
Figure 2.
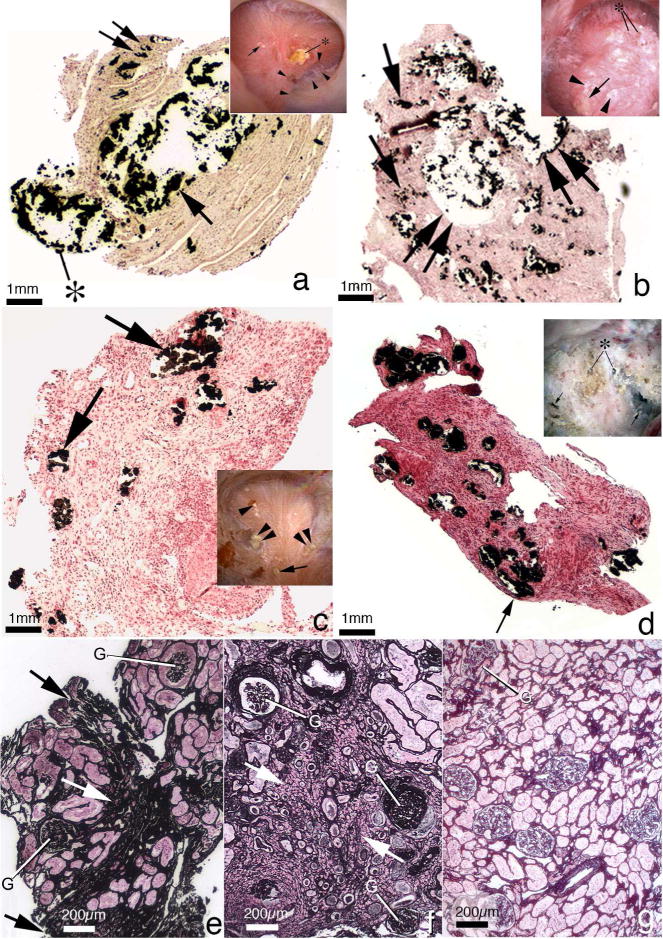
Histopathology of renal papilla and cortex from apatite and brushite stone formers. Panel A is a low magnification light microscopic image of a renal papilla from a brushite stone former showing an enormous amount of Yasue-positive deposits (arrow) filling a grossly dilated IMCD and BD. The crystalline material is protruding (asterisk) from the dilated opening of a BD. Sites of interstitial plaque are noted through out papilla (double arrow). Insert to panel A shows endoscopic view of papillum from brushite patients characterized by areas of white plaque (arrows), yellowish crystalline material protruding from dilated BD (asterisk), pitting (arrowheads) and sites of yellow plaque. Panel B is a histologic section from an apatite stone former with large fields of interstitial plaque termed “novel interstitial plaque structures” (NIPS, arrows) located near greatly dilated IMCD and BD filled with Yasue-positive deposits (double arrows) which are hydroxyapatite. Extensive regions of interstitial fibrosis surround the dilated IMCD and NIPS. The insert in panel B shows endoscopic view of a papilla from an apatite stone former characterized by sites of white plaque (arrowheads), protruding plugs for dilated opening of BD (asterisk) and an occasional site of yellow plaque (arrow). Panel C is a histologic section from a patient with primary hyperparathyroidism with stones. These patients show numerous IMCD with apatite plugs (arrows), extensive interstitial fibrosis at sites of intraluminal plugs and areas of interstitial plaque. The insert in panel C shows an endoscopic view of a papilla from a patient with primary hyperparathyroidism characterized by attached stone to white plaque, sites of yellow plaque (double arrows), interstitial plaque (arrowhead), and dilated BD with protruding plug (double arrowhead). Panel D is a histologic section from a patient with distal renal tubular acidosis presenting with diffuse IMCD plugging (arrows), severe and diffuse interstitial fibrosis and little to no interstitial plaque. The insert to panel D shows endoscopic view of a papilla from a patient with distal renal tubular acidosis characterized extensive papillary damage with retraction, loss of normal architecture, multiple dilated BD that produce a pitted appearance (arrows), some with protruding mineral deposits (asterisks) and a whitish thickened membrane appearance. Panel E shows a cortical biopsy from an apatite stone former revealing a moderate level of interstitial fibrosis (arrow) and glomerular (G) changes while panel F shows a severe level of interstitial fibrosis (arrow) and glomerular (G) change in a brushite stone former. Panel H shows a cortical biopsy from a patient with distal renal tubular acidosis revealing only a minimal level of change.