
Figure 2.
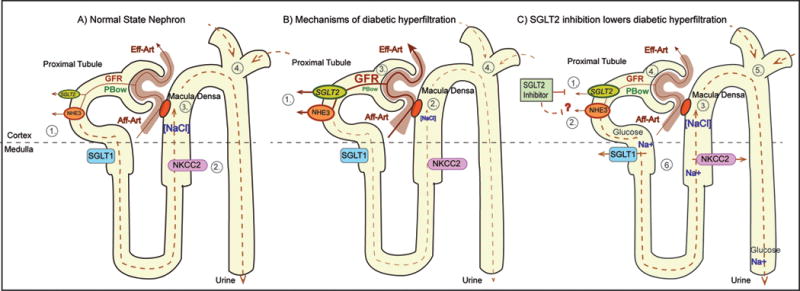
The tubular hypothesis of diabetic glomerular hyperfiltration: effect of SGLT2 inhibition. Panel A) 1. Glucose reabsorption occurs via SGLT2 in early proximal tubule (PT) and to a small degree via SGLT1 in late PT; Na+ is reabsorbed via NHE3. 2. NaCl is reabsorbed via NKCC2 in thick ascending limb (TAL). 3. Luminal NaCl concentration at macula densa ([NaCl]) inversely regulates GFR via tubuloglomerular feedback (TGF). 4. Fluid delivery to distal tubule (site of main tubular resistance) is proportional to hydrostatic pressure in Bowman space (PBow) which imposes inhibitory influence on GFR. Panel B) 1. Hyperglycemia and tubular growth increase Na+/ glucose reabsorption via SGLT2 and SGLT1 and increase Na+ reabsorption via NHE3. 2. & 3. This lowers [NaCl] at macula densa and increases GFR via TGF. 4. The hyperreabsorption also decreases fluid delivery to distal tubule which reduces PBow and increases GFR. Panel C) 1. & 2. SGLT2 inhibitor blocks Na+/ glucose reabsorption via SGLT2 and potentially inhibits NHE3. 3. & 4. This increases [NaCl] at the macula densa and lowers GFR via TGF. 5. Inhibition of hyperreabsorption increases fluid delivery to distal tubule which increases PBow and lowers GFR. 6. In addition, SGLT2 inhibition increases load to and Na+ reabsorption via SGLT1 and NKCC2 in outer medulla. This may enhance medullary hypoxia unless counterbalanced by GFR reduction.