
Fig. 1.
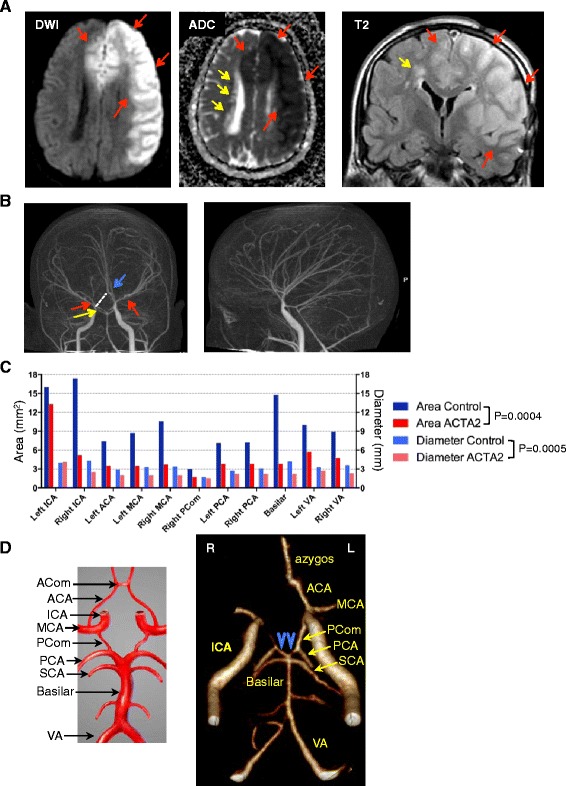
Radiologic characteristics of ARCD. a. MRI axial diffusion weighted image (DWI) and corresponding apparent diffusion coefficient (ADC) map, and coronal T2W-FLAIR image showing acute infarct with restricted diffusion involving the territories of the left MCA and bilateral ACAs (red arrows). Chronic periventricular leukoencephalopathy (yellow arrows) appears with hyperintensity on FLAIR images and increased diffusivity on ADC map. b. CT angiography demonstrating the straight course of most of the intracranial arteries, as well as lack of basal collaterals, which are typically seen in MMD. Narrowing of the supraclinoid segment of right ICA (yellow arrow) and bilateral MCAs (red arrows), and the azygos configuration of the A2 segment of ACA (blue arrow) are also shown. The missing right ACA A1 segment is indicated by a punctuated line and explains involvement of bilateral ACA territories with a left ICA occlusion. c. In vivo lumen diameter and area measurements by CT angiography (see also Additional file 1: Figure S1). The arterial measurements are compared to a normal age and gender-matched control. No left posterior communicans artery (PCom) was identified for the control. Control and mutant datasets are compared by two-way ANOVA. d. The configuration of the circle of Willis in the ARCD patient shows a combination of anatomic variants in both the anterior – lack of A1 of right ACA and common anterior azygos trunk- and posterior parts - “fetal-type” variant of PCAs with hypoplastic P1 segments (blue arrowheads). A drawing depicting the circle of Willis is shown for comparison