
Figure 1.
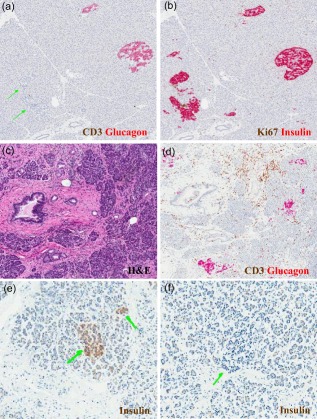
Largely unrecognized pathological features of the endocrine and exocrine pancreas in human type 1 diabetes (T1D). A common but widely underappreciated feature of endocrine pancreatic pathology in T1D involves lobular variance in the presence of (a) glucagon‐positive islets (i.e. devoid of insulin; indicated by double green arrows) versus (b) islets that contain both insulin‐ and glucagon‐positive cells. In this case (nPOD 6195), regions in close proximity clearly demonstrate such marked differences, as determined by the immunohistochemistry of adjacent pancreatic sections with anti‐glucagon and anti‐insulin antibodies, as described 23. A second characteristic involves features of the exocrine pancreas. This case (nPOD 6240) demonstrates, via standard haematoxylin and eosin (H&E), (c) fibrosis as well as (d) focal pancreatitis and peri‐ductal inflammation (determined by immunohistochemisty with anti‐glucagon and anti‐CD3 antibodies, as described 23). Finally, for many years it was presumed that the pancreas of patients with T1D with long‐standing disease was devoid of beta cells, but recent evidence suggests otherwise. The pancreas of many patients contain (e) insulin‐positive cells observed as small clusters or single cells (double green arrows), as well as (f) islets devoid of insulin (single green arrow) for years to decades following the diagnosis of T1D. Shown herein is a pancreatic section of a 60 year‐old patient with T1D (nPOD 6042) with disease duration of 59 years. Once again, expression was determined by immunohistochemistry 23. Photomicrographs courtesy of Dr Martha Campbell‐Thompson.