
Figures 1.
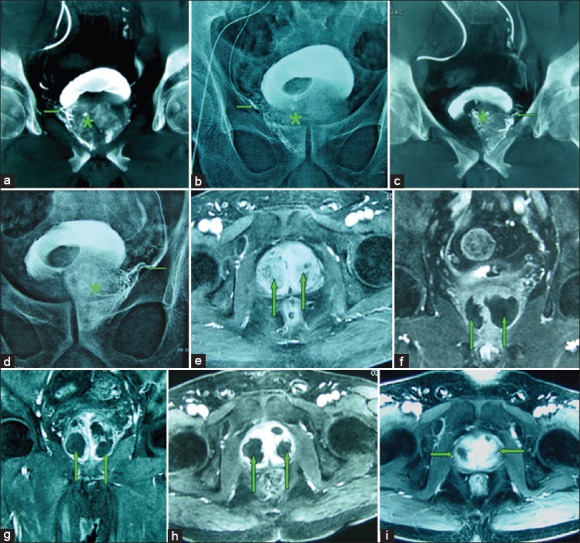
(a-i) Images from an 82-year-old man with significant lower urinary tract symptoms due to large benign prostatic hyperplasia (BPH) (100 cm3) underwent bilateral prostatic artery embolization (PAE). (a) Cone-beam computed tomography (CT) image with coronal view after super-selective catheterization of the right prostatic artery (→) demonstrates contrast medium staining in the right prostate lobe (*). (b) Image obtained at the end of embolization shows complete embolized of the right prostatic artery (→) and the right prostatic lobe opacification (*). (c) Cone-beam CT image with coronal view after super-selective catheterization of the left prostatic artery (→) demonstrates contrast medium staining in the left prostate lobe (*). (d) Image obtained at the end of embolization shows complete embolized of the left prostatic artery (→) and the left prostatic lobe opacification (*). (e) Axial contrast-enhanced T1-weighted magnetic resonance image (MRI) obtained before PAE shows a large BPH (straight arrows). (f) Coronal contrast-enhanced T1-weighted MRI obtained at 1-month after PAE shows significantly infarct areas (85%) on the both side of the prostate (straight arrows). (g) Axial contrast-enhanced T1-weighted MRI obtained at 3-month after PAE shows significantly infarct areas on the both side of the prostate (straight arrows), with the volume reduction of 32%. (h) Axial contrast-enhanced T1-weighted MRI obtained at 6-month after PAE shows significantly infarct areas on the both side of the prostate (straight arrows), with the volume reduction of 45%. (i) Axial contrast-enhanced T1-weighted MRI obtained at 12-month after PAE shows the prostate volume reduction of 46%; this patient experienced marked clinical improvement during 18-month follow-up, with International Prostate Symptom Score improvement of 80%.