

Abstract
Oxidized regenerated cellulose (Ethicon Surgicel) is often used during surgery to achieve hemostasis. The appearance of Surgicel on postoperative computed tomography (CT) may be mistaken for abscess. Meanwhile, the literature regarding its ultrasound appearance remains scant. We report the CT and sonographic appearances of Surgicel in the right ovary of a 21-year-old woman presenting to the emergency department with pelvic pain 7 days after ovarian cystectomy. The patient was discharged home with only supportive measures, and follow-up ultrasound obtained 26 days later demonstrated resolution of the sonographic abnormality. This case stresses the importance of familiarity with common imaging appearances of topical hemostatic agents and the need to correlate radiologic findings with the patient's clinical condition and prior operative reports to identify patients suitable for conservative management.
Keywords: Surgicel, Abscess, Torsion, Computed tomography, Ultrasound
Introduction
Surgicel (Ethicon, Inc, a Johnson & Johnson company) is a resorbable agent composed of oxidized cellulose polymer used to achieve hemostasis during surgical procedures. Biodegradation of Surgicel begins within 24-48 hours and is completed in as early as 1-2 weeks [1]. Perhaps for this reason, there is a paucity of literature regarding its radiologic appearance, particularly on ultrasound, as computed tomography (CT) is often the preferred imaging modality in the immediate postoperative period.
We present the CT and ultrasound appearance of Surgicel used during ovarian cystectomy of a 21-year-old patient presenting with postoperative pelvic pain.
Case report
A 21-year-old woman presented to the emergency department with suprapubic and pelvic pain. At presentation, the patient was afebrile with a normal white blood cell count and benign physical examination. Seven days before presentation, she had undergone laparoscopy and right ovarian cystectomy for a large symptomatic ovarian cyst. A CT scan of the abdomen and pelvis performed in the emergency department with oral and intravenous contrast revealed a small collection in the right adnexal surgical bed containing minute foci of gas (Fig. 1). A pelvic ultrasound was performed on the same night, demonstrating a 3.3 × 1.3 × 1.6 cm echogenic mass in the right ovary associated with “dirty” posterior acoustic shadowing (Fig. 2). There was no blood flow within the mass on color Doppler ultrasound although blood flow to the remainder of the right ovary was preserved. The uterus and left ovary appeared normal, and there was no pelvic free fluid.
Fig. 1.

Initial computed tomography of abdomen/pelvis demonstrates a small right adnexal collection containing minute foci of gas (annotated by the white arrow).
Fig. 2.
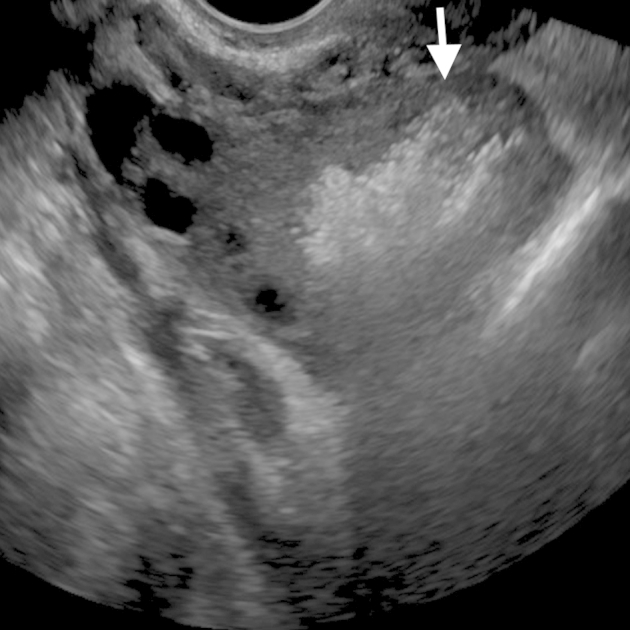
Initial pelvic ultrasound obtained within 3 hours of the computed tomography shows an echogenic mass in the right ovary with “dirty” posterior acoustic shadowing (annotated by the white arrow).
The initial differential diagnosis included postsurgical changes, ovarian torsion, or gas-containing postoperative abscess. A detailed review of the operative report revealed that a small piece of Surgicel had been placed over the cyst wall surface of the right ovary during her cystectomy. Both the CT and pelvic ultrasound findings were felt to be attributable to the postoperative appearance of Surgicel. The patient was managed conservatively and discharged home from the emergency department. Follow-up pelvic ultrasound performed 33 days after her initial surgery demonstrated resolution of the echogenic mass within the right ovary (Fig. 3).
Fig. 3.

Follow-up pelvic ultrasound performed 33 days after the initial surgery shows complete resolution of the echogenic mass within the right ovary.
Discussion
Given the importance of control of bleeding during surgery, use of topical hemostatic agents has become widespread and continues to evolve. Surgicel is a hemostatic agent commonly used in gynecologic and pelvic surgery. It is readily available and relatively inexpensive. It can easily be brought into the peritoneal cavity via laparoscopy trocars, making it compatible with minimally invasive surgery. It is then placed directly onto the tissue where assurance of hemostasis is desired. Surgicel is believed to achieve hemostasis through multiple mechanisms including activation of the intrinsic coagulation pathway, creation of a low pH environment to promote vasoconstriction, and formation of a scaffold for the establishment of a platelet plug [1], [2]. Despite their widespread use, the imaging appearances of topical hemostatic agents remain underreported in radiologic literature, perhaps owing to their limited durability (and therefore limited imaging), the diversity of hemostatic formulations, and the breadth of surgeries and anatomic locations in which they are used [3].
On postoperative CT scan, Surgicel (oxidized regenerated cellulose) has been described as a heterogeneous mass or collection containing small locules of gas, potentially leading to the misdiagnosis of abscess and subsequent futile attempts at drainage [4], [5]. There have been few reports on the imaging appearance of Surgicel on ultrasound. In our case, the sonographic appearance of Surgicel as a highly echogenic mass demonstrating posterior shadowing and reverberation is consistent with prior descriptions and is felt to be secondary to small trapped air bubbles [6]. Although Surgicel can be quickly resorbed, it may persist for 4-8 weeks in the body and even years after the initial surgery [7].
The reported case is unique given the location of Surgicel in the ovary and the inclusion of sonographic findings. A previous report of a foreign-body granulomatous reaction to Surgicel mimicking an ovarian mass described only histologic findings [8]. Behbehani and Tulandi [5] reported the CT appearance of intrapelvic Surgicel after gynecological surgery, but none of the cases had ultrasound correlates or involved the intraovarian placement of Surgicel. The combination of CT and ultrasound imaging findings in this patient was consistent with the history of Surgicel utilization during pelvic surgery. An abscess was felt to be unlikely given the lack of concerning clinical and laboratory findings. Ovarian torsion, although initially a diagnostic consideration, was excluded based on the lack of associated imaging features such as abnormal ovarian location, asymmetric enlargement of the ovary, peripheralization of the follicles, or absence of vascular flow on color Doppler ultrasound [9]. Familiarity with the patient's surgical history prevented additional costs and risks to the patient associated with unnecessary work-up and procedures.
In conclusion, knowledge of the utilization and imaging appearance of Surgicel is important for the radiologist interpreting ultrasound and CT imaging performed after pelvic surgery to prevent erroneous diagnosis of abscess and avoid unnecessary interventions.
Footnotes
Competing Interests: The authors have declared that no competing interests exist.
References
- 1.Albala D. Biosurgicals and Hemostasis. Global Robotics Institute. http://www.globalroboticsinstitute.com/sites/default/files/protected_files/Tools%20for%20Hemostasis.pdf. Accessed 21 Jan 2015.
- 2.Keshavarzi S., MacDougall M., Lulic D., Kasasbeh A., Levy M. Clinical experience with the Surgicel family of absorbable hemostats (oxidized regenerated cellulose) in neurosurgical applications. Wounds. 2013;25(6):160–167. [PubMed] [Google Scholar]
- 3.Achneck H., Sileshi B., Jamiolkowski R., Albala D., Shapiro M., Lawson J. A comprehensive review of topical hemostatic agents: efficacy and recommendations for use. Ann Surg. 2010;251(2):217–228. doi: 10.1097/SLA.0b013e3181c3bcca. [DOI] [PubMed] [Google Scholar]
- 4.Young S.T., Paulson E.K., McCann R.L., Baker M.E. Appearance of oxidized cellulose (Surgicel) on postoperative CT scans: similarity to postoperative abscess. Am J Roentgenol. 1993;160:275–277. doi: 10.2214/ajr.160.2.8424333. [DOI] [PubMed] [Google Scholar]
- 5.Behbehani S., Tulandi T. Oxidized regenerated cellulose imitating pelvic abscess. Obstet Gynecol. 2013;121(2):447–449. doi: 10.1097/aog.0b013e318276ce3f. [DOI] [PubMed] [Google Scholar]
- 6.Melamed J.W., Paulson E.K., Kliewer M.A. Sonographic appearance of oxidized cellulose (Surgicel): pitfall in the diagnosis of postoperative abscess. J Ultrasound Med. 1995;14(1):27–30. doi: 10.7863/jum.1995.14.1.27. [DOI] [PubMed] [Google Scholar]
- 7.Ibrahim M.F., Aps C., Young C.P. A foreign body reaction to Surgicel® mimicking an abscess following cardiac surgery. Eur J Cardiothorac Surg. 2002;22(3):489–490. doi: 10.1016/s1010-7940(02)00328-7. [DOI] [PubMed] [Google Scholar]
- 8.Gao H.W., Lin C.K., Yu C.P., Yu M.S., Chen A. Oxidized cellulose (Surgicel) granuloma mimicking a primary ovarian tumor. Int J Gynecol Pathol. 2002;21(4):422–423. doi: 10.1097/00004347-200210000-00015. [DOI] [PubMed] [Google Scholar]
- 9.Chang H.C., Bhatt S., Dogra V.S. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics. 2008;28(5):1355–1368. doi: 10.1148/rg.285075130. [DOI] [PubMed] [Google Scholar]