 5 showed that 4 years after crossectomy, the strain gauge plethysmographic parameters refill time t = 90 and t = 50 remained still significantly improved in comparison with the preoperative situation, which might explain why 84.2% of patients with congestive symptoms before treatment were symptomless after crossectomy irrespective of whether they had recurrence or not.15 The analysis of the strain gauge plethysmographic parameter refill volume, which can be regarded as the indicator of venous congestion, found the value of 0.4 /100 mL to be the boundary discriminating symptomless patients from patients with congestive symptoms; statistical evaluation showed that this value had the sensitivity of 70.8% and the specificity of 62.5%.15 According to Geier et al23 freedom from recurrent varicose veins was 6.3 years, and freedom from venous symptoms 8.5 years. Most patients experienced a symptom-free interval after initial operation with a mean duration of 7.4 ± 5.5 years.
Abolition of Reflux in the GSV Trunk using Endovenous Ablative Methods
The introduction of EVLA, RFA, and UGFS challenged the well-established surgical experience that flush ligation at the SFJ and resection of the terminal segment of the GSV with its tributaries in combination with stripping was essential to achieve good long-term results. Most authors performing ablative procedures to not carry out SFJ ligation or crossectomy and leave the terminal segment of GSV near the SFJ with a few junctional tributaries untreated. The reported short-term and medium-term results up to 5 years were comparable with those after crossectomy and stripping, which ostensibly questioned the necessity of the flush ligation at the SFJ. Fischer et al18 and Geier et al23 found out that it took 10 years or even more for the symptomatic recurrences to occur after conventional surgery. Because no long-term follow-ups exceeding 10 years after ablative methods without crossectomy or long-term randomized studies are available as yet, the issue whether it is justifiable to abstain from SFJ ligation/crossectomy when performing ablative procedures remains unresolved. Although it was reported that the flow in the GSV stump and its tributaries in the groin after ablative methods was not refluxing at 1 year of follow-up, this might change with time.
From the hemodynamic point of view, it can scarcely be expected that late results after endovenous ablations without SFJ ligation would differ from those after stripping and inadequate crossectomy with residual GSV stump. This may be apparent not before 10 years of follow-up.23
Successful GSV ablation depends on a set of following factors: optimal mode and amount of the energy delivered, laser wavelength, pullback speed, and also on methodological aspects, such as, the use of perivenous infiltration, manual compression over the vein during the procedure and fiber tip position 0.5 to 1 cm below the SFJ. Delivery of optimal heat intensity expressed as joules per cm and/or optimal pullback speed has been shown to reduce the rates of recanalization of the GSV.49 In contrast to that, stripping is much easier to perform and less prone to mishap.
Endovenous ablative methods (EVLA, RFA, and UGFS) are alternatives to surgical stripping. Instead of removing the incompetent venous segment they work by destroying it through thermal or chemical irritation delivered by intravenous catheter. Following events potentially influence the failure rate of endovenous ablative methods: immediate failure to achieve occlusion; recanalization; and recurrent reflux through the untreated incompetent SFJ.
Recanalization of the treated venous channels enables reoccurrence of reflux. But even if recanalization develops, it does not necessarily result in clinical recurrence or symptomatic reflux. Nevertheless, it must be taken into account that any recanalization means that the goal to eliminate reflux in the treated GSV trunk was not fulfilled; it represents a failure in comparison with stripping; stripped GSV cannot get recanalized.
The benefits of ablative methods include fewer complications, quicker return to work, reduced need for general anesthesia, and equivalent recurrence rates during medium-term follow-up. The question remains unanswered whether the benefit of reduced short-term morbidity and convalescence would not be discredited by worse long-term results because of refraining from SFJ ligation/crossectomy, from a procedure that is not burdening for the treated patient and does not cause postoperative troubles. However, it has one substantial downside: it must be performed by a skilled surgeon.
Ablative methods performed without SFJ ligation encompass another potential risk, namely, the extension of the thrombus from the treated GSV through the SFJ into the common femoral vein.50 51 52 Mozes et al50 detected during routine DUS follow-up thrombus extension from the GSV into the common femoral vein after EVLA in three cases (7.7%). In one patient, cava filter was placed to prevent pulmonary embolism. All the three patients remained asymptomatic; the thrombus resolved by 1 month in all of them. According to Wright et al,51 floating thrombus extending from the GSV into the common femoral vein appears roughly in 1 to 7% as a consequence of GSV ablation using laser, radiofrequency, and foam sclerotherapy. This phenomenon was mostly clinically silent, and was detected by DUS examination during the early posttreatment checking. The thrombi were apparent on DUS within 3 to 7 days of treatment, nonocclusive and asymptomatic, and rarely identifiable after 14 days. They caused neither venous obstruction nor symptomatic pulmonary embolism. Similar complications occurred after RFA. Hingorani et al52 reported extension of the occlusive clot filling the treated GSV into the common femoral vein with a floating tail in 15% of cases, as assessed on DUS 10 days after RFA. None of these patients had pulmonary embolism. Overall, three patients with floating common femoral vein clots underwent inferior vena cava filter placement.
SFJ ligation, a procedure not furthermore burdening the treated patient, would have prevented these events, the placement of cava filter in some of them, and would impede the very probable reoccurrence of reflux through the incompetent GSV stump with tributaries in the future.
Endovenous Laser Ablation without Crossectomy
Most EVLA procedures are performed without SFJ ligation.53 54 55 56 57 58 The fate of the tributaries emptying into the terminal part of the GSV and their potential future role in the development of recurrences is not yet cleared; medium-term results reported up to now do not exceed 6 years, most of them relate to only of a few years of follow-up. Even if they showed that the rate of varicose vein and reflux recurrences were comparable with those after conventional surgery, longer follow-ups exceeding 10 years and randomized studies are necessary before the fate of the residual stump at the SFJ and its recurrence potential can be established with certainty.23 The failure rate of GSV closure after EVLA without SFJ ligation was reported to range between 0 and 34%, and was influenced by the wavelength applied, the experience of the performers, and the energy applied. Immediate nonocclusion or early reopening was reported to occur in 2.7%.54 Occlusion rate after 1 to 2 years amounts to over 90%.54 55 57 Nonrefluxing terminal segment of the GSV with one or more tributaries were visible on DUS in 59% 1 year after EVLA without SFJ ligation; no terminal segment of the GSV and no tributaries were detectable in 40%.58
As concerns recanalization, incongruent data were reported in the literature, depending on the technique used and the diameter of the GSV. According to Theivacumar et al53 3.5% of treated GSV showed evidence of recanalization at 12 weeks and 12 months. The GSV diameter diminishes over a period of months following EVLA, and 85% of ablated veins were invisible by 1 year. In the study by Myers and Jolley,56 recanalization following EVLA occurred in 29 of 509 treated GSV (5.6%) over a 5-year period. Most recurrences occurred within the first 18 months, but three late GSV recurrences were detected 3 years after the treatment. This resulted in primary ultrasound success rate at 4 years by life table analysis of 75.7%. There was a trend to worse results in older patients older than 60 years and in limbs with C4–6 classification.56 In another study, occlusion rate after 6 years came to 88.9%.54 Histological examination detected variously organized thrombi containing necrotic inclusions and patent areas in the vein lumen, progressive venous diameter shrinkage and thrombus fibrotic transformation at 12 months. Not occluded segments were found in 18.8%, recanalized short segments in 22.7%, and entirely recanalized saphenous veins in 4.5%. Nonocclusions prevailed in larger veins. The healing process is based on vein thrombosis, fibrosis, and venous atrophy.59
Comparing EVLA and Conventional Surgery
There are a few randomized studies comparing results of EVLA with conventional surgery. The study published by Kalteis et al60 included 100 patients. Postoperative complications were assessed after 4 weeks. Hematomas were significantly smaller after EVLA. No difference was registered between the groups for the CIVIQ quality of life score. According to Rasmussen et al61 62 5-year follow-up of the randomized controlled trial comparing EVLA with conventional surgery did not show any significant difference between the two groups as concern open refluxing GSV, recurrent varicose veins, and improvement in quality of life scores. Postoperative pain and bruising was higher in the surgical group. There was no difference in the meantime to resume normal physical activity. Rass et al63 presented a two-center randomized controlled trial of 400 patients with 2-year follow-up. Clinically observed recurrent varicose veins were similar in both the groups. Duplex-detected saphenofemoral recurrences appeared significantly more frequently after EVLA (p < 0.001). Clinical improvement was similar in both the groups. In a randomized trial published by Lin et al,64 the results were compared at 12 months employing air plethysmography. Improvement of venous volume, venous filling index, and residual volume fraction was detected in both cohorts with no statistical differences between them. Prospective randomized trial by Christenson et al65 presented results of 100 limbs in each group 1 and 2 years after the intervention. Limbs had significantly more postoperative hematomas after conventional surgery than after EVLA. All GSV were occluded immediately after the procedure in both groups. During the follow-up, two patients after the EVLA developed total recanalization of the GSV with symptoms; both underwent SFJ ligation and stripping and were excluded from further follow-up. Two additional limbs in the EVLA group showed long reflux in partially opened GSVs, raising the failure rate to 7.4% at 2 years. Improvement of quality of life was similar in both groups. According to Health Quality Ontario,57 recovery after treatment was significantly quicker after the EVLA than after conventional surgery. Major adverse events occurring after surgery were higher but not significant. Symptom relief and quality of life were similar in both groups. Patient preferences were strongly in favor of EVLA because of less complications, quick recovery, and outpatient scheduling. In a prospective (nonrandomized) study by Theivacumar et al,66 neovascularization in the groin at 2 years was detected in 18% after conventional surgery and in 1% after the EVLA (p = 0.001). In addition, 4.3% of GSVs recanalized at 2 years in the EVLA group, so that the frequency of recurrent varicosities 2 years after surgery and the EVLA was similar.
Articles comparing the EVLA without crossectomy with conventional surgery assessed the visible varicose vein recurrence, the necessity for reoperations, and recurrent reflux by the DUS. Regrettably, they did not evaluate (with one cited exception) the reflux intensity and its impact on the severity of the venous disorders employing plethysmographic methods. The study by Lin et al64 stated no difference in air plethysmographic parameters after 1 year; nevertheless, the situation will presumably look differently 10 years later.
Comparing EVLA without and with SFJ Ligation/Crossectomy
There are a few randomized studies comparing EVLA with and without SFJ ligation. Disselhoff et al67 randomized 86 limbs of 43 patients with bilateral incompetent GSV so that one limb underwent EVLA without SFJ ligation and the other limb underwent EVLA with SFJ ligation. Two-year life table analysis detected freedom from groin recurrence in 83% in the EVLA without SFJ ligation and in 87% with ligation. Overall, 88% of GSVs in the group without ligation and 98% of those with ligation were completely occluded. In the EVLA without ligation group, 9% had no improvement and required additional SFJ ligation at the 6 months' follow-up. The differences were not statistically significant, apparently because of the insufficient sample size in the cohorts, but better results in the SFJ ligation group were looming. Venous clinical severity score improved significantly in both the groups. A further study by Disselhoff et al68 reanalyzed 60 limbs 5 years after the procedures. Only patients with uncomplicated C2 varicose veins were included. Freedom from groin recurrence was found in 79% of limbs in the EVLA without SFJ ligation and in 65% of limbs with SFJ ligation. An interesting phenomenon occurred during the follow-up: until 40 months, the Kaplan–Meier life table analysis of freedom from duplex-confirmed recurrence showed better results in the group with SFJ ligation; thereafter, in the time span between 40 and 60 months, the situation changed: better results were registered in the group without SFJ ligation. The authors did not explain this phenomenon neither did comment on the hemodynamic consequence resulting from the different GSV occlusion rates: 88% of GSVs were occluded in the cohort without SFJ ligation, and 98% of the cohort with SFJ ligation. Moreover, four limbs in the EVLA group without SFJ ligation had varicose vein recurrence and no improvement in venous clinical severity score requiring additional SFJ ligation at the 6-month follow-up. In another comparative study presented by Longhini et al,69 the DUS detected the absence of GSV flow in the EVLA/high ligation cohort amounted to 92.0%, whereas in the EVLA/without SFJ ligation cohort to only 54.6%; the difference was statistically significant (p < 0.01), documenting that distinctly better results were achieved after the EVLA with SFJ ligation than after the EVLA without ligation. Flessenkämper et al70 presented a multicenter, randomized, three-arm study encompassing 449 patients during a follow-up of 2 months. The following three cohorts were compared: EVLA without SFJ ligation, EVLA with SFJ ligation, and surgical cohort with SFJ ligation and stripping. Reflux in the groin was detected in 8.5% after EVLA without SFJ ligation, in 2.2% after the EVLA with SFJ ligation, and in none in the surgical cohort.
Radiofrequency Ablation
In the multicenter prospective study published by Merchant et al,49 immediate GSV occlusion at 1 week was achieved in 96.8% (i.e., 3.2% anatomical failures). At 5 years, 87.2% were occluded (12.8% failures). There was no mention about the fate of the GSV tributaries in the groin. Similar occlusion rates ranging between 75 and 87.2% 3 to 5 years after RFA were published in other articles.71 72 73 74 75 Lurie et al72 73 presented the results of RFA in 44 patients from five centers (France, 2; Austria, 1; and the United States, 2). Immediate success on the day of treatment was recorded in 95%. At 3 weeks, 13.6% had reflux in the treated GSV but at 4 years, 92% of the treated GSVs were occluded; the reason for this amelioration was not mentioned. The closed GSVs underwent progressive shrinkage to eventual sonographic disappearance. Recanalization was related to several factors, including vein diameter and energy delivered. Adequate pullback speed to ensure proper thermal dose delivery has been shown to reduce the rates of recanalization of saphenous vein. The 2-year clinical results of RFA, that is, varicose vein recurrences, corresponded to those after SFJ ligation and stripping. Analogous results were published by Pichot et al.74 GSV truncal occlusion was observed in 90% of treated GSVs; 9.5% were anatomical failures. Two years after RFA, the most common duplex finding in the groin was an open SFJ and patent, approximately 5 cm large terminal GSV segment with tributaries. Despite the presence of 104 patent junctional tributaries, SFJ reflux was uncommon, affecting allegedly only five limbs. This finding is, of course, worrying: a few years later, incompetent SFJ and GSV stump with tributaries might become the origin of recurrent reflux. According to the Health Quality Ontario study,75 the overall level of evidence of randomized studies comparing RFA with surgical ligation and vein stripping was graded as low to moderate. Recovery after treatment was significantly quicker after RFA both with return to usual activity and return to work with on average a 1 week less of work loss. Major adverse events occurring after surgery were higher than after RFA but not significant.
Fate of GSV Tributaries in the Groin after GSV Endovenous Ablation
One or more patent tributaries were seen in continuity with the SFJ in 59% of cases 1 year after ELVA.58 Chandler et al76 published a prospective multicenter nonrandomized study assessing results after RFA: 60 limbs were treated with SFJ ligation in addition to RFA, 120 limbs were treated with RFA alone. Overall, 35% of limbs without SFJ ligation had one or more SFJ tributaries 6 months after treatment; the external pudendal vein was the most commonly identified open tributary. SFJ duplex scan anatomy was studied serially (1 week, 6 weeks, 6 months) in 15 limbs treated by RFA without SFJ ligation. One-third of the limbs studied showed complete occlusion of the GSV up to the SFJ 1 week after treatment. By 6 months, only 1 of the 15 SFJ remained completely occluded; the other 14 (93%) had at least one open tributary, documenting the progressive opening of the terminal 1 to 2 cm long segment of the GSV with tributaries at the SFJ. Even though the flow at 6 months was reported to be prograde, this situation can change in the future; it can be likened to that one after incomplete crossectomy, and might be regarded as the first step in the process leading to reflux recurrence.
The results document that if SFJ ligation is not performed in addition to endovenous GSV ablations, the terminal part of the GSV with tributaries at the SFJ remains patent in most cases and embodies the risk to become the origin of recurrent reflux in the course of time.
Foam Sclerotherapy
Bergan et al77 presented experience in treating 332 patients with UGFS. The efficacy in terms of immediate venous occlusion was over 80%. Following complications were recorded: dry cough, visual disturbances, chest tightness, and myoclonus. The most troublesome adverse event is thought to be because of foam reaching the lung or escaping into the left heart through a patent foramen ovale. If this occurs and causes any untoward event, it does so during or immediately after the introduction of foam into the venous system; such an event occurred in 4% of the total experience. According to the study by Badri and Bhattacharya,78 the recurrence rate after UGFS reached 30.5% after 1 year, and 51% after 10 years. Nicolini et al71 presented results of a prospective study from eight centers. Occlusion of GSV was 81% by 1 year and 75% by 3 years. Shadid et al79 presented a randomized clinical trial of USGFS versus conventional surgery. At 2 years, reflux was significantly more frequent in the UGFS group with 35.0% than in the surgery group with 21.0% (p = 0.003). In the 5-year prospective study by Chapman-Smith and Browne80 serial annual DUS demonstrated recurrence in 27% at 12 months, and in 64% at 5 years after UGFS. The reflux was regarded as clinically insignificant. Lattimer et al81 compared UGFS versus EVLA and found that occlusion of the GSV was more effective with the EVLA at 95.5% versus UGFS at 67.4%.
Meta-Analysis of Results after EVLA, RFA, and UGFS
Luebke and Brunkwall82 performed a meta-analysis study comparing EVLA, RFA, and UGFS. EVLA had the best results concerning the long-term effectiveness parameters “occlusion at the end of follow-up” and “recanalization, recurrence or development of new veins.” UGFS was associated with higher recurrence rate in comparison with EVLA and RFA treatment. By 48 months, recanalization of the GSV occurred in 4.5% after EVLA, in 8.4% after RFA, and in 15.5% after UGFS. Occlusion rate was approximately 95% after 2 years for EVLA and almost 90% after 5 years for RFA.
Randomized Studies comparing EVLA, UGFS, and SFJ Ligation with Stripping (SFJL/S)
Biemans et al83 presented a 1-year follow-up comparative randomized study including 240 consecutive patients. After 1 year, the anatomic success rate (no reflux in the GSV in the thigh) was higher after the EVLA (88.5%) and SFJL/S (88.2%) than after UGFS (72.2%) (p < 0.001). The authors did not explain why there was merely 88.2% success after SFJL/S; the possible reason might be that only short stripping in the thigh was performed, so that the remaining 11.8% in the surgical cohort might be labeled as inadequate stripping. The complication rate was low and comparable between the treatment groups. All groups showed significant improvement of quality of life scores. In the SFJL/S group, 10% of patients had neovascularization on ultrasound examination of the groin (tiny new vein up to 3 mm diameter, not connecting with any superficial vein). Regrettably, the fate of the nontreated terminal segment of the GSV with tributaries in the EVLA and UGFS groups was not mentioned. Overall, 27.3% of the UGFS had partial obliteration of the GSV with reflux.
Assessment of Endovenous Ablative Methods
CEAP clinical class and symptom scores were significantly improved and comparable both after ablative methods and conventional surgery at the end of short-term and medium-term follow-ups.
Endovenous ablative methods (EVLA, RFA, and UGFS) intend to eliminate reflux in the incompetent GSV and leave the origin of reflux in the SFJ undisturbed, which is the main difference in comparison with conventional surgery. Comparison of results achieved after ablative methods showed that anatomical failures (nonocclusion of the treated GSV) occurred more frequently after UGFS than after EVLA and RFA. Substitution of stripping by endovenous ablation has some advantages including fewer immediate posttreatment discomfort, quicker return to work, and reduced need for general anesthesia; that is why endovenous ablation is better tolerated and preferred by the patients. Nevertheless, leaving the source of reflux untouched constitutes a possible substantial downside: it is very probable that the results after a follow-up exceeding 10 years will comply with those after stripping and inadequate crossectomy. Comprehensive surgical experience showed that incompetent SFJ with incompetent terminal segment of the GSV and tributaries (in German “Venenstern,” i.e., venous star) was the most common source of hemodynamically important recurrent reflux. Although the short-term and medium-term results achieved after the EVLA and RFA without SFJ ligation are comparable with those after the SFJ ligation and stripping, they do not justify refraining from SFJ ligation. As long as it would not be confirmed by long-term and very long term randomized studies that refraining from interruption of the source of GSV reflux is acceptable, SFJ ligation should remain the integral part of the therapy of varicose vein disease.
Summary
Saphenous reflux can be abolished by eliminating either the source of reflux or the reflux-carrying incompetent vein(s); both measures remove the hemodynamic disturbance and restore physiological decrease in pressure during calf pump activity. Unfortunately, the excellent hemodynamic effect dwindles progressively in the course of time because of the increasing intensity of recurrent reflux, and the hemodynamic disturbance tends to supervene again. The process generating reappearance of reflux is triggered by the ambulatory pressure gradient. New venous connections inducing recurrent reflux develop because of the vascular remodeling, which means progressive dilatation of preformed tiny, and hitherto functionless communicating channels connecting the femoral vein and the saphenous system in the thigh; fluid shear stress and vasoactive agents play a significant role in this process. Vascular remodeling in the groin takes place after correctly performed surgery. If inadequate surgery or deliberate refraining from ligation of SFJ leaves behind an incompetent terminal part of GSV with tributaries, recurrent reflux takes place through these channels. Residual branches at the SFJ are the favorable point of origin, residual remnants of incompetent saphenous system in the thigh are connector paths; both accelerate reoccurrence of reflux. If residual branches or connector paths are not present, the recurrent reflux-carrying vessels are created in their entirety, which takes up more time.
Randomized prospective studies showed that GSV stripping adds significant recurrent reflux protection, as compared to pure crossectomy.
Ablative methods represent alternatives to stripping; they are sufficiently effective, cause less postoperative discomfort in comparison with stripping, and will probably replace stripping in the future. When performed without SFJ ligation, they provide the following two potential sources for recurrent reflux: incompetent SFJ with junctional tributaries, and possible recanalization of the treated GSV; some studies showed that recanalization of the treated GSV occurs more frequently if ligation of the SFJ has been omitted. It must be born in mind that each recanalization of the GSV after endovenous ablation represents a failure in comparison with stripping; the stripped vein cannot get recanalized.
To achieve the most favorable therapeutic results when treating varicose vein disease, it is necessary to eliminate both the reflux source(s) and the reflux-carrying channel(s); leaving behind either incompletely abolished reflux sources or incompetent veins in the thigh expedites recurrences. It can be presumed that ablative methods performed without SFJ ligation, if evaluated in future studies with a time interval exceeding 10 years, will yield results comparable with those after incomplete crossectomy and stripping; the hemodynamic preconditions setting off recurrent reflux resemble in both these situations. Studies comparing the results after ablative methods with and without SFJ ligation yielded some evidences hinting in that direction. Unfortunately, it must be acknowledged that even if all possible refluxing sources and communications have been removed, new incompetent channels created by vascular remodeling tend to occur in the posttreatment period with progressively increasing recurrent reflux; it is impossible to reliably hinder the reappearance of reflux.
It is not only a matter of the presence of recurrent reflux, but importantly it is the matter of its intensity. Many symptomatic patients remain symptomless after treatment in spite of proven recurrent reflux; this points to the lesser intensity of recurrent reflux in comparison with the pretreatment situation. Plethysmographic parameters are able to quantify the degree of hemodynamic disturbance caused by reflux, and to yield values that can be statistically evaluated. Regrettably, in studies dealing with ablative methods the results were not evaluated by plethysmographic methods. In randomized future studies that will compare endovenous ablative procedures with conventional surgery, plethysmographic evaluation of the results should not be lacking.
Because no therapeutic procedure treating varicose vein disease is capable to transform all incompetent superficial veins in the thigh into competent ones and to preclude centrifugal drainage of venous blood into deep lower leg veins, it is not possible to heal varicose vein disease definitely, and we must reconcile to the fact that recurrences tend to occur after any mode of therapy.
References
- 1.Höjensgard I C, Stürup H. Static and dynamic pressures in superficial and deep veins of the lower extremity in man. Acta Physiol Scand. 1952;27(1):49–67. doi: 10.1111/j.1748-1716.1953.tb00923.x. [DOI] [PubMed] [Google Scholar]
- 2.Arnoldi C C. Venous pressure in the legs of healthy human subjects at rest and during muscular exercise in nearly erect position. Acta Chir Scand. 1965;130:530–583. [PubMed] [Google Scholar]
- 3.Recek C, Pojer H. Ambulatory pressure gradient in the veins of the lower extremity. Vasa. 2000;29(3):187–190. doi: 10.1024/0301-1526.29.3.187. [DOI] [PubMed] [Google Scholar]
- 4.Recek C. Calf pump activity influencing venous hemodynamics in the lower extremity. Int J Angiol. 2013;22(1):23–30. doi: 10.1055/s-0033-1334092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Recek C. The hemodynamic paradox as a phenomenon triggering recurrent reflux in varicose vein disease. Int J Angiol. 2012;21(3):181–186. doi: 10.1055/s-0032-1325168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pipp F, Boehm S, Cai W J. et al. Elevated fluid shear stress enhances postocclusive collateral artery growth and gene expression in the pig hind limb. Arterioscler Thromb Vasc Biol. 2004;24(9):1664–1668. doi: 10.1161/01.ATV.0000138028.14390.e4. [DOI] [PubMed] [Google Scholar]
- 7.Schaper W, Scholz D. Factors regulating arteriogenesis. Arterioscler Thromb Vasc Biol. 2003;23(7):1143–1151. doi: 10.1161/01.ATV.0000069625.11230.96. [DOI] [PubMed] [Google Scholar]
- 8.Resnick N, Gimbrone M A Jr. Hemodynamic forces are complex regulators of endothelial gene expression. FASEB J. 1995;9(10):874–882. doi: 10.1096/fasebj.9.10.7615157. [DOI] [PubMed] [Google Scholar]
- 9.Schierling W, Troidl K, Troidl C, Schmitz-Rixen T, Schaper W, Eitenmüller I K. The role of angiogenic growth factors in arteriogenesis. J Vasc Res. 2009;46(4):365–374. doi: 10.1159/000189797. [DOI] [PubMed] [Google Scholar]
- 10.El Wajeh Y, Giannoukas A D, Gulliford C J, Suvarna S K, Chan P. Saphenofemoral venous channels associated with recurrent varicose veins are not neovascular. Eur J Vasc Endovasc Surg. 2004;28(6):590–594. doi: 10.1016/j.ejvs.2004.09.011. [DOI] [PubMed] [Google Scholar]
- 11.Trendelenburg F. Ligation of the great saphenous vein in varicose veins of the lower leg (German) Beitr Klin Chir. 1891;7:195–210. [Google Scholar]
- 12.Perthes G. The operation of varicose veins of the lower leg according to Trendelenburg (German) Dtsch Med Wochenschr. 1895;21:253–257. [Google Scholar]
- 13.Recek C. The impact of crossectomy on the venous hemodynamics in primary varicose veins (German) Phlebologie. 1996;25:11–18. [Google Scholar]
- 14.Recek C. Saphenous reflux as the cause of severe hemodynamic disturbance in primary varicose veins and chronic venous insufficiency (German) Acta Chir Austriaca. 1998;30:76–77. [Google Scholar]
- 15.Recek C. Medium-term results after crossectomy combined with sclerotherapy (German) Phlebologie. 2000;29:23–26. [Google Scholar]
- 16.Ludbrook J, Beale G. Femoral venous valves in relation to varicose veins. Lancet. 1962;1(7220):79–81. doi: 10.1016/s0140-6736(62)91724-5. [DOI] [PubMed] [Google Scholar]
- 17.Perrin M R, Guex J J, Ruckley C V. et al. Recurrent varices after surgery (REVAS), a consensus document. REVAS group. Cardiovasc Surg. 2000;8(4):233–245. doi: 10.1177/096721090000800402. [DOI] [PubMed] [Google Scholar]
- 18.Fischer R, Linde N, Duff C, Jeanneret C, Chandler J G, Seeber P. Late recurrent saphenofemoral junction reflux after ligation and stripping of the greater saphenous vein. J Vasc Surg. 2001;34(2):236–240. doi: 10.1067/mva.2001.115802. [DOI] [PubMed] [Google Scholar]
- 19.Kostas T, Ioannou C V, Touloupakis E. et al. Recurrent varicose veins after surgery: a new appraisal of a common and complex problem in vascular surgery. Eur J Vasc Endovasc Surg. 2004;27(3):275–282. doi: 10.1016/j.ejvs.2003.12.006. [DOI] [PubMed] [Google Scholar]
- 20.Winterborn R J, Foy C, Earnshaw J J. Causes of varicose vein recurrence: late results of a randomized controlled trial of stripping the long saphenous vein. J Vasc Surg. 2004;40(4):634–639. doi: 10.1016/j.jvs.2004.07.003. [DOI] [PubMed] [Google Scholar]
- 21.Hartmann K, Klode J, Pfister R. et al. Recurrent varicose veins: sonography-based re-examination of 210 patients 14 years after ligation and saphenous vein stripping. Vasa. 2006;35(1):21–26. doi: 10.1024/0301-1526.35.1.21. [DOI] [PubMed] [Google Scholar]
- 22.Allegra C, Antignani P L, Carlizza A. Recurrent varicose veins following surgical treatment: our experience with five years follow-up. Eur J Vasc Endovasc Surg. 2007;33(6):751–756. doi: 10.1016/j.ejvs.2006.12.020. [DOI] [PubMed] [Google Scholar]
- 23.Geier B, Stücker M, Hummel T. et al. Residual stumps associated with inguinal varicose vein recurrences: a multicenter study. Eur J Vasc Endovasc Surg. 2008;36(2):207–210. doi: 10.1016/j.ejvs.2008.03.013. [DOI] [PubMed] [Google Scholar]
- 24.Nelzén O, Fransson I. Varicose vein recurrence and patient satisfaction 10-14 years following combined superficial and perforator vein surgery: a prospective case study. Eur J Vasc Endovasc Surg. 2013;46(3):372–377. doi: 10.1016/j.ejvs.2013.05.022. [DOI] [PubMed] [Google Scholar]
- 25.Bradbury A W, Stonebridge P A, Callam M J. et al. Recurrent varicose veins: assessment of the saphenofemoral junction. Br J Surg. 1994;81(3):373–375. doi: 10.1002/bjs.1800810316. [DOI] [PubMed] [Google Scholar]
- 26.Tong Y, Royle J. Recurrent varicose veins following high ligation of long saphenous vein: a duplex ultrasound study. Cardiovasc Surg. 1995;3(5):485–487. doi: 10.1177/096721099500300508. [DOI] [PubMed] [Google Scholar]
- 27.Viani M P, Poggi R V, Pinto A, Andreani S M, Spagnoli C, Maruotti R A. Re-exploration of the saphenofemoral junction in the treatment of recurrent varicose veins. Int Surg. 1996;81(4):382–384. [PubMed] [Google Scholar]
- 28.Jiang P, van Rij A M, Christie R, Hill G, Solomon C, Thomson I. Recurrent varicose veins: patterns of reflux and clinical severity. Cardiovasc Surg. 1999;7(3):332–339. doi: 10.1177/096721099900700311. [DOI] [PubMed] [Google Scholar]
- 29.Egan B Donnelly M Bresnihan M Tierney S Feeley M Neovascularization: an “innocent bystander” in recurrent varicose veins J Vasc Surg 20064461279–1284., discussion 1284 [DOI] [PubMed] [Google Scholar]
- 30.Bartos J Jr, Bartos J. Causes of recurrencies following procedures for varicose veins of the lower extremities[in Czech] Rozhl Chir. 2006;85(6):293–295. [PubMed] [Google Scholar]
- 31.Gabriel M, Zieliński P, Pawlaczyk K, Krasiński Z, Stanisić M, Dzieciuchowicz Ł. The analyze of recurrent varicose veins development after surgical treatment of lower limbs varicose veins [in Polish] Przegl Lek. 2011;68(3):161–166. [PubMed] [Google Scholar]
- 32.Stonebridge P A, Chalmers N, Beggs I, Bradbury A W, Ruckley C V. Recurrent varicose veins: a varicographic analysis leading to a new practical classification. Br J Surg. 1995;82(1):60–62. doi: 10.1002/bjs.1800820121. [DOI] [PubMed] [Google Scholar]
- 33.Winterborn R J, Earnshaw J J. Crossectomy and great saphenous vein stripping. J Cardiovasc Surg (Torino) 2006;47(1):19–33. [PubMed] [Google Scholar]
- 34.Sarin S, Scurr J H, Coleridge Smith P D. Assessment of stripping the long saphenous vein in the treatment of primary varicose veins. Br J Surg. 1992;79(9):889–893. doi: 10.1002/bjs.1800790911. [DOI] [PubMed] [Google Scholar]
- 35.Sarin S, Scurr J H, Coleridge Smith P D. Stripping of the long saphenous vein in the treatment of primary varicose veins. Br J Surg. 1994;81(10):1455–1458. doi: 10.1002/bjs.1800811017. [DOI] [PubMed] [Google Scholar]
- 36.Dwerryhouse S, Davies B, Harradine K, Earnshaw J J. Stripping the long saphenous vein reduces the rate of reoperation for recurrent varicose veins: five-year results of a randomized trial. J Vasc Surg. 1999;29(4):589–592. doi: 10.1016/s0741-5214(99)70302-2. [DOI] [PubMed] [Google Scholar]
- 37.Jones L, Braithwaite B D, Selwyn D, Cooke S, Earnshaw J J. Neovascularisation is the principal cause of varicose vein recurrence: results of a randomised trial of stripping the long saphenous vein. Eur J Vasc Endovasc Surg. 1996;12(4):442–445. doi: 10.1016/s1078-5884(96)80011-6. [DOI] [PubMed] [Google Scholar]
- 38.Glass G M. Neovascularization in recurrence of the varicose great saphenous vein following transection. Phlebology. 1987;2:81–91. [Google Scholar]
- 39.Turton E P, Scott D J, Richards S P. et al. Duplex-derived evidence of reflux after varicose vein surgery: neoreflux or neovascularisation? Eur J Vasc Endovasc Surg. 1999;17(3):230–233. doi: 10.1053/ejvs.1998.0719. [DOI] [PubMed] [Google Scholar]
- 40.van Rij A M, Jones G T, Hill G B, Jiang P. Neovascularization and recurrent varicose veins: more histologic and ultrasound evidence. J Vasc Surg. 2004;40(2):296–302. doi: 10.1016/j.jvs.2004.04.031. [DOI] [PubMed] [Google Scholar]
- 41.Nyamekye I, Shephard N A, Davies B, Heather B P, Earnshaw J J. Clinicopathological evidence that neovascularisation is a cause of recurrent varicose veins. Eur J Vasc Endovasc Surg. 1998;15(5):412–415. doi: 10.1016/s1078-5884(98)80202-5. [DOI] [PubMed] [Google Scholar]
- 42.Munn S R, Morton J B, Macbeth W A, Mcleish A R. To strip or not to strip the long saphenous vein? A varicose veins trial. Br J Surg. 1981;68(6):426–428. doi: 10.1002/bjs.1800680621. [DOI] [PubMed] [Google Scholar]
- 43.Rutgers P H, Kitslaar P J. Randomized trial of stripping versus high ligation combined with sclerotherapy in the treatment of the incompetent greater saphenous vein. Am J Surg. 1994;168(4):311–315. doi: 10.1016/s0002-9610(05)80155-2. [DOI] [PubMed] [Google Scholar]
- 44.Raivio P, Perhoniemi V, Lehtola A. Long-term results of vein sparing varicose vein surgery. World J Surg. 2002;26(12):1507–1511. doi: 10.1007/s00268-002-6375-8. [DOI] [PubMed] [Google Scholar]
- 45.Casoni P, Lefebvre-Vilardebo M, Villa F, Corona P. Great saphenous vein surgery without high ligation of the saphenofemoral junction. J Vasc Surg. 2013;58(1):173–178. doi: 10.1016/j.jvs.2012.11.116. [DOI] [PubMed] [Google Scholar]
- 46.Brake M, Lim C S, Shepherd A C, Shalhoub J, Davies A H. Pathogenesis and etiology of recurrent varicose veins. J Vasc Surg. 2013;57(3):860–868. doi: 10.1016/j.jvs.2012.10.102. [DOI] [PubMed] [Google Scholar]
- 47.Blomgren L, Johansson G, Dahlberg-AKerman A. et al. Recurrent varicose veins: incidence, risk factors and groin anatomy. Eur J Vasc Endovasc Surg. 2004;27(3):269–274. doi: 10.1016/j.ejvs.2003.12.022. [DOI] [PubMed] [Google Scholar]
- 48.Mouton W G, Marklewitz M M, Friedli S. et al. Neovascularisation after surgery for recurrent saphenofemoral incompetence: does surgical dissection technique matter? Vasa. 2011;40(4):296–301. doi: 10.1024/0301-1526/a000118. [DOI] [PubMed] [Google Scholar]
- 49.Merchant R F Pichot O; Closure Study Group. Long-term outcomes of endovenous radiofrequency obliteration of saphenous reflux as a treatment for superficial venous insufficiency J Vasc Surg 2005423502–509., discussion 509 [DOI] [PubMed] [Google Scholar]
- 50.Mozes G, Kalra M, Carmo M, Swenson L, Gloviczki P. Extension of saphenous thrombus into the femoral vein: a potential complication of new endovenous ablation techniques. J Vasc Surg. 2005;41(1):130–135. doi: 10.1016/j.jvs.2004.10.045. [DOI] [PubMed] [Google Scholar]
- 51.Wright D, Morrison N, Recek C, Passariello F. Post ablation superficial thrombus extension (PASTE) into the commons femoral vein as a consequence of endovenous ablation of the great saphenous vein. Acta Phlebol. 2010;11:59–64. [Google Scholar]
- 52.Hingorani A P, Ascher E, Markevich N. et al. Deep venous thrombosis after radiofrequency ablation of greater saphenous vein: a word of caution. J Vasc Surg. 2004;40(3):500–504. doi: 10.1016/j.jvs.2004.04.032. [DOI] [PubMed] [Google Scholar]
- 53.Theivacumar N S, Dellagrammaticas D, Darwood R J, Mavor A I, Gough M J. Fate of the great saphenous vein following endovenous laser ablation: does re-canalisation mean recurrence? Eur J Vasc Endovasc Surg. 2008;36(2):211–215. doi: 10.1016/j.ejvs.2008.03.014. [DOI] [PubMed] [Google Scholar]
- 54.Kaspar S, Pirkl M, Príborská J, Kaspar D. A six-year experience with endovenous laser in the treatment of lower extremity varices [in Czech] Rozhl Chir. 2009;88(3):106–114. [PubMed] [Google Scholar]
- 55.Pannier F, Rabe E. Endovenous laser therapy and radiofrequency ablation of saphenous varicose veins. J Cardiovasc Surg (Torino) 2006;47(1):3–8. [PubMed] [Google Scholar]
- 56.Myers K A, Jolley D. Outcome of endovenous laser therapy for saphenous reflux and varicose veins: medium-term results assessed by ultrasound surveillance. Eur J Vasc Endovasc Surg. 2009;37(2):239–245. doi: 10.1016/j.ejvs.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 57.Health Quality Ontario . Endovascular laser therapy for varicose veins: an evidence-based analysis. Ont Health Technol Assess Ser. 2010;10(6):1–92. [PMC free article] [PubMed] [Google Scholar]
- 58.Theivacumar N S, Dellagrammaticas D, Beale R J, Mavor A I, Gough M J. Fate and clinical significance of saphenofemoral junction tributaries following endovenous laser ablation of great saphenous vein. Br J Surg. 2007;94(6):722–725. doi: 10.1002/bjs.5804. [DOI] [PubMed] [Google Scholar]
- 59.Corcos L, Dini S, Peruzzi G, Pontello D, Dini M, De Anna D. Duplex ultrasound changes in the great saphenous vein after endosaphenous laser occlusion with 808-nm wavelength. J Vasc Surg. 2008;48(5):1262–1271. doi: 10.1016/j.jvs.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 60.Kalteis M Berger I Messie-Werndl S et al. High ligation combined with stripping and endovenous laser ablation of the great saphenous vein: early results of a randomized controlled study J Vasc Surg 2008474822–829., discussion 829 [DOI] [PubMed] [Google Scholar]
- 61.Rasmussen L H, Bjoern L, Lawaetz M, Blemings A, Lawaetz B, Eklof B. Randomized trial comparing endovenous laser ablation of the great saphenous vein with high ligation and stripping in patients with varicose veins: short-term results. J Vasc Surg. 2007;46(2):308–315. doi: 10.1016/j.jvs.2007.03.053. [DOI] [PubMed] [Google Scholar]
- 62.Rasmussen L, Lawaetz M, Bjoern L, Blemings A, Eklof B. Randomized clinical trial comparing endovenous laser ablation and stripping of the great saphenous vein with clinical and duplex outcome after 5 years. J Vasc Surg. 2013;58(2):421–426. doi: 10.1016/j.jvs.2012.12.048. [DOI] [PubMed] [Google Scholar]
- 63.Rass K, Frings N, Glowacki P. et al. Comparable effectiveness of endovenous laser ablation and high ligation with stripping of the great saphenous vein: two-year results of a randomized clinical trial (RELACS study) Arch Dermatol. 2012;148(1):49–58. doi: 10.1001/archdermatol.2011.272. [DOI] [PubMed] [Google Scholar]
- 64.Lin Y, Ye C S, Huang X L, Ye J L, Yin H H, Wang S M. A random, comparative study on endovenous laser therapy and saphenous veins stripping for the treatment of great saphenous vein incompetence in Chinese] Zhonghua Yi Xue Za Zhi. 2007;87(43):3043–3046. [PubMed] [Google Scholar]
- 65.Christenson J T, Gueddi S, Gemayel G, Bounameaux H. Prospective randomized trial comparing endovenous laser ablation and surgery for treatment of primary great saphenous varicose veins with a 2-year follow-up. J Vasc Surg. 2010;52(5):1234–1241. doi: 10.1016/j.jvs.2010.06.104. [DOI] [PubMed] [Google Scholar]
- 66.Theivacumar N S, Darwood R, Gough M J. Neovascularisation and recurrence 2 years after varicose vein treatment for sapheno-femoral and great saphenous vein reflux: a comparison of surgery and endovenous laser ablation. Eur J Vasc Endovasc Surg. 2009;38(2):203–207. doi: 10.1016/j.ejvs.2009.03.031. [DOI] [PubMed] [Google Scholar]
- 67.Disselhoff B C, der Kinderen D J, Kelder J C, Moll F L. Randomized clinical trial comparing endovenous laser ablation of the great Saphenous vein with and without ligation of the sapheno-femoral junction: 2-year results. Eur J Vasc Endovasc Surg. 2008;36(6):713–718. doi: 10.1016/j.ejvs.2008.08.015. [DOI] [PubMed] [Google Scholar]
- 68.Disselhoff B C, der Kinderen D J, Kelder J C, Moll F L. Five-year results of a randomised clinical trial of endovenous laser ablation of the great saphenous vein with and without ligation of the saphenofemoral junction. Eur J Vasc Endovasc Surg. 2011;41(5):685–690. doi: 10.1016/j.ejvs.2010.12.014. [DOI] [PubMed] [Google Scholar]
- 69.Longhini A, Borelli P, Franzini M, Kazemian A R, Munarini G, Marcolli G. Combination of endovenous laser treatment and a surgical approach for venous disease [in Italian] Chir Ital. 2007;59(4):475–479. [PubMed] [Google Scholar]
- 70.Flessenkämper I, Hartmann M, Stenger D, Roll S. Endovenous laser ablation with and without high ligation compared with high ligation and stripping in the treatment of great saphenous varicose veins: initial results of a multicentre randomized controlled trial. Phlebology. 2013;28(1):16–23. doi: 10.1258/phleb.2011.011147. [DOI] [PubMed] [Google Scholar]
- 71.Nicolini P; Closure Group. Treatment of primary varicose veins by endovenous obliteration with the VNUS closure system: results of a prospective multicentre study Eur J Vasc Endovasc Surg 2005294433–439. [DOI] [PubMed] [Google Scholar]
- 72.Lurie F, Creton D, Eklof B. et al. Prospective randomised study of endovenous radiofrequency obliteration (closure) versus ligation and vein stripping (EVOLVeS): two-year follow-up. Eur J Vasc Endovasc Surg. 2005;29(1):67–73. doi: 10.1016/j.ejvs.2004.09.019. [DOI] [PubMed] [Google Scholar]
- 73.Lurie F, Creton D, Eklof B. et al. Reprinted article “Prospective randomised study of endovenous radiofrequency obliteration (closure) versus ligation and vein stripping (EVOLVeS): two-year follow-up”. Eur J Vasc Endovasc Surg. 2011;42 01:S107–S113. doi: 10.1016/j.ejvs.2011.06.019. [DOI] [PubMed] [Google Scholar]
- 74.Pichot O, Kabnick L S, Creton D, Merchant R F, Schuller-Petroviae S, Chandler J G. Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration. J Vasc Surg. 2004;39(1):189–195. doi: 10.1016/j.jvs.2003.07.015. [DOI] [PubMed] [Google Scholar]
- 75.Health Quality Ontario . Endovascular radiofrequency ablation for varicose veins: an evidence-based analysis. Ont Health Technol Assess Ser. 2011;11(1):1–93. [PMC free article] [PubMed] [Google Scholar]
- 76.Chandler J G, Pichot O, Sessa C, Schuller-Petrović S, Osse F J, Bergan J J. Defining the role of extended saphenofemoral junction ligation: a prospective comparative study. J Vasc Surg. 2000;32(5):941–953. doi: 10.1067/mva.2000.110348. [DOI] [PubMed] [Google Scholar]
- 77.Bergan J, Pascarella L, Mekenas L. Venous disorders: treatment with sclerosant foam. J Cardiovasc Surg (Torino) 2006;47(1):9–18. [PubMed] [Google Scholar]
- 78.Badri H, Bhattacharya V. A review of current treatment strategies for varicose veins. Recent Patents Cardiovasc Drug Discov. 2008;3(2):126–136. doi: 10.2174/157489008784705304. [DOI] [PubMed] [Google Scholar]
- 79.Shadid N, Ceulen R, Nelemans P. et al. Randomized clinical trial of ultrasound-guided foam sclerotherapy versus surgery for the incompetent great saphenous vein. Br J Surg. 2012;99(8):1062–1070. doi: 10.1002/bjs.8781. [DOI] [PubMed] [Google Scholar]
- 80.Chapman-Smith P, Browne A. Prospective five-year study of ultrasound-guided foam sclerotherapy in the treatment of great saphenous vein reflux. Phlebology. 2009;24(4):183–188. doi: 10.1258/phleb.2009.008080. [DOI] [PubMed] [Google Scholar]
- 81.Lattimer C R, Kalodiki E, Azzam M, Makris G C, Somiayajulu S, Geroulakos G. Interim results on abolishing reflux alongside a randomized clinical trial on laser ablation with phlebectomies versus foam sclerotherapy. Int Angiol. 2013;32(4):394–403. [PubMed] [Google Scholar]
- 82.Luebke T, Brunkwall J. Systematic review and meta-analysis of endovenous radiofrequency obliteration, endovenous laser therapy, and foam sclerotherapy for primary varicosis. J Cardiovasc Surg (Torino) 2008;49(2):213–233. [PubMed] [Google Scholar]
- 83.Biemans A A, Kockaert M, Akkersdijk G P. et al. Comparing endovenous laser ablation, foam sclerotherapy, and conventional surgery for great saphenous varicose veins. J Vasc Surg. 2013;58(3):727–340. doi: 10.1016/j.jvs.2012.12.074. [DOI] [PubMed] [Google Scholar]